

Abstract
Background:
Traumatic unilateral facet dislocation without fracture is an uncommon injury of the lumbosacral junction. We describe a case of a unilateral perched L5–S1 facet causing axial back pain and radiculopathy provoked by motion.
Case Description:
The patient underwent reduction with complete facetectomy followed by internal fixation at L5–S1, facilitating decompression of the S1 nerve root. Postoperatively, the patient reported improvement in her pain.
Conclusions:
This injury can be recognized using subtle clues, such as transverse process fractures and/or widened posterior elements. Despite its rarity, when identified, this injury can be characterized using the new TLICS system for thoracolumbar fractures and should be managed accordingly.
Keywords: Facet dislocation, operative management, trauma
INTRODUCTION
Traumatic unilateral or bilateral facet dislocations without fracture of the cervical spine are common injuries, indicative of injury of the stabilizing ligaments, and are routinely managed with reduction and operative fixation. In contrast, facet dislocations without fracture of the lumbar spine are rare. The superior articular process may be partially or completely dislocated, and the dislocations may involve either one or both articular processes.[49] Most reported cases of this injury pattern localize to the lumbosacral junction and have been managed both conservatively and, more recently, with open reduction and fusion.[1,2,5,8,9,11] The Thoracolumbar Injury Classification and Severity (TLICS) score for thoracolumbar fractures can provide guidance.[44,45] We describe a case of a unilateral perched L5–S1 facet causing axial back pain and radiculopathy provoked by motion, discuss the literature, and explain the rationale for treatment based on the TLICS classification.
CASE DESCRIPTION
A 46-year-old woman presented in transfer from a community hospital after sustaining injuries from a motor-vehicle accident in which she was a restrained driver. During evaluation at the community hospital, no gross signs of internal or external injuries and no neurologic deficit were noted; however, the patient complained of significant pain and spasms in the lower back, worsened by an upright position. She also complained of right leg pain with a sharp quality when she would change position. Lumbar radiographs showed a potential widening of one of the L5–S1 neuroforamina [Figure 1]. Evaluation with thin-slice computed tomography (CT) with coronal and sagittal plane reconstructions demonstrated a unilateral dislocation of the right L5–S1 facet joint with a perched facet [Figure 2]. Fractures with significant diastasis of the fragments of the right L4 and L5 transverse processes were noted (not shown). Magnetic resonance (MR) imaging of the lumbar spine did not show significant disruption of the intervertebral disc; however, unilateral distraction of the disc space is visible on the CT and MR images [Figures 3 and 4]. We calculated the patient’s TLICS score to be 8, 3 points for translational/rotational injury morphology, 3 points for injured posterior ligamentous complex, and 2 points for radiculopathy.
Figure 1.

Plain lateral radiograph of the lumbar spine, demonstrating subtle widening of one of the L5–S1 neuroforamina
Figure 2.
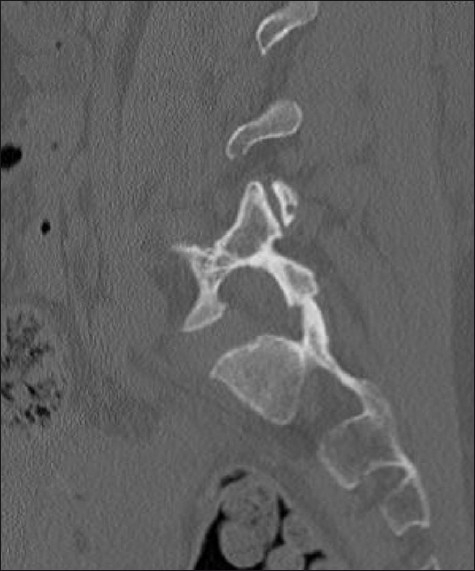
Computed tomography of the lumbar spine. Sagittal reconstruction through the perched right L5–S1 facet joint
Figure 3.

