

Abstract
Indications for botulinum toxin type A have been constantly evolving, and it can currently be used in virtually any area of the face and neck. The authors present their experience with this neurotoxin in treating the platysmal bands and depressor anguli oris muscle with the purpose of cosmetically improving the anterior neck and lifting the oral commissure.
Keywords: Botulinum toxin type A, mouth, neck, platysma, rejuvenation
INTRODUCTION
The shape, position, and size of the mouth are fundamental elements for the beauty and harmony of the face. The appearance, orientation, and position of the commissure of the lips, as well as its relation to the rest of the anatomic structures of the face may denote youth, aging, or sadness. Similar to the mouth, the cervical region also plays an important role in facial harmony and youth. Laxity of the skin and deep structures, submental or subplatysmal lipodystrophy, vascular alterations, skin aging, and marked bands of the platysma muscle, when associated with perioral aging and ptosis of the corner of the mouth, may all lead to a further aged face and neck. There are manifold surgical and nonsurgical resources which aim at improving this region, and each technique has its own indication criteria and varied outcomes. The main techniques used in this region of the face are the rhytidectomy and the filling of wrinkles, lips, vermillion, and commissures with temporary or permanent products as well as the various types of laser and peeling procedures.[1]
The application of botulinum toxin A (BoNT/A) in the cervical or oral region has been described by several authors. In 1998, Brandt and Bellman reported on the treatment of the aged neck with this exotoxin.[2] Carruthers and Carruthers suggested that BoNT/A can be applied directly into the depressor anguli oris muscle.[3–5] In 1999 and 2000, Goldman reported on his experience with the application of the toxin in facial wrinkles and in platysmal bands.[6–10] Also in 1999, Kane[11] and Matarasso and coworkers[12,13] described the use of BoNT/A for cosmetic outcomes in the anterior cervical region.
Herein, the authors suggest and discuss that, in selected cases and as a nonsurgical option, the combined treatment of platysmal bands and the depressor anguli oris muscle with the application of BoNT/A not only improves the appearance of the neck, but also lifts the corner of the mouth.
OBJECTIVES
This study aims at demonstrating the use of BoNT/A to improve the bands of the platysma muscle and redefine oral commissures.
Anatomy and physiology of the platysma muscle and the depressor anguli oris muscle
The platysma muscle originates in the superficial fascia of the upper portion of the thorax, clavicle, and acromion. Its posterior fibers are inserted into the depressor anguli oris and risorius muscles as well as into the lateral portion of the orbicularis oris muscle. The platysma retracts and depresses the angle of the mouth. The anterior fibers are inserted into the periosteum of the medial portion of the mandibular border. These fibers interface those of the masseter, buccinator, and depressor anguli oris. Superficial platysmal fibers can insert directly into masseter, risorius and depressor anguli oris. It is mainly these anterior portions that are responsible for the formation of platysmal bands when muscular contraction occurs.[14]
The depressor anguli oris muscle arises from the oblique line of the mandible. It is inserted within the inferior aspect of the mouth and interfaces the adjacent muscles. It lowers the commissure of the mouth, which, in turn, generates an expression of sadness or frustration. Together with the mandibular ligament, it is involved in the formation of the mentolabial fold.[15,16]
Physiopathology of the platysmal bands and ptosis of the oral commissure
The main determining factors of the aging neck are the presence of submental fat, loss of definition of the mandibular border and neck angle, flaccidity and poor quality of the skin as well as horizontal lines and vertical bands of the platysma muscle. These bands are mainly determined by hyperkinetic activity and loss of muscle tone.[17] This hyperkinetic activity of the platysma muscle and its interfaces as well as its connections with adjacent oral muscles combined with the function of the depressor anguli oris lead to marked bands and depressed oral commissures, which are also aspects commonly associated with aging.[16]
Indication
The technique is indicated for patients with horizontal and vertical platysma muscle bands and with downturned oral commissures, without excessive skin laxity or submental lipodystrophy. Patients with unrealistic expectations regarding results are to be excluded from the treatment. BoNT/A is contraindicated for pregnant and lactacting women. Similarly, it is contraindicated in patients with neuromuscular alterations, a history of allergy to any of the components of the drug, infectious disease in the area of the application, or active herpes. Finally, caution should be excercised while injecting BoNT/A to those taking aminoglycosides.[18]
METHODS
Given that the muscles to be treated are those involved in facial expression, function and mimicry, it is vital that the patients should receive proper counseling with detailed mention of expected outcomes, duration, risks, and limitations. Pretreatment photographic documentation and an informed consent form must be part of treatment routine.
