

Abstract
AIM: To explore the feasibility of a water-jet hybrid knife to facilitate wedge hepatic resection using a natural orifice transluminal endoscopic surgery (NOTES) approach in a non-survival porcine model.
METHODS: The Erbe Jet2 water-jet system allows a needleless, tissue-selective hydro-dissection with a pre-selected pressure. Using this system, wedge hepatic resection was performed through three natural routes (trans-anal, trans-vaginal and trans-umbilical) in three female pigs weighing 35 kg under general anesthesia. Entry into the peritoneal cavity was via a 15-mm incision using a hook knife. The targeted liver segment was marked by an APC probe, followed by wedge hepatic resection performed using a water-jet hybrid knife with the aid of a 4-mm transparent distance soft cap mounted onto the tip of the endoscope for holding up the desired plane. The exposed vascular and ductal structures were clipped with Endoclips. Hemostasis was applied to the bleeding cut edges of the liver parenchyma by electrocautery. After the procedure, the incision site was left open, and the animal was euthanized followed by necropsy.
RESULTS: Using the Erbe Jet2 water-jet system, trans-anal and trans-vaginal wedge hepatic resection was successfully performed in two pigs without laparoscopic assistance. Trans-umbilical attempt failed due to an unstable operating platform. The incision for peritoneal entry took 1 min, and about 2 h was spent on excision of the liver tissue. The intra-operative blood loss ranged from 100 to 250 mL. Microscopically, the hydro-dissections were relatively precise and gentle, preserving most vessels.
CONCLUSION: The Erbe Jet2 water-jet system can safely accomplish non-anatomic wedge hepatic resection in NOTES, which deserves further studies to shorten the dissection time.
Keywords: Natural orifice transluminal endoscopic surgery, Hepatic resection, Water-jet, Hybrid knife, Triangulation
INTRODUCTION
Liver resection, a surgical procedure consisting of hepatic parenchymal dissection as well as precise identification followed by control of intra/extra-hepatic vascular and biliary anatomy, is technically challenging due to the risk of massive bleeding during operation. Since excessive hemorrhage and subsequent blood transfusion are strongly associated with increased peri-operative morbidity and mortality, technical innovations have mainly focused on minimizing blood loss[1]. Besides inflow occlusion and low central pressure used to prevent bleeding from inflow vessels and hepatic veins in the transaction surface since the early 20th century, the development of specific devices for separating hepatic parenchyma, such as the ultrasonic dissector, water jet, Harmonic scalpel, Ligasure, and Tissue-Link dissecting sealer, has also contributed to bloodless transection. A meta-analysis[2] assessing the benefits and risks of current techniques of parenchymal transection showed that there were no significant differences in terms of the mortality, morbidity, markers of liver parenchymal injury or liver dysfunction in pairwise comparisons including cavitron ultrasound surgical aspirator, radiofrequency dissecting sealer, sharp dissection and hydro-jet. Among them, the water-jet dissector employs a pressurized jet of water to fragment the liver parenchyma tissue, with intact vascular and ductal structures, which can be ligated with staplers or clipped with titanium hemoclips, resulting in reduced blood loss, transfusion requirement, and biliary leak[3].
High-pressure water-jet dissection technology was originally developed in the steel and glass industries, where ultra-precise cutting and engraving were considered as professional demands[4]. Since introduced to medical application in 1982[5], this technology (Hydro-Jet®; ERBE, Tuebingen, Germany) has been successfully employed in open and laparoscopic operations, achieving favorable results in precise, controllable tissue-selective (indicating water-rich tissue such as liver parenchyma) dissection with excellent visualization and minimal injury to the surrounding fibrous structures (such as ductal and vessel systems with a high content of collagen and elastin)[6]. The above-mentioned Helix Hydro-Jet device with a rigid hand-held applicator is not designed with sufficient flexibility for natural orifice transluminal endoscopic surgery (NOTES) procedures, and can not be passed through a standard working channel of the current flexible endoscope because its outer-diameter is larger than the endoscopic operative channel. Now a new water-jet hybrid knife[7] incorporating with high-pressure water-jet and radiofrequency may overcome this drawback. It has a smaller size, being easy to handle, and showing more preciseness, with almost linear correlation of pressure and dissection depth, and less foaming compared with the precursor model Helix Hydro-Jet[5].