Anterior (a) and right lateral (b) views of the three-dimensional reconstruction of the computed tomography scan of the lumbar spine, demonstrating the unilateral perched facet joint and asymmetric widening of the L5–S1 disc space
Figure 4.

Coronal inversion recovery (STIR) weighted image showing edema and asymmetric widening of the L5–S1 disc space
Surgical intervention was undertaken because of the presence of clinical instability and her TLICS score. We found obvious disruption of the posterior tension band, including the interspinous ligaments between L4, L5, and S1 with associated soft tissue hematoma. After subperiosteal dissection, the naked superior articular process of S1 was visible, with the most caudal aspect of the inferior articular process of L5 lying cephalad and ventral to it, causing a clockwise rotation of L5. Reduction was accomplished with a complete facetectomy on the right followed by internal fixation with interbody graft and pedicle screw instrumentation at the L5–S1 level, facilitating complete decompression of the S1 nerve root [Figure 5]. Postoperatively, the patient reported immediate and sustained improvement in her back and leg pain. Dynamic X-rays obtained at 6 months showed no significant motion at the operated level [Figure 6].
Figure 5.

Sagittal reconstruction of the postoperative computed tomography showing the extent of resection of the articular processes and the transpedicular posterior segmental fixation on the right side. A portion of the polyetheretherketone (PEEK) interbody graft is visible
Figure 6.

Lateral flexion (a) and extension (b) radiographs of the lumbar spine demonstrating pedicle screw instrumentation and interbody graft at L5–S1 with no significant motion between flexion and extension at the instrumented level
DISCUSSION
Trauma to the lumbar spine typically results in injuries at the thoracolumbar junction. In a large series more than half of all fractures involved T12 or L1.[27] Approximately 60% were classified as compression or burst fractures resulting most often from a flexion–compression-type injury.
The diagnosis of lumbosacral dislocation may be missed because radiographs taken as part of a trauma evaluation may be inadequate to visualize an abnormal relationship of the lumbosacral facets. The presence of transverse process fractures, as seen in our case, should alert the medical team to the possibility of a more serious injury.[23,53,54] Thin-sliced CT images with sagittal and coronal reconstructions demonstrate the injury with clarity. Additionally, we found three-dimensional reconstructions particularly helpful to discern the relationship of the L5 and S1 articular processes.
For subacute dislocation, surgical treatment is complex. The reported cases treated conservatively had excellent clinical outcomes.[5,23,31,54] In contrast, the conservative treatment of acute fracture–dislocation of L5–S1 is likely ineffective because of significant instability, necessitating open reduction and internal fixation.[31]
Although our patient was neurologically intact without canal compromise, with a score of 8 on the TLICS system, optimal management of this lesion is operative reduction and fixation.[44,45] Additionally, we considered this lesion unstable according to the comprehensive definition by White and Panjabi.[52]
Lumbosacral dislocations are usually associated with high-energy trauma, and patients often suffer from associated visceral lesions, extraspinal fractures, and secondary spine fractures, including transverse process fractures in the majority.[6] Our patient suffered 2 transverse process fractures without evidence of visceral injury.
In a review of the literature on lumbosacral dislocations, we found 93 cases that were previously reported [Table 1].[1–26,28,30–43,46,48–51,53,54] Purely ligamentous injury akin to the findings in our case were less prevalent and have been reported in only a few cases.[2,42,48] Although a few cases were managed conservatively, most patients underwent open reduction and fusion, by variable approaches and fusion techniques. Primary facet dislocations involving the lumbosacral spine are rare and have been reported to occur mainly at the lumbosacral junction in association with anterior subluxation.[1,2,5,8,9,11] A case of lateral subluxation associated with a unilateral locked facet in the lumbar spine has also been reported.[29]
Table 1.
