

Abstract
The purpose of this study was to evaluate the effectiveness of a high-probability (high-p) request sequence as a means of increasing compliance with medical examination tasks. Participants were children who had been diagnosed with autism and who exhibited noncompliance during general medical examinations. The inclusion of the high-p request sequence effectively increased compliance with medical examination tasks. In addition, the procedure was efficient, could be implemented by parents and medical professionals, and did not involve aversive procedures.
Keywords: autism, children, noncompliance, high-probability request sequence
Refusal to initiate or complete requested tasks in a specified time period is a commonly reported problem exhibited by children with autism and developmental disabilities (Lovaas, 1993). Noncompliance with medical procedures is a widespread problem, particularly among children with disabilities (McComas, Wacker, & Cooper, 1998). In some settings, this problem is addressed by employing restraint, sedation, or anesthesia (Mason et al., 2008). These methods often alter the test results and cause unnecessary stress for the child (Hulland & Sigal, 2000).
Behavior therapy techniques have been used to increase compliance exhibited by children with developmental disabilities, including autism (e.g., Heinicke, Carr, & Mozzoni, 2009). One such procedure that has been demonstrated to increase compliance is the high-probability (high-p) request sequence (e.g., Mace et al., 1988; McComas et al., 1998; Zuluaga & Normand, 2008). According to Mace et al. (1988), reinforcement for compliance with the high-p requests establishes behavioral momentum for compliance that persists when the low-probability (low-p) request is presented. Thus, treatments based on the high-p request sequence involve preceding a low-p request (i.e., one associated with low levels of compliance) with a series of requests with which the participant has a history of a high probability of compliance.
The purpose of the current study was to evaluate the effectiveness of a high-p request sequence as a means of increasing compliance with medical examination requests directed to children with autism. In addition, the participants' mothers and medical professionals who had no previous training in or knowledge of behavior-analytic methods implemented the intervention.
METHOD
Participants and Settings
Two boys who had been diagnosed with autistic disorder participated in this study. Thomas was 6 years old and also had been diagnosed with developmental delays. Michel was 8 years old. Both participants had a history of noncompliance with dental and medical examination requests. Sessions were conducted either in the participants' houses or at the medical offices where the children received general medical care.
Dependent and Independent Variables, Data Collection, Procedural Integrity, and Interobserver Agreement
Compliance with a low-p request was the primary dependent variable. Compliance was defined as completing a low-p request within 10 s of its delivery. Three sets of low-p requests were implemented with each participant. Set 1 included requests related to looking in the participant's mouth. These requests were presented with modelling by the participant's mother. Set 2 included requests to look in the participant's ears. Set 3 included requests related to cutting toenails (e.g., “Give me your foot so I can cut your toenails”).
The high-p request sequence was the primary independent variable. High-p request sequences for each participant were generated using the following procedures. Prior to beginning the study, the experimenter and the participants' mothers generated a list of potential high-p requests. The participant's mother presented each potential high-p request to the participant three times a day over a 5-day period. Requests that occasioned 80% compliance or greater (about 15 for each participant) were formed into high-p request sequences. An example of a high-p request sequence generated from this list was “clap your hands,” “turn,” “do this” (simple motor imitation).
All sessions were videotaped and two observers (naive to the purposes of the study) collected data directly from videotape using a Compaq pocket PC and the Obswin software program (Kahng & Iwata, 1998). Compliance was scored if the participant complied with the low-p request within 10 s. Compliance scores were converted to a percentage by dividing the frequency of compliance by the total number of low-p requests and multiplying by 100%. Data were also collected on the delivery of the reinforcer by the various therapists, occurrence of low-p requests, occurrence of high-p requests, and compliance with high-p requests. To evaluate procedural integrity, the percentage of compliance to high-p requests that was followed by reinforcer delivery and the percentage of compliance to low-p requests that was followed by reinforcer delivery were calculated (i.e., percentage of correct trials). In the same way, the percentage of noncompliance to high-p requests that was followed by reinforcer delivery and the percentage of noncompliance to low-p requests that was followed by reinforcer delivery were calculated (i.e., percentage of error trials). Procedural integrity was assessed during 44% of sessions for Thomas and 56% of sessions for Michel. The percentage of correct trials ranged from 98% to100% (M = 98% for Thomas and M = 99% for Michel) and the percentage of error trials ranged from 0% to 2% (M = 1% for Thomas and M = 2% for Michel).
Interobserver agreement data were collected during 44% of Thomas' sessions and 56% of Michel's sessions, evenly distributed across conditions. Agreement coefficients were calculated on a point-by-point basis by dividing the total number of agreements by the number of agreements and disagreements and multiplying by 100%. Mean agreement for compliance with low-p requests was 89% for Thomas (range, 86% to 98%) and 92% (range, 88% to 100%) for Michel. Agreement was also calculated for experimenter behavior (i.e., reinforcer delivery) and was 100% for both participants.