As is known, trans-luminal liver resection is technically demanding and its expansion has been lagged behind other NOTES procedures. Phee et al[8] demonstrated for the first time how a dexterous master and slave transluminal endoscopic robot could efficiently perform the wedge hepatic resection without laparoscopic assistance. Unfortunately, this technology is still an unexplored field in China. The aim of our study was to explore the safety and efficacy of a water-jet hybrid knife to facilitate wedge hepatic resection using a NOTES approach in a non-survival porcine model.
MATERIALS AND METHODS
Experimental design
This non-survival study evaluated the performance of the water-jet hybrid knife during NOTES procedure in a live porcine model. A pilot experiment in an isolated liver was conducted first, and followed by an open procedure in a 35-kg female porcine model. The formal study included three operations of wedge hepatic resection using NOTES and water-jet technology through three respective natural routes (trans-anal, trans-vaginal and trans-umbilical). The outcome measures were the time spent in performing a trans-visceral incision, the time spent in excising the liver segment, and the blood loss including oozing and brisk vascular hemorrhage, determined as blood accumulation in the suction device.
This study was conducted with prior approval by the Institutional Animal Care and Use Committee of Tongji University of China.
Experimental animal and instrument
Transluminal hepatic wedge hydro-dissection was performed in three 35-kg female pigs. The pigs were food deprived but allowed liquids for 24 h before the procedure. Urethral catheterization and warm saline enema were conducted immediately before surgery. The animals were then transferred to an operating table, and placed in supine position.
The water-jet hybrid knife (Erbe Elektromedizin) used in this study is a stainless-steel tube that incorporates a microcapillary with a diameter of 150 mm[7]. The flexible instrument has an outer diameter of 2.1 mm and a length of 2.20 mm so that it can pass through the operating channels (diameter, 2.8 and 3.7 mm) of a forward-viewing dual-channel therapeutic endoscope (GIF-2T160; Olympus Medical Systems Corporation, Tokyo, Japan). The hybrid knife can be used for hydro-dissection, rinsing blood clot and rinsing for a better endoscopic view by water-jet application, as well as coagulation by radiofrequency application. The foaming with the use of the hybrid-knife can be scavenged by the suction mechanism of the endoscope. In NOTES procedure, a 4-mm transparent distance soft cap was mounted onto the tip of the endoscope for holding up the desired surface, subsequently avoiding the deviation in the direction of the water-jet. However, it was not used in the previous open procedure, because distraction (with surgical retractors) could allow the water-jet hybrid knife to effectively dissect the tissue by exposing the base of the cutting plane.
Rau et al[6] found that a pressure of 30-40 bar was very effective to dissect normal human liver tissues, and the long-distance transmission attenuation was about 10%. Therefore, we set the pressure at 45 bar, which was proved to be effective in our pilot experiment and open operation.
Other instruments used were as follows: a flexible sterile overtube (MD48618, Sumitomo Bakelite, Tokyo, Japan), a transparent distance flat soft cap (D-201-13404, Olympus), a hook knife (KD-620LR, Olympus), endoscopic hemostatic forceps (FD-410LR, Olympus), endoclips (HX-610-135L OLYMPUS, Olympus), a foreign forcep (FQ-46L-1, Olympus), APC probe (argon plasma coagulation, APC) (ERBE Elektromedizin), and the modular VIO generator (VIO 300D; Erbe Elektromedizin, Tubingen, Germany).
Experimental procedure
Anesthesia was induced with 5% isoflurane administered intravenously. The animal was then intubated with endo-endotracheal tube, followed by general anesthesia with 1%-2% isoflurane. Throughout the operation, oxygen was administered to the animal at a flow rate according to oxygen saturation, and both pulse rate and oxygen saturation were monitored continuously using the pulse oximeter clamped to the animal tougue. Then normal saline enema was administered to each animal. Residual stool would be removed with aggressive washing, and suctioning during endoscopic inspection.
At the beginning of the procedure, entry into the peritoneal cavity was via a 15-mm linear incision made by the hook knife (a cutting width was set at 6 units and cutting interval was set at 1 unit). The ideal access point was the abdominal site 1 cm away from the umbilicus in trans-umbilical route, the bottom of the vagina in trans-vaginal route, the junction of rectum and sigmoid colon at a distance of 15-20 cm away from the anus in trans-anal route (Figure 1). Then the endoscope with a 4-mm transparent distance soft cap mounted onto the tip of the endoscope beforehand was passed through the access to reach the peritoneum using the air inflation mechanism of the endoscope.