This paper was developed on the basis of the use of BoNT/A (Botox®, Allergan; Dysport®, Ipsen®; Xeomin, Merz®). A detailed description of these products can be found elsewhere.[19] Two types of dilutions are used; one being a less concentrated one and having a greater volume of saline solution per unit of drug and another one is more concentrated (i.e. 3 ml NaCl or 1.5 ml per vial Botox®, respectively). The more diluted one is used in the treatment of the platysma and the more concentrated one, using less volume (lower risk of drug diffusion), is used in the depressor anguli oris. A careful assessment of the muscles, both at rest and in action is carried out prior to the application of the drug in order to identify the location, intensity, symmetry, and extent of the muscle bands, the presence and orientation of the wrinkles and lines, and the appearance of the mouth and position of the oral commissures. With the patient in the supine position, the injections are administered utilizing a thin needle (30 G ½ inch) attached to an insulin-type syringe. The procedure is usually performed without anaesthesia though a topical anesthetic may be used in patients who are more sensitive to pain. Application of cold compresses before and shortly after injection improves convenience. Next, the physician administers three or four injection sites with approximately 5 U (Botox®and Xeomin®) or 15 U (Dysport®) in 0.1 mL physiological sodium chloride solution each on both sides of the medial portion of the platysma muscle. In some cases, the small bands and more lateral wrinkles of the muscle are also treated with a few additional units of the toxin. The depressor anguli oris muscles are treated bilaterally with a single injection of approximately 2-5 U (Botox® and Xeomin®) or 6-15 U (Dysport®) in each muscle. The total dose varies according to the areas to be treated, following the pretreatment clinical assessment of each patient's muscle tone and activity and facial mimicry, the latter being the most important parameter. It is important to recognize asymmetries in rest and motion. We do not recommend any special care or bandages after treatment as we believe that the outcomes and possible complications are more closely related to the technique itself and to the doses used than to the care that follows the injection of the drug. The combination of this technique with temporary fillers probably prolongs their lasting effect.[10]
RESULTS
The results obtained, namely the attenuation of the platysmal bands and elevation and redefinition of the angle of the mouth, become visible within 2 or 3 days following the injection and remain stable for a variable period of time. The effect is longer lasting in the neck region (4 months on average) than in the oral region (approximately 3 months), probably due to the lower dosing and particular physiological characteristics of this muscle group. Although the results can be better appreciated during movements of expression and facial animation, they can also be seen in the face and neck at rest [Figures [1–6]. The best results are observed in younger patients who have greater muscular strength and no significant laxity or submental lipodystrophy.
Figure 1.

(a) Patient with marked bands of the platysma muscle and ptosis of the oral commissure. (b) After BoNT/A treatment, the attenuation of the bands and the elevation and new orientation of the oral commissure can be observed
Figure 6.
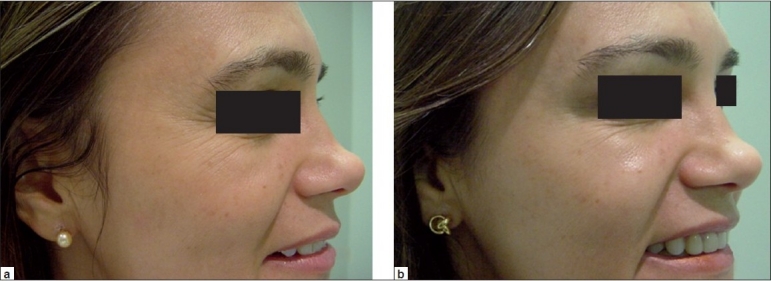
(a) Patient smiling, revealing the downturn of the oral commissure. (b) Noticeable elevation of the angle of the mouth and improvement of the smile after application of BoNT/A in the depressor muscles
Figure 2.