Design and Conditions
The effects of the high-p request sequence were evaluated using an ABABCB′ design (A = low-p requests, B = high-p sequence, B′ = high-p sequence with low rate of reinforcement, C = high-p sequence with medical professional) for each participant. Sessions were conducted twice per day, 4 days per week. A session was composed of the presentation of 12 low-p requests.
Low-p requests (baseline)
The first two sessions of this condition were conducted by a medical professional who requested the participant open his mouth for a dental examination. The participant's mother conducted the three remaining sessions in the child's home, with the child seated in a chair or on the bed. Low-p requests (from Sets 1, 2, and 3 randomly) were presented once per minute during these three sessions. If the participant complied within 10 s, his mother or the medical professional provided access to preferred stimuli from a list of 10 hypothesized highly preferred items, including verbal statements (especially for the medical professional) and tactile stimuli. If the participant did not comply, his mother or the medical professional looked away without comment and the next low-p request was presented after a 45-s interval.
High-p request sequence
Procedures were identical to those in baseline, except that that the participant's mother presented a randomly selected series of three previously identified high-p requests before each low-p request. If compliance to the high-p request occurred within 5 s, she delivered praise and presented the next high-p request. If a high-p request did not result in compliance, she continued with another high-p request after a 5-s delay. All high-p requests were given within 5 s after the child complied with the previous request. After the child complied with three high-p requests, the mother delivered the low-p request (from Sets 1, 2, and 3 randomly). The next set of high-p requests was presented 15 s after the low-p request.
High-p request sequence, medical professional
The medical professional implemented the high-p request sequence in the child's home as described above. Prior to beginning the condition, the experimenter explained the procedures to the medical professional and modeled them.
High-p request sequence, low reinforcement rate
This condition was identical to the high-p request sequence condition, with the exception that the participant's mother delivered reinforcement for compliance to three consecutive high-p requests.
RESULTS AND DISCUSSION
Figure 1 displays the results for both participants. Compliance was low for both boys during baseline (Ms = 27% and 15% of low-p requests for the last three sessions for Thomas and Michel, respectively). The first implementation of the high-p request sequence was associated with an increase in compliance to means of 96% and 89% (last three sessions, Thomas and Michel, respectively). Compliance decreased with the return to baseline (Ms = 59% for Thomas and 62% for Michel) and immediately increased when the mothers reimplemented the high-p request sequence (Ms = 94% for Thomas and 98% for Michel). When the medical professional implemented the high-p request procedure, compliance with the low-p requests continued at high levels for Thomas (M = 78%) and Michel (M = 85%). Finally, high levels of compliance were maintained when the mothers implemented the high-p request sequence with the low reinforcement rate (Ms = 90% for Thomas and 92% for Michel).
Figure 1.
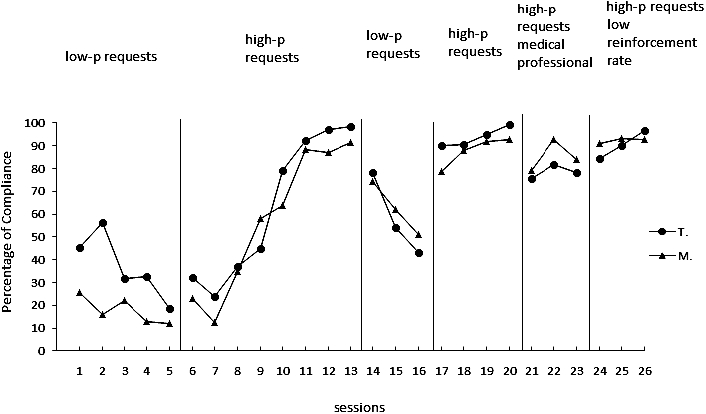
Percentage of compliance for both participants (T = Thomas and M = Michel) observed in baseline, the high-p request sequence with parents, the high-p request sequence with the medical professional, and the high-p instruction sequence with low rate of reinforcement. The two first sessions in baseline were obtained with the medical professional.
This study evaluated the effectiveness of a high-p request sequence to increase compliance of children with autism when given medical examination tasks. In addition, caregivers (parents and medical professionals) who were not trained in applied behavior analysis implemented the procedures. Results indicated that the use of the high-p response sequence increased compliance with the medical examination tasks. These findings are consistent with previous applications of high-p request sequences to increase compliance (e.g., Bullock & Normand, 2006; Davis, Brady, Williams, & Hamilton, 1992; Dawson, Piazza, Sevin, Lerman, & Keller, 2003; McComas et al., 1998, 2000; Wehby & Hollahan, 2000). The results obtained during the low reinforcement rate condition were similar to those obtained by Ardoin, Martens, and Wolfe (1999).