Review of the existing literature concerned with the management of lumbosacral dislocations
| Report | Number of cases | Treatment | Dislocation type | Cause |
|---|---|---|---|---|
| Dewey et al,1968[16] | 2 | Trauma | ||
| Samberg, 1975[39] | 1 | Trauma | ||
| Fardon, 1976[19] | 1 | Surgery | Trauma | |
| Newell, 1977[31] | 1 | Conservative | Trauma | |
| Jackson et al,1979[25] | 3 | Surgery | Trauma | |
| Zoltan et al,1979[54] | 1 | Unilateral | ||
| Griffin et al,1980[21] | 1 | Conservative | ||
| Das De, 1981[14] | 4 | Surgery | ||
| Morris, 1981[30] | 1 | Unilateral | ||
| Boger et al,1983[5] | 1 | Unilateral | ||
| Nicholson, 1983[32] | 1 | Surgery | Unilateral | |
| Herron et al,1984[22] | 1 | Surgery | ||
| Boyd et al,1985[7] | 1 | Conservative | ||
| Resnik et al,1985[36] | 1 | |||
| Wilchinsky, 1987[53] | 1 | |||
| Grabe, 1988[20] | 1 | Tonic-clonic seizure | ||
| Miz et al,1988[28] | 1 | Unilateral | ||
| Cohn et al,1989[10] | 1 | Bilateral | Trauma | |
| Kramer et al,1989[26] | 1 | Unilateral | ||
| Carl et al,1991[8] | 1 | Unilateral | ||
| Connolly et al,1992[11] | 4 | Surgery | Unilateral | |
| Pellise et al,1992[33] | 1 | Surgery | Unilateral | Trauma |
| Van Savage et al,1992[46] | 1 | Surgery | Unilateral | |
| Barquet et al,1993[3] | 1 | Unilateral | Trauma | |
| Davis et al,1993[15] | 1 | Surgery | Bilateral | Trauma |
| Beguiristain et al,1995[4] | 1 | Conservative | Bilateral | Trauma |
| Hilibrand et al,1995[23] | 4 | Surgery | Bilateral | Trauma |
| Fabris et al,1996[18] | 12 | Surgery | Bilateral | Pediatric, degenerative |
| Steinitz et al,1997[40] | 1 | Surgery | Bilateral | Trauma, delayed |
| Aihara et al,1998[1] | 7 | Surgery | Both | Trauma |
| Roche et al,1998[37] | 1 | Surgery | Bilateral | Trauma |
| Carlson et al,1999[9] | 2 | Surgery | Trauma | |
| Fabris et al,1999[17] | 3 | Surgery | Trauma | |
| Hodges et al,1999[24] | 1 | Surgery | Bilateral | Trauma |
| Verlaan et al,2001[48] | 1 | Surgery | Bilateral | Trauma |
| Cruz-Conde et al,2003[12] | 1 | Surgery | Bilateral | Trauma |
| Arnold et al,2004[2] | 1 | Surgery | Bilateral | Trauma |
| Boldin et al,2004[6] | 1 | Unilateral | Trauma | |
| Stuart et al,2004[41] | 1 | Unilateral | Trauma | |
| Tsirikos et al,2004[43] | 2 | Surgery | Bilateral | Trauma, delayed |
| Vialle et al,2004[51] | 4 | Surgery | Trauma | |
| Vialle et al,2005[50] | 1 | Surgery | Unilateral | Trauma |
| Reinhold et al,2006[35] | 1 | Surgery | Bilateral | Trauma |
| Saiki et al,2006[38] | 1 | Surgery | Bilateral | Trauma |
| Vialle et al,2007[49] | 11 | Surgery | Both | Trauma |
| Reddy et al,2008[34] | 2 | Surgery | Unilateral | Trauma |
| Szentirmai et al,2008[42] | 1 | Unilateral | Trauma | |
| Daniels et al,2009[13] | 1 | Surgery | Bilateral | Trauma |
In young children, this injury has been managed successfully by cast immobilization[23]; however, conservative treatment of fracture–dislocation of L5 in adolescents is generally ineffective because the lesion is considered fundamentally unstable as a result of the incurred severe bone and ligamentous damage.[6]
Unlike the lumbar facets with a relative sagittal orientation, the L5–S1 facet has a more coronal alignment.[47] Thus, the lumbosacral junction behaves similar to the cervical spine, and a unilateral perched facet implies a rotatory component.