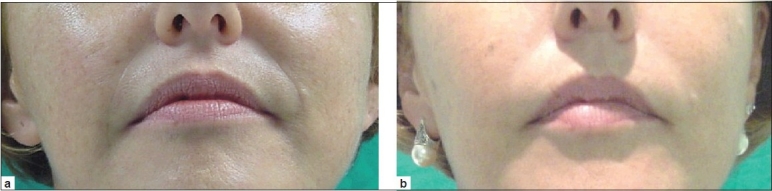
(a) Same patient as previous figure. (b) Elevation of the corner of the mouth after the application of BoNT/A
Figure 3.
(a) Inferior orientation of the angle of the mouth. (b) A change in expression and orientation of the mouth can be observed after BoNT/A
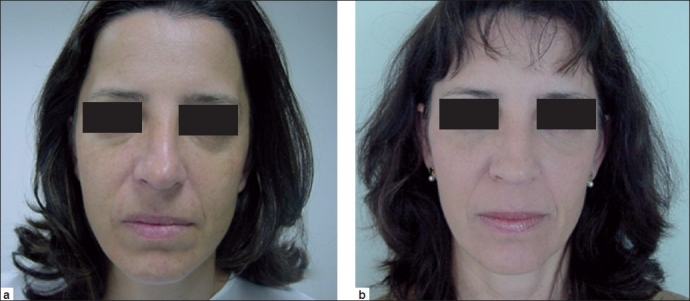
Figure 4.
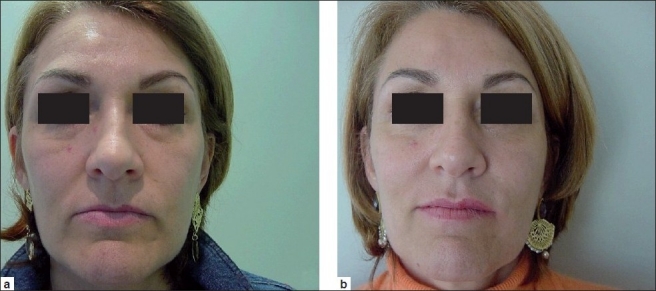
(a) Patient with hypotrophy of the upper vermillion border, marked grooves and downturn of the corner of the mouth. (b) Improvement after injection of BoNT/A into the platysma and depressor anguli oris muscles and a plasmagel filling of the grooves and vermillion border
Figure 5.

(a) Downturn of the oral commissure and hypotrophy of the upper lip vermillion border. (b) Comparative appearance after the treatment with BoNT/A for mouth lift
The results are more evident when the toxin is injected in conjunction with traditional techniques such as fillers, chemical peelings, laser procedures (ablative or nonablative and fractioned), or dermabrasion. In patients older than 60 years of age, lengthening of the philtrum may occur. It has to be corrected before BoNT/A to obtain an optimum result since otherwise the dropping of the central part of the upper lip could be aggravated.[20]
The only adverse effects observed were stinging at the injection site and discrete asymmetries and ecchymosis. Neither increase in neck laxity nor inadequate occlusion of the mouth was observed.
DISCUSSION
The use of and new indications for BoNT/A have been increasing over the past years, and it is the most frequent nonsurgical procedure performed now a days.[21] The demand for less invasive treatments that provide quick recovery and more predictable and safer outcomes is ever more frequent. Understanding and mastering anatomy and the function of facial and neck muscles as well as the balance of forces involved therein are crucial to reach effective outcomes while preserving natural facial expression, mainly because this therapy leads to muscular paralysis, even if only temporarily. In this region, antagonism to the platysma and the depressor anguli oris takes place mainly by means of the levator anguli oris and the zygomatic major and minor muscles. Thus, relaxing those depressor muscles may lead to the elevation of the corner of the mouth precisely through their antagonists, namely the levator anguli oris which end up having less opposition to their movement. Paralyzing an entire muscle group, in most cases, is unwanted and should be avoided so as to prevent the risk of generating stigmas or lack of facial expression in animation.[14–17]
A common complaint when patients present for facial rejuvenation is the expression of sadness or discontentment which is made evident by the downturn of the corner of the mouth. The use of BoNT/A in the treatment of the aged neck and depressed corner of the mouth does not present the same risks involved in surgical treatments, even though it requires that the toxin is to be re-administered after a given period. Furthermore, it is easily applied and can be performed as an outpatient procedure, which enables patients to return immediately to their regular activities. The procedure offers predictable and replicable outcomes with few risks and little discomfort.