Results also show that the high-p request sequence can be implemented by parents and medical staff who work with children with autism. It may be easier for parents to use high-p procedures than other behavioral treatments that include potentially aversive strategies (e.g., papoose boards) or extinction because it has fewer negative side effects (e.g., increased problem behavior). Prior to the beginning of the study, the participants were given sedatives to make dental or medical examinations easier. With the high-p request sequence in place, the medical professionals were able to carry out necessary dental care and medical examinations without medication.
These results also extend the results of Zuluaga and Normand (2008). Specifically, Zuluaga and Normand demonstrated that increases in compliance with low-p requests were observed only when compliance with preceding high-p requests was followed by reinforcement. In the current study, we demonstrated that reinforcement following compliance with each high-p request was not required to maintain increases in compliance with low-p requests, as demonstrated in the low reinforcement rate condition. However, it is not clear whether initial compliance with low-p requests would have emerged had this condition been implemented at the outset of treatment. This question provides at least one avenue for future research related to the rate of reinforcement and resistance to change when using treatments that incorporate high-p request sequences.
REFERENCES
- Ardoin S.P, Martens B.K, Wolfe L.A. Using high-probability instruction sequences with fading to increase student compliance during transitions. Journal of Applied Behavior Analysis. 1999;32:339–352. [Google Scholar]
- Bullock C, Normand M. The effects of a high-probability instruction sequence and response-independent reinforcer delivery on child compliance. Journal of Applied Behavior Analysis. 2006;39:495–499. doi: 10.1901/jaba.2006.115-05. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davis C.A, Brady M.P, Williams R.E, Hamilton R. Effects of high-probability requests on the acquisition and generalization of responses to requests in young children with behavior disorders. Journal of Applied Behavior Analysis. 1992;25:905–916. doi: 10.1901/jaba.1992.25-905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dawson J.E, Piazza C.C, Sevin B.M, Lerman D, Keller M.L. Use of the high-probability instructional sequences and escape extinction in a child with food refusal. Journal of Applied Behavior Analysis. 2003;36:105–108. doi: 10.1901/jaba.2003.36-105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heinicke M.R, Carr J.E, Mozzoni M.P. Using differential reinforcement to decrease academic response latencies of an adolescent with acquired brain injury. Journal of Applied Behavior Analysis. 2009;42:861–865. doi: 10.1901/jaba.2009.42-861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hulland S, Sigal M.J. Hospital-based dental care for persons with disabilities: A study of patient selection criteria. Special Care Dentist. 2000;20((4)):131–138. doi: 10.1111/j.1754-4505.2000.tb01149.x. [DOI] [PubMed] [Google Scholar]
- Kahng S.W, Iwata B.A. Computerized systems for collecting real-time observational data. Journal of Applied Behavior Analysis. 1998;31:253–261. [Google Scholar]
- Lovaas O.I. The development of a treatment-research project for developmentally disabled and autistic children. Journal of Applied Behavior Analysis. 1993;26:617–630. doi: 10.1901/jaba.1993.26-617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mace F.C, Hock M.L, Lalli J.S, West B.J, Belfiore P, Pinter E, et al. Behavioral momentum in the treatment of noncompliance. Journal of Applied Behavior Analysis. 1988;21:123–141. doi: 10.1901/jaba.1988.21-123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mason K.P, Zurakowski D, Zgleszewski S.E, Robson C.D, Carrier M, Hickey P.R, et al. High dose dexmedetomidine as the sole sedative for pediatric MRI. Pediatric Anesthesia. 2008;18((5)):403–411. doi: 10.1111/j.1460-9592.2008.02468.x. [DOI] [PubMed] [Google Scholar]
- McComas J.J, Wacker D.P, Cooper L.J. Increasing compliance with medical procedures: Application of the high-probability request procedure to a toddler. Journal of Applied Behavior Analysis. 1998;31:287–290. doi: 10.1901/jaba.1998.31-287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McComas J.J, Wacker D.P, Cooper L.J, Peck S, Golonka Z, Millard T, et al. Effects of the high-probability request procedure: Patterns of responding to low-probability requests. Journal of Developmental and Physical Disabilities. 2000;12:157–171. [Google Scholar]
- Wehby J.H, Hollahan M.S. Effects of high-probability requests on the latency to initiate academic tasks. Journal of Applied Behavior Analysis. 2000;33:259–262. doi: 10.1901/jaba.2000.33-259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zuluaga C, Normand M. An evaluation of the high-probability instruction sequence with and without programmed reinforcement for compliance with high-probability instructions. Journal of Applied Behavior Analysis. 2008;41:453–457. doi: 10.1901/jaba.2008.41-453. [DOI] [PMC free article] [PubMed] [Google Scholar]