The management of these rare injuries is still controversial. Boldin and coworkers[6] argued that open reduction and internal fixation are indicated for the management of acute lumbosacral dislocation in all but children. For open reduction, the fifth lumbar and first sacral articular processes are distracted by temporarily increasing the flexion deformity. Occasionally, disimpaction and reduction can be achieved only after partial excision of the tip of the superior facet of S1.[8,11,28] In cases of intervertebral disc derangement, anterior interbody fusion has been advocated.[1] We chose operative reduction and fixation for our patient based on the clinical instability demonstrated by severe back and radicular pain associated with motion, which resulted in improvement of her symptoms.
CONCLUSIONS
A unilateral lumbosacral facet dislocation is a rare injury that has been managed both conservatively and surgically. Transverse process fractures may point to the diagnosis of this injury, which otherwise may be missed on routine evaluation. Despite its rarity, this injury pattern fits into the categories of the Thoracolumbar Injury Classification and Severity Score (TLICS) system for thoracolumbar fractures and can be managed accordingly. Open reduction and fixation is safe and efficacious.
Contributor Information
Clemens M. Schirmer, Email: clemens.schirmer@baystatehealth.org.
Erica F. Bisson, Email: erica.bisson@hsc.utah.edu.
REFERENCES
- 1.Aihara T, Takahashi K, Yamagata M, Moriya H. fracture-dislocation of the fifth lumbar vertebra. A new classification. J Bone Joint Surg Br. 1998;80:840–5. doi: 10.1302/0301-620x.80b5.8657. [DOI] [PubMed] [Google Scholar]
- 2.Arnold PM, Malone DG, Han PP. Bilateral locked facets of the lumbosacral spine: Treatment with open reduction and transpedicular fixation. J Spinal Cord Med. 2004;27:269–72. doi: 10.1080/10790268.2004.11753761. [DOI] [PubMed] [Google Scholar]
- 3.Barquet A, Menendez J, Dubra A, Masliah R, Pereyra D. Anterolateral dislocation of the lumbosacral junction. Can Assoc Radiol J. 1993;44:129–32. [PubMed] [Google Scholar]
- 4.Beguiristain J, Schweitzer D, Mora G, Pombo V. Traumatic lumbosacral dislocation in a 5-year-old boy with eight years follow-up. Spine. 1995;20:362–6. doi: 10.1097/00007632-199502000-00020. [DOI] [PubMed] [Google Scholar]
- 5.Boger DC, Chandler RW, Pearce JG, Balciunas A. Unilateral facet dislocation at the lumbosacral junction. Case report and literature review. J Bone Joint Surg Am. 1983;65:1174–8. [PubMed] [Google Scholar]
- 6.Boldin C, Grechenig W, Fankhauser F, Sorantin E. Traumatic unilateral facet dislocation of the lumbosacral junction. Injury. 2004;35:950–2. doi: 10.1016/S0020-1383(03)00189-X. [DOI] [PubMed] [Google Scholar]
- 7.Boyd MC, Yu WY. Closed reduction of lumbosacral fracture dislocations. Surg Neurol. 1985;23:295–8. doi: 10.1016/0090-3019(85)90099-0. [DOI] [PubMed] [Google Scholar]
- 8.Carl A, Blair B. Unilateral lumbosacral facet fracture-dislocation. Spine. 1991;16:218–21. doi: 10.1097/00007632-199102000-00023. [DOI] [PubMed] [Google Scholar]
- 9.Carlson JR, Heller JG, Mansfield FL, Pedlow FX., Jr Traumatic open anterior lumbosacral fracture dislocation. A report of two cases. Spine. 1999;24:184–8. doi: 10.1097/00007632-199901150-00021. [DOI] [PubMed] [Google Scholar]