Other treatment options or the combined use of this toxin with other traditional techniques should be considered in cases involving patients with significant cervicofacial laxity, advanced age, photoaging of the region, highly marked wrinkles, large amounts of submental fat, or significant muscular impairment.[1,21]
In selected cases, careful and judicious adjuvant treatment using the toxin in other muscles involved in facial animation may improve outcomes. It is possible to combine the application in selected muscles by injecting the drug into the orbicularis oris, risorius and zygomatic muscles, the levator labii superioris alaeque nasi muscle, the depressor septi nasi and the depressor labii inferioris (or quadratus labii inferioris), among others. However, physicians must bear in mind that some of these muscles have antagonistic movements to those in the lower third of the face. Thus, the synergistic and antagonistic activity of these muscle groups must be fully understood and assessed thoroughly prior to treatment.[1]
In the case of prominent nasolabial folds contributing to the expression of sadness, a “liquid lift” can be combined with our technique. Here, a deep subdermal deposit of monophasic hyaluronic acid filler can be placed in close proximity to the cheek bone to obtain a midface lift.[18,20]
The technique described herein differs from what has been described by Levy as “Nefertiti lift,” where BoNT/A is injected along and under each mandible and to the upper part of the platsymal band for a total of 15-20 U (Vistable®/Botox®) for re-contouring of the jaw line.[22]
New fillers, lipotransfer, and the potential uses of stem cells, the clinical application of the tetanus toxin, the evolution of videosurgery and laser technologies and new indications in the use of BoNT/A toxin today represent a new perspective in the treatment of the aged neck and face.[23] The development of new serotypes of this toxin, new commercial preparations with different dosing and advances in the modification of the protein structure of the drug all point toward a broader and safer use of BoNT/A in medicine in the near future.
CONCLUSION
In selected cases, the use of BoNT/A represents an alternative, effective and safe nonsurgical option in the treatment of the platysma muscle bands and in redefining the oral commissures. The technique can be used as an isolated procedure or in combination with other treatments.
When indications meet careful criteria and good sense, this technique offers predictable and replicable results with minimal risks and little discomfort.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Carruthers JD, Glogau RG, Blitzer A. Advances in facial rejuvenation: Botulinum toxin type A, hyaluronic acid dermal fillers, and combination therapies - consensus recommendations. Plast Reconstr Surg. 2008;121:5S–36S. doi: 10.1097/PRS.0b013e31816de8d0. The Facial Aesthetics Consensus Group Faculty. [DOI] [PubMed] [Google Scholar]
- 2.Brandt FS, Bellman B. Cosmetic use of botulinum A exotoxin for the aging neck. Dermatol Surg. 1988;24:1232–4. doi: 10.1111/j.1524-4725.1998.tb04103.x. [DOI] [PubMed] [Google Scholar]
- 3.Carruthers J, Carruthers A. Clinical indications and injection technique for the cosmetic use of botulinum A exotoxin. Dermatol Surg. 1988;24:1189–94. doi: 10.1111/j.1524-4725.1998.tb04097.x. [DOI] [PubMed] [Google Scholar]
- 4.Carruthers J, Carruthers A. Botox treatment for expressive facial lines and wrinkles. Curr Opin Otolaryngol. 2000;8:357–61. [Google Scholar]