Figure 1.

Colostomy on anterior wall of rectal junction and sigmoid colon. At the beginning of trans-annual natural orifice transluminal endoscopic surgery procedure, entry into the peritoneal cavity was via a 15-mm linear incision using the hook knife (cutting width set at 6 units and cutting interval set at 1 unit). The ideal access point was the junction of rectum and sigmoid colon at a distance of 15-20 cm away from the anus.
After the target liver segment was identified, hepatic parenchymal dissection with the water-jet hybrid knife was performed in the following steps (Figure 2), which were generally similar to those in the previous open operation except the assistance of manual retraction (Figure 3). The range to be separated was marked by an APC probe. The Glisson’s capsule was scored 2-3 mm deep along the demarcated plane of transaction with the hook knife. Then hepatic parenchyma dissection was performed using the water-jet hybrid knife kept away from the tissue in a no-touch fashion. The tip of the knife was perpendicular to but not tangentially against the predetermined surface (this was achieved with a 4-mm transparent distance soft cap mounted onto the tip of the endoscope for holding up the desired surface, subsequently avoiding the deviation in the direction of the water-jet). A smooth, reproducible, back-and-forth waving motion was used. Minor slow oozing from the cutting surface was controlled using the same knife, the hook knife or APC probe to initiate bursts of coagulation. Visible intra-hepatic vascular and ductal structures were clipped with endoscopic hemoclips. Once the liver segment was completely free and after checking for hemostasis, the incision was slightly enlarged, then an endoscopic retrieval net was inserted through the endoscopic working channel and the specimen was introduced into the net and was retrieved intactly. After the procedure, the incision site was left open, and the animal was euthanized followed by necropsy.
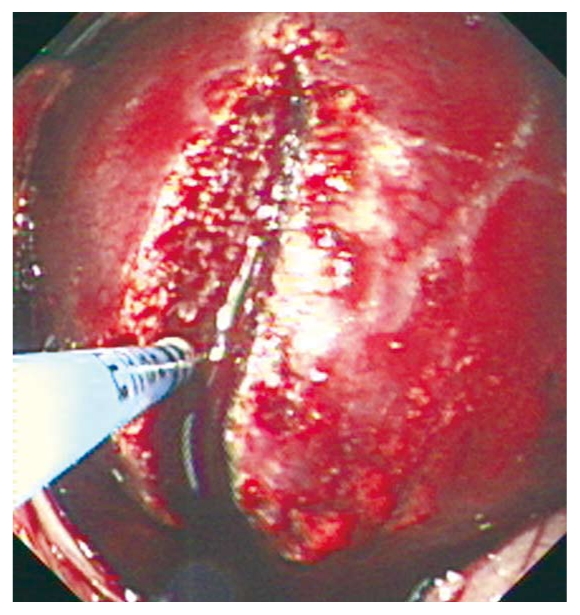
Figure 2.

Hydro-dissection of liver segment in natural orifice transluminal endoscopic surgery procedure. Hepatic parenchyma dissection was performed using the water-jet hybrid knife kept away from the tissue in a no-touch fashion and perpendicular to but not tangentially against the predetermined surface, keeping in a smooth, reproducible, back-and-forth waving motion. A 4-mm transparent distance soft cap was mounted onto the tip of the endoscope for holding up the desired surface, subsequently avoiding the deviation in the direction of the water-jet.
Figure 3.
Hydro-dissection of liver segment in open procedure. Hepatic parenchyma dissection was performed using the water-jet hybrid knife in a similar natural orifice transluminal endoscopic surgery procedure, except that the 4-mm transparent distance soft cap was not used.
Histopathological examination
Histologic examination was performed for all dissected specimens. The results were observed under microscope after hematoxylin and eosin staining based on the characteristics of the dissection margins, vessel preservation and dissection impact on the surrounding tissues. Thermal alterations such as edema and structural changes of different layers of the specimen were also microscopically analyzed.
RESULTS
It took 20 min to complete the excision of a liver segment 50 mm × 30 mm × 10 mm in size during the pilot experiment, and 45 min to complete the excision of a liver segment 45 mm × 25 mm × 10 mm in size during the open procedure. The blood loss was 100 mL in the open operation.