- 10.Cohn SL, Keppler L, Akbarnia BA. Traumatic retrolisthesis of the lumbosacral junction. A case report. Spine. 1989;14:132–4. doi: 10.1097/00007632-198901000-00031. [DOI] [PubMed] [Google Scholar]
- 11.Connolly PJ, Esses SI, Heggeness MH, Cook SS. Unilateral facet dislocation of the lumbosacral junction. Spine. 1992;17:1244–8. doi: 10.1097/00007632-199210000-00020. [DOI] [PubMed] [Google Scholar]
- 12.Cruz-Conde R, Rayo A, Rodriguez de Oya R, Berjano P, Garate E. Acute traumatic lumbosacral dislocation treated by open reduction internal fixation and fusion. Spine. 2003;28:E51–3. doi: 10.1097/01.BRS.0000042236.91724.56. [DOI] [PubMed] [Google Scholar]
- 13.Daniels AH, Deodhar AA, Hart RA. Traumatic spondyloptosis resulting from high-energy trauma concurrent with a tonic-clonic seizure. Spine J. 2009;9:e1–4. doi: 10.1016/j.spinee.2007.10.030. [DOI] [PubMed] [Google Scholar]
- 14.Das De S, McCreath SW. Lumbosacral fracture-dislocations. A report of four cases. J Bone Joint Surg Br. 1981;63-B:58–60. doi: 10.1302/0301-620X.63B1.7225186. [DOI] [PubMed] [Google Scholar]
- 15.Davis AA, Carragee EJ. Bilateral facet dislocation at the lumbosacral joint. A report of a case and review of literature. Spine. 1993;18:2540–4. [PubMed] [Google Scholar]
- 16.Dewey P, Browne PS. Fracture-dislocation of the lumbo-sacral spine with cauda equina lesion. Report of two cases. J Bone Joint Surg Br. 1968;50:635–8. [PubMed] [Google Scholar]
- 17.Fabris D, Costantini S, Nena U, Lo Scalzo V. Traumatic L5–S1 spondylolisthesis: Report of three cases and a review of the literature. Eur Spine J. 1999;8:290–5. doi: 10.1007/s005860050176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Fabris DA, Costantini S, Nena U. Surgical treatment of severe L5–S1 spondylolisthesis in children and adolescents. Results of intraoperative reduction, posterior interbody fusion, and segmental pedicle fixation. Spine. 1996;21:728–33. doi: 10.1097/00007632-199603150-00014. [DOI] [PubMed] [Google Scholar]
- 19.Fardon DF. Displaced fracture of the lumbosacral spine with delayed cauda equina deficit: Report of a case and review of literature. Clin Orthop Relat Res. 1976;120:155–8. [PubMed] [Google Scholar]
- 20.Grabe RP. fracture-dislocation of the lumbosacral spine during a grand mal epileptic seizure. A case report. S Afr Med J. 1988;74:129–31. [PubMed] [Google Scholar]
- 21.Griffin JB, Sutherland GH. Traumatic posterior fracture-dislocation of the lumbosacral joint. J Trauma. 1980;20:426–8. [PubMed] [Google Scholar]
- 22.Herron LD, Williams RC. fracture-dislocation of the lumbosacral spine. Report of a case and review of the literature. Clin Orthop Relat Res. 1984;186:205–11. [PubMed] [Google Scholar]
- 23.Hilibrand AS, Urquhart AG, Graziano GP, Hensinger RN. Acute spondylolytic spondylolisthesis. Risk of progression and neurological complications. J Bone Joint Surg Am. 1995;77:190–6. doi: 10.2106/00004623-199502000-00004. [DOI] [PubMed] [Google Scholar]
- 24.Hodges SD, Shuster J, Asher MA, McClarty SJ. Traumatic L5–S1 spondylolisthesis. South Med J. 1999;92:316–20. doi: 10.1097/00007611-199903000-00012. [DOI] [PubMed] [Google Scholar]