- 5.Carruthers J, Carruthers A. Botox use in the mid and lower face and neck. Semin Cutan Surg. 2001;20:85–92. doi: 10.1053/sder.2001.25139. [DOI] [PubMed] [Google Scholar]
- 6.Goldman A. Toxina botulínica na cirurgia plástica: Indicações e experiência em 1200 áreas tratadas. Rev Soc Bras Cir Plast. 1999;14:21. [Google Scholar]
- 7.Goldman A. Tratamento das bandas platismais com toxina botulínica tipo A. Arq Cat Med. 2000;29:67–9. [Google Scholar]
- 8.Goldman A. Platysmal bands. In: Hexsel D, Trinidade de Almeida A, editors. Cosmetic Use of Botulinum Toxin. Sao Paulo: AGE Editoria; 2002. pp. 173–7. [Google Scholar]
- 9.Goldman A. Treatment of facial paralysis and asymmetry. In: Hexsel D, Trinidade de Almeida A, editors. Cosmetic Use of Botulinum Toxin. Sao Paulo: AGE Editoria; 2002. pp. 187–91. [Google Scholar]
- 10.Goldman A. Combining procedures with botulinum toxin in plastic surgery. In: Hexsel D, Trinidade de Almeida A, editors. Cosmetic Use of Botulinum Toxin. Sao Paulo: AGE Editoria; 2002. pp. 216–20. [Google Scholar]
- 11.Kane MA. Nonsurgical treatment of platysma bands with injections of botulinum toxin A. Plast Reconstr Surg. 1999;103:656–63. doi: 10.1097/00006534-199902000-00045. [DOI] [PubMed] [Google Scholar]
- 12.Matarasso A. Botulinum A exotoxin for the management of platysma bands. Plast Reconstr Surg. 1999;103:645–52. doi: 10.1097/00006534-199902000-00043. [DOI] [PubMed] [Google Scholar]
- 13.Matarasso SL, Matarasso A. Treatment guidelines for botulinum toxin type A for periocular region and a report on partial upper lip ptosis following injections to the lateral canthal rhytids. Plast Reconstr Surg. 2001;108:208–14. doi: 10.1097/00006534-200107000-00033. [DOI] [PubMed] [Google Scholar]
- 14.Thiel W. 2nd ed. Heidelberg: Springer; 2005. Photographischer Atlas der Praktischen Anatomie. [Google Scholar]
- 15.Kane MA. The functional anatomy of the lower face as it applies to rejuvenation via chemodenervation. Facial Plast Surg. 2005;21:55–64. doi: 10.1055/s-2005-871764. [DOI] [PubMed] [Google Scholar]
- 16.Perkins SW, Sandel HD. Anatomic considerations, analysis, and the aging process of the perioral region. Facial Plast Surg Clin North Am. 2007;15(5):403–7. doi: 10.1016/j.fsc.2007.08.006. [DOI] [PubMed] [Google Scholar]
- 17.DeCastro CC. The anatomy of the platysma muscle. Plast Reconst Surg. 1980;66:681–3. [Google Scholar]
- 18.Wollina U, Rowland Payne C. Aging well: The role of minimally invasive aesthetic dermatological procedures in women over 65. J Cosmet Dermatol. 2010;9:50–8. doi: 10.1111/j.1473-2165.2010.00475.x. [DOI] [PubMed] [Google Scholar]
- 19.Carruthers A, Carruthers J. Botulinum toxin products overview. Skin Therapy Lett. 2008;13:1–4. [PubMed] [Google Scholar]
- 20.Wollina U. Botulinum toxin: Mechanism of action and possible noncosmetic indications. J Cutan Aesthet Surg. 2008;1:1–4. doi: 10.4103/0974-2077.41148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Wollina U. Liquid-Lift. Face - Int Mag Orofac Esthet. 2008;2:40–1. [Google Scholar]
- 22.Levy PM. The ‘Nefertiti lift’: A new technique for specific re-contouring of the jaw-line. J Cosmet Laser Ther. 2007;9:249–52. doi: 10.1080/14764170701545657. [DOI] [PubMed] [Google Scholar]
- 23.Wollina U, Goldman A, Berger U, Abdel-Naser MB. Esthetic and cosmetic dermatology. Dermatol Ther. 2008;21:118–30. doi: 10.1111/j.1529-8019.2008.00179.x. [DOI] [PubMed] [Google Scholar]