

Figure 1.
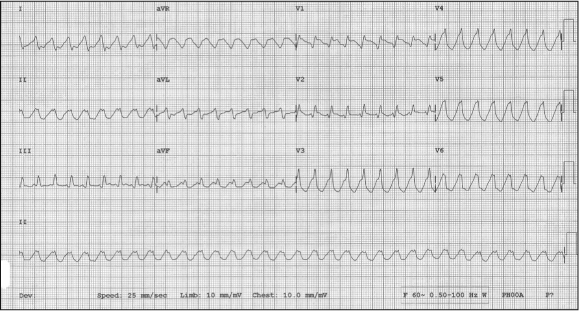
12-lead ECG from a man with a history of atrial fibrillation and dilated cardiomyopathy, age 43 years, with palpitations and shortness of breath.
Demonstrates a wide-complex, regular tachycardia with a ventricular rate of 200 beats/minute, consistent with probable monomorphic ventricular tachycardia.
Figure 2.

12-lead ECG from same patient following electrical synchronized cardioversion.
Demonstrates atrial fibrillation with a ventricularly paced rhythm at 70 beats/minute (patient had a previously placed internal pacemaker for complete heart block).
The differential diagnosis of a wide-complex regular tachycardia includes supraventricular tachycardia (SVT) with intraventricular aberrant conduction, SVT conducting to the ventricles over an accessory pathway, and ventricular tachycardia (VT).1 The ECG characteristics of VT are A) wide QRS complexes; B) rate >100 (most commonly 150–200); C) rhythm is usually regular, although there may be some beat-to-beat variation, and D) QRS axis is usually constant.2 The most common predictors of VT are ischemic heart disease, especially acute myocardial infarction and prior VT. The presence of atrioventricular dissociation can be used to exclude the diagnosis of SVT, but is often difficult to identify on ECG. Wide-complex regular tachydysrhythmias that do not show regular sinus activity should always be treated as VT; inappropriate treatment of VT as an SVT may induce hemodynamic compromise.3
References
- Antunes E, Brugada J, Steurer G, Andries E, Brugada P. The differential diagnosis of a regular tachycardia with a wide QRS complex on the 12-lead ECG: ventricular tachycardia, supraventricular tachycardia with aberrant intraventricular conduction, and supraventricular tachycardia with anterograde conduction over an accessory pathway. Pacing Clin Electrophysiol. 1994 Sep;17(9):1515–24. doi: 10.1111/j.1540-8159.1994.tb01517.x. [DOI] [PubMed] [Google Scholar]
- Hollowell H, Mattu A, Perron D, Holstege C, Brady WJ. Wide-complex tachycardia: beyond the traditional differential diagnosis of ventricular tachycardia vs supraventricular tachycardia with aberrant conduction. Am J Emerg Med. 2005 Nov;23(7):876–89. doi: 10.1016/j.ajem.2005.04.015. [DOI] [PubMed] [Google Scholar]
- Garmel GM. Wide complex tachycardias: understanding this complex condition part 2—management, miscellaneous causes, and pitfalls. West J Emerg Med. 2008 May;9(2):97–103. [PMC free article] [PubMed] [Google Scholar]