- 25.Jackson RH, Quisling RG, Day AL. Fracture and complete dislocation of the thoracic or lumbosacral spine: report of three cases. Neurosurgery. 1979;5:250–3. doi: 10.1227/00006123-197908000-00009. [DOI] [PubMed] [Google Scholar]
- 26.Kramer KM, Levine AM. Unilateral facet dislocation of the lumbosacral junction. A case report and review of the literature. J Bone Joint Surg Am. 1989;71:1258–61. [PubMed] [Google Scholar]
- 27.McAfee PC, Yuan HA, Fredrickson BE, Lubicky JP. The value of computed tomography in thoracolumbar fractures. An analysis of one hundred consecutive cases and a new classification. J Bone Joint Surg Am. 1983;65:461–73. [PubMed] [Google Scholar]
- 28.Miz GS, Engler GL. Unilateral dislocation of a lumbosacral facet. Spine. 1988;13:956–7. doi: 10.1097/00007632-198808000-00022. [DOI] [PubMed] [Google Scholar]
- 29.Mori K, Hukuda S, Katsuura A, Saruhashi Y, Asajima S. Traumatic bilateral locked facet at L4-5: Report of a case associated with incorrect use of a three-point seatbelt. Eur Spine J. 2002;11:602–5. doi: 10.1007/s00586-002-0396-8. [DOI] [PubMed] [Google Scholar]
- 30.Morris BD. Unilateral dislocation of a lumbosacral facet. A case report. J Bone Joint Surg Am. 1981;63:164–5. [PubMed] [Google Scholar]
- 31.Newell RL. Lumbosacral fracture-dislocation: A case managed conservatively, with return to heavy work. Injury. 1977;9:131–4. doi: 10.1016/0020-1383(77)90006-7. [DOI] [PubMed] [Google Scholar]
- 32.Nicholson RA. Lateral lumbosacral fracture dislocation: A case report. Injury. 1983;15:41–3. doi: 10.1016/0020-1383(83)90161-4. [DOI] [PubMed] [Google Scholar]
- 33.Pellise F, Bago J, Villanueva C. Double-level spinal injury resulting in “en bloc” dislocation of the lumbar spine. A case report. Acta Orthop Belg. 1992;58:349–52. [PubMed] [Google Scholar]
- 34.Reddy SJ, Al-Holou WN, Leveque JC, La Marca F, Park P. Traumatic lateral spondylolisthesis of the lumbar spine with a unilateral locked facet: Description of an unusual injury, probable mechanism, and management. J Neurosurg Spine. 2008;9:576–80. doi: 10.3171/SPI.2008.6.08301. [DOI] [PubMed] [Google Scholar]
- 35.Reinhold M, Knop C, Blauth M. Acute traumatic L5–S1 spondylolisthesis: A case report. Arch Orthop Trauma Surg. 2006;126:624–30. doi: 10.1007/s00402-005-0078-1. [DOI] [PubMed] [Google Scholar]
- 36.Resnik CS, Scheer CE, Adelaar RS. Lumbosacral dislocation. J Can Assoc Radiol. 1985;36:259–61. [PubMed] [Google Scholar]
- 37.Roche PH, Dufour H, Graziani N, Jolivert J, Grisoli F. Anterior lumbosacral dislocation: Case report and review of the literature. Surg Neurol. 1998;50:11–6. doi: 10.1016/s0090-3019(98)00009-3. [DOI] [PubMed] [Google Scholar]
- 38.Saiki K, Hirabayashi S, Sakai H, Inokuchi K. Traumatic anterior lumbosacral dislocation caused by hyperextension mechanism in preexisting L5 spondylolysis: A case report and a review of literature. J Spinal Disord Tech. 2006;19:455–62. doi: 10.1097/00024720-200608000-00015. [DOI] [PubMed] [Google Scholar]
- 39.Samberg LC. fracture-dislocation of the lumbosacral spine. A case report. J Bone Joint Surg Am. 1975;57:1007–8. [PubMed] [Google Scholar]