As for the NOTES procedure, using the Erbe Jet2 water-jet system, trans-anal and trans-vaginal wedge hepatic resections were successfully performed in two pigs without laparoscopic assistance. Trans-umbilical attempt failed due to an unstable operating platform. Each incision for peritoneal entry took 1 min, and 2 h was spent on excision of the liver tissue, indicating a hugely time-consuming part of the entire procedure. There was neither hemodynamic nor pulmonary instability throughout the NOTES procedure, and target visualization within the peritoneum was always kept clear. No untoward incident such as injury to surrounding organs occurred, and the whole intra-operative blood loss ranged from 100 to 250 mL. Parenchymal bleeding from resection could be adequately controlled by electrocautery with the hybrid knife itself, the hook knife or the APC probe (Table 1, Figure 4). Since all the exposed ductal structures were successfully clipped with Endoclips, no bile leak from the remnant liver occurred.
Table 1.
Comparisons of three routes for natural orifice transluminal endoscopic surgery procedure
| Items | Trans-umbilical route | Trans-anal route | Trans-vaginal route |
| Access position | Visually inspected at para-umbilical region | Verified by finger pressing | Located by surrounding anatomic landmarks |
| Time to complete a trans-visceral incision | About 1 min | ||
| Time to reach peritoneum | About 2 min | ||
| Liver exposure | Antero-lateral segments could be easily detected, while posterosuperior segments were hard to be explored | ||
| Working platform | Unstable | Relatively stable | |
| Time to hydro-dissection | Abandoned 1 h later | 2 h | 2 h and 40 min |
| Size of resected liver segment | No resected specimen was obtained due to failure in trans-umbilical hepatic resection | 50 mm × 25 mm × 5 mm | 45 mm × 30 mm × 7 mm |
| Bile leak | Not found | ||
| Blood loss | 100 mL | 200 mL | 250 mL |
| Injury to surrounding organs | Not occurred | ||
Figure 4.

A resected liver segment compared with the reserved part. A resected liver segment was picked out with white gauze.
There were relatively smooth and precise cutting margins in all histological preparations. The cutting width at the bottom of the cut was similar to the dissection width at tissue surface, with little vessel damage (Figure 5). Some thermal alterations were obtained due to intra-operative electrocautery (Figure 6).
Figure 5.

Microscopic findings of water-jet dissection in liver tissues (HE stain, × 40). A smooth and gentle cutting margin was presented. The cutting width at the bottom of the cut was similar to the dissection width at tissue surface, with little vessel damage.
Figure 6.

Thermal alterations due to intra-operative coagulation (HE stain, × 100). Removal of the liver capsule could be seen in an example of thermal damage.
DISCUSSION
To the best of our knowledge, this is the first study in a non-survival porcine model evaluating the feasibility and safety of wedge hepatic resection merely using a NOTES approach, Erbe Jet2 water-jet technology and endoscopic instrument.
Since first described by Kalloo et al[9], natural orifice transluminal endoscopic surgery (NOTES) has become the newest minimally invasive surgical procedure in contrast to open and laparoscopic technology. It involves passing flexible endoscopic systems through natural orifices (per-oral, trans-vaginal, trans-anal, trans-umbilical or trans-vesical routes), approaching target organs and performing intra-abdominal procedures. For the entry into the peritoneal cavity, a trans-luminal incision is mostly created by endoscopic needle knife followed by balloon dilation. However, in our study, it was achieved just in about 1 min via a hook knife, with the same desirable effect. The air-inflation mechanism of the endoscope was used to induce and maintain peritoneum, and the suction mechanism of the endoscope was used intermittently to avoid a high intra-abdominal pressure. Overall, there was neither hemodynamic nor pulmonary instability during NOTES, as described elsewhere[10].
Similar to laparoscopic liver resection, NOTES hepatic procedures must confront one and the same Achilles’ heel, difficulty in obtaining hemostasis. Given the facts that protection of blood vessels is essential to minimize hemorrhage and blood transfusion, and smooth dissection margins might minimize adhesion formation[11], the water-jet hybrid knife was taken into consideration. Hydro-dissection was accomplished with the hybrid knife kept away from the tissue in a no-touch fashion and perpendicular to but not tangentially against the predetermined surface. Minor slow oozing from the cutting surface was controlled using the same knife, the hook knife or APC probe to initiate bursts of coagulation. Visible intra-hepatic vascular and ductal structures were clipped with endoscopic hemoclip. Certainly, the need for coagulation or clipping of individual vessels led to a prolonged operative time.