- 40.Steinitz DK, Alexander DI, Leighton RK, O’Sullivan JJ. Late displacement of a fracture dislocation at the lumbosacral junction. A case study. Spine. 1997;22:1024–7. doi: 10.1097/00007632-199705010-00016. [DOI] [PubMed] [Google Scholar]
- 41.Stuart RM, Song SJ. Unilateral lumbosacral facet joint dislocation without associated fracture. Australas Radiol. 2004;48:224–9. doi: 10.1111/j.1440-1673.2004.01303.x. [DOI] [PubMed] [Google Scholar]
- 42.Szentirmai O, Seinfeld J, Beauchamp K, Patel V. Traumatic unilateral lumbosacral jumped facet without fracture in a child - presentation of a safe treatment strategy for a rare injury. Patient Saf Surg. 2008;2:29. doi: 10.1186/1754-9493-2-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Tsirikos AI, Saifuddin A, Noordeen MH, Tucker SK. Traumatic lumbosacral dislocation: Report of two cases. Spine. 2004;29:E164–8. doi: 10.1097/00007632-200404150-00026. [DOI] [PubMed] [Google Scholar]
- 44.Vaccaro AR, Lehman RA, Jr, Hurlbert RJ, Anderson PA, Harris M, Hedlund R, et al. A new classification of thoracolumbar injuries: The importance of injury morphology, the integrity of the posterior ligamentous complex, and neurologic status. Spine. 2005;30:2325–33. doi: 10.1097/01.brs.0000182986.43345.cb. [DOI] [PubMed] [Google Scholar]
- 45.Vaccaro AR, Zeiller SC, Hulbert RJ, Anderson PA, Harris M, Hedlund R, et al. The thoracolumbar injury severity score: A proposed treatment algorithm. J Spinal Disord Tech. 2005;18:209–15. [PubMed] [Google Scholar]
- 46.Van Savage JG, Dahners LE, Renner JB, Baker CC. fracture-dislocation of the lumbosacral spine: Case report and review of the literature. J Trauma. 1992;33:779–84. doi: 10.1097/00005373-199211000-00033. [DOI] [PubMed] [Google Scholar]
- 47.Van Schaik JP, Verbiest H, Van Schaik FD. The orientation of laminae and facet joints in the lower lumbar spine. Spine. 1985;10:59–63. doi: 10.1097/00007632-198501000-00009. [DOI] [PubMed] [Google Scholar]
- 48.Verlaan JJ, Oner FC, Dhert WJ, Verbout AJ. Traumatic lumbosacral dislocation: Case report. Spine. 2001;26:1942–4. doi: 10.1097/00007632-200109010-00026. [DOI] [PubMed] [Google Scholar]
- 49.Vialle R, Charosky S, Rillardon L, Levassor N, Court C. Traumatic dislocation of the lumbosacral junction diagnosis, anatomical classification and surgical strategy. Injury. 2007;38:169–81. doi: 10.1016/j.injury.2006.06.015. [DOI] [PubMed] [Google Scholar]
- 50.Vialle R, Court C. Traumatic lateral lumbosacral dislocation: One case and review of literature. J Spinal Disord Tech. 2005;18:286–9. [PubMed] [Google Scholar]
- 51.Vialle R, Wolff S, Pauthier F, Coudert X, Laumonier F, Lortat-Jacob A, et al. Traumatic lumbosacral dislocation: Four cases and review of literature. Clin Orthop Relat Res. 2004;419:91–7. [PubMed] [Google Scholar]
- 52.White AA, Panjabi MM. 2nd ed. Philadelphia: Lippincott; 1990. Clinical biomechanics of the spine. [Google Scholar]
- 53.Wilchinsky ME. Traumatic lumbosacral dislocation. A case report and review of the literature. Orthopedics. 1987;10:1271–4. [PubMed] [Google Scholar]
- 54.Zoltan JD, Gilula LA, Murphy WA. Unilateral facet dislocation between the fifth lumbar and first sacral vertebrae. Case report. J Bone Joint Surg Am. 1979;61:767–9. [PubMed] [Google Scholar]