Current flexible endoscopes have significant limitations when used for complex therapeutic procedures. Stable platform and off-axis operation are often necessary for the NOTES. However, standard endoscopic shafts are too flexible and prone to looping, if these unfavorable factors caused the failure in transumbilical endoscopic hepatic resection. As for triangulation of endoscopically deployed instruments to approach the same target, internal double channels are small and in close proximity, producing parallelism and limiting possible triangulating interactions[12]. The operator interface parallelism does not allow satisfactory traction/countertraction for effective dissection of tissue and organs. To counteract the negative impact on dissection efficiency, a 4-mm transparent distance soft cap was mounted onto the tip of the endoscope for holding up the desired plane, subsequently avoiding the deviation in the direction of the water-jet. Unfortunately, its effect was limited due to the heavy weight of the porcine liver and the restricted field of view. As a result, excision of one piece of the same size from the porcine liver was more difficult in NOTES than in open procedure (more than 2 h was spent in NOTES, but only 45 min spent in open procedure).
Notably, non-anatomic wedge hepatic resection by a NOTES approach in either our or Phee’s[8] study is still at a primary stage. As NOTES using current endoscopic instruments is technically difficult to realize pedicle control with an intrahepatic Glissonian approach[13], it is suitable only for superficial lesions of the liver mostly with the fine trabecular infrastructures and medium caliber structures. In order to achieve the same level of segment-based laparoscopic liver resection[14], advance in NOTES technology still has a long way to go.
In conclusion, the water-jet hybrid knife with the capacity of selective vessel-sparing tissue dissection can safely accomplish non-anatomic wedge hepatic resection through a NOTES approach. At the same time, its efficiency may be discounted by endoscopic deficiencies: lack of surgical triangulation, unstable operating platform as well as transmission attenuation caused by long distance and endoscopic looping. Although this technology is only at its beginning stage, as the old saying goes: well begun is half done.
COMMENTS
Background
Liver resection is technically challenging due to the risk of massive bleeding during operation. Since the early 20th century, the development of specific devices for separating hepatic parenchyma has contributed to bloodless transection. Furthermore, trans-luminal liver resection is technically demanding and its expansion has been lagged behind other natural orifice transluminal endoscopic surgery (NOTES) procedures.
Research frontiers
Phee described for the first time how a dexterous master and slave transluminal endoscopic robot could efficiently perform the wedge hepatic resection without laparoscopic assistance. This technology is still an unexplored field in China.
Innovations and breakthroughs
This is the first study to evaluate the feasibility and safety of non-anatomic wedge hepatic resection in a non-survival porcine model using a NOTES approach, Erbe Jet2 water-jet technology and endoscopic instruments. The study demonstrated that the water-jet hybrid knife with the capacity of selective vessel-sparing tissue dissection can safely accomplish non-anatomic wedge hepatic resection through a NOTES approach.
Applications
Currently, non-anatomic wedge hepatic resection using NOTES approach and water-jet technology is suitable only for superficial lesions of the liver mostly with the fine trabecular infrastructures and medium caliber structures.
Terminology
High-pressure water-jet dissection technology was originally developed in the steel and glass industries, where ultra-precise cutting and engraving were considered as professional demands[4]. Since introduced to medical application in 1982[5], this technology has been successfully employed in open and laparoscopic operations, achieving favorable results in precise, controllable tissue-selective dissection with excellent visualization and minimal injury to the surrounding fibrous structures (such as ductal and vessel systems with a high content of collagen and elastin).
Peer review
This is the study in a non-survival porcine model evaluating the feasibility and safety of wedge hepatic resection by using pure NOTES approach.
Acknowledgments
We thank Dr. Jiang-Fan Zhu for his editorial assistance.
Footnotes
Peer reviewer: Chih-Chi Wang, MD, Department of Surgery, Chang Gung Memorial Hospital-Kaohsiung Medical Center, 123 Ta-Pei Road, Niao-Sung, Kaohsiung 833, Taiwan, China
S- Editor Tian L L- Editor Ma JY E- Editor Ma WH
References
- 1.Lesurtel M, Belghiti J. Open hepatic parenchymal transection using ultrasonic dissection and bipolar coagulation. HPB (Oxford) 2008;10:265–270. doi: 10.1080/13651820802167961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gurusamy KS, Pamecha V, Sharma D, Davidson BR. Techniques for liver parenchymal transection in liver resection. Cochrane Database Syst Rev. 2009:CD006880. doi: 10.1002/14651858.CD006880.pub2. [DOI] [PubMed] [Google Scholar]
- 3.Rau HG, Wichmann MW, Schinkel S, Buttler E, Pickelmann S, Schauer R, Schildberg FW. [Surgical techniques in hepatic resections: Ultrasonic aspirator versus Jet-Cutter. A prospective randomized clinical trial] Zentralbl Chir. 2001;126:586–590. doi: 10.1055/s-2001-16573. [DOI] [PubMed] [Google Scholar]
- 4.Vollmer CM, Dixon E, Sahajpal A, Cattral MS, Grant DR, Gallinger S, Taylor BR, Greig PD. Water-jet dissection for parenchymal division during hepatectomy. HPB (Oxford) 2006;8:377–385. doi: 10.1080/13651820600839449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tschan CA, Tschan K, Krauss JK, Oertel J. First experimental results with a new waterjet dissector: Erbejet 2. Acta Neurochir (Wien) 2009;151:1473–1482. doi: 10.1007/s00701-009-0333-2. [DOI] [PubMed] [Google Scholar]
- 6.Rau HG, Duessel AP, Wurzbacher S. The use of water-jet dissection in open and laparoscopic liver resection. HPB (Oxford) 2008;10:275–280. doi: 10.1080/13651820802167706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Neuhaus H, Wirths K, Schenk M, Enderle MD, Schumacher B. Randomized controlled study of EMR versus endoscopic submucosal dissection with a water-jet hybrid-knife of esophageal lesions in a porcine model. Gastrointest Endosc. 2009;70:112–120. doi: 10.1016/j.gie.2008.10.042. [DOI] [PubMed] [Google Scholar]
- 8.Phee SJ, Ho KY, Lomanto D, Low SC, Huynh VA, Kencana AP, Yang K, Sun ZL, Chung SC. Natural orifice transgastric endoscopic wedge hepatic resection in an experimental model using an intuitively controlled master and slave transluminal endoscopic robot (MASTER) Surg Endosc. 2010;24:2293–2298. doi: 10.1007/s00464-010-0955-8. [DOI] [PubMed] [Google Scholar]
- 9.Kalloo AN, Singh VK, Jagannath SB, Niiyama H, Hill SL, Vaughn CA, Magee CA, Kantsevoy SV. Flexible transgastric peritoneoscopy: a novel approach to diagnostic and therapeutic interventions in the peritoneal cavity. Gastrointest Endosc. 2004;60:114–117. doi: 10.1016/s0016-5107(04)01309-4. [DOI] [PubMed] [Google Scholar]
- 10.von Delius S, Sager J, Feussner H, Wilhelm D, Thies P, Huber W, Schuster T, Schneider A, Schmid RM, Meining A. Carbon dioxide versus room air for natural orifice transluminal endoscopic surgery (NOTES) and comparison with standard laparoscopic pneumoperitoneum. Gastrointest Endosc. 2010;72:161–169, 169.e1-2. doi: 10.1016/j.gie.2010.01.013. [DOI] [PubMed] [Google Scholar]
- 11.Dubcenco E, Grantcharov T, Streutker C. A pilot study in a survival Porcine model evaluating the feasibility and safety of adhesiolysis by using transgastric NOTES® approach, waterjet technology and endoscopic instruments. Gastrointest Endosc. 2010;71:AB198. [Google Scholar]
- 12.Thompson CC, Ryou M, Soper NJ, Hungess ES, Rothstein RI, Swanstrom LL. Evaluation of a manually driven, multitasking platform for complex endoluminal and natural orifice transluminal endoscopic surgery applications (with video) Gastrointest Endosc. 2009;70:121–125. doi: 10.1016/j.gie.2008.11.007. [DOI] [PubMed] [Google Scholar]
- 13.Machado MA, Makdissi FF, Galvão FH, Machado MC. Intrahepatic Glissonian approach for laparoscopic right segmental liver resections. Am J Surg. 2008;196:e38–e42. doi: 10.1016/j.amjsurg.2007.10.027. [DOI] [PubMed] [Google Scholar]
- 14.Yoon YS, Han HS, Cho JY, Ahn KS. Total laparoscopic liver resection for hepatocellular carcinoma located in all segments of the liver. Surg Endosc. 2010;24:1630–1637. doi: 10.1007/s00464-009-0823-6. [DOI] [PubMed] [Google Scholar]