

Abstract
Background:
Acne vulgaris is a chronic inflammatory disease of the pilosebaceous units, which chiefly involves face and upper part of the trunk. Its prevalence is highest in adolescence, where the individual counters several psychosocial changes. Depression, suicidal thoughts, and low self esteem are reported in the patients with this disease.
Aim:
The goal of this study is to compare prevalence of anxiety and depression in the patients with acne vulgaris and normal population.
Materials and Methods:
In this cross-sectional study, 82 patients with acne vulgaris and 82 persons without acne who referred to a dermatology clinic and a specialized office for skin diseases in Rasht were studied. Anxiety and depression were evaluated by Hospital Anxiety and Depression Scale (HADS) questionnaire and severity of acne was evaluated by Global Acne Grading System (GAGS). Data were analyzed by SPSS ver. 14.0 software, independent T-test, multi variate analysis of covariance (MANCOVA) and chi-square test for comparison the quantitative and ordinal data, respectively; with α=0.05.
Results:
Prevalence of anxiety and mean of anxiety scores were 68.3% and 9.17 ± 3.52, respectively, in patients group and 39.1% and 7.10 ± 3.07, respectively, in control group in which there was a significant difference (P = 0.001). Prevalence of depression and mean of depression scores were 25.6% and 5.34 ± 3.29, respectively, in patients group and 28.1% and 5.01 ± 3.32, respectively, in control group in which there was no significant difference.
Conclusion:
According to high prevalence of anxiety in patients with acne vulgaris, assessment of the screening mental status of the patients by simple questionnaire such as HADS is suggested.
Keywords: Anxiety, Depression, GAGS, HADS questionnaire
Introduction
Acne vulgaris is the chronic inflammatory disease of the pilosebaceous units, which chiefly involves face and upper part of the trunk and is characterized by seborrhea, comedo, red papules, superficial pustules, deep or pseudocystic nodules, pustules, and sometimes scar.
Four main factors play roles in its pathogenesis: increase of sebum production, hyper cornification of the pilosebaceous duct, microbial flora, especially colonization of Propionibacterium Acne, and inflammation[1]
Knowledge of relationship between skin diseases and mental health is increasing. There are some reports of existence of mental disorders such as anxiety, depression, aggression, low self esteem, suicidal thoughts and attempts in patients with acne vulgaris.[1,2]
In some studies, increase of prevalence of anxiety in patients with acne and positive relationship between severity of anxiety and severity of acne are reported.[3–5,7] However, in some other studies, no relationship between acne and anxiety is seen or the severity of anxiety and depression was not related to the severity of acne clinically.[6,7,8] Some studies reported that anxiety and depression are not correlated with age and sex,[4,6] but some studies reported that these disorders are more prevalent in women.[9,10] In one study, among 16 cases of reported suicide in skin disease, seven cases were due to acne.[7] In Kellet et al. study on 34 patients with acne, using hospital anxiety and depression scale (HADS) questionnaire, depression and anxiety score in these patients were more than in patients with psoriasis and cancer and mental disorders were more in women. Considerable clinical depression and anxiety were present in 18 and 44% of the patients, respectively.[9]
Yazici et al. performed a study on 61 patients with acne, using hospital anxiety and depression score (HADS), dermatology life quality index (DLQI), acne quality of life (AQOL), global acne grading system (GAGS), and it was found that amount of anxiety and depression in patients group were respectively 0 and 7.9% (P=0.001, P=0.011 respectively.[6] Because some confirmed psychological disorders in patients with acne, we decided to evaluate the prevalence of anxiety depression in comparison to healthy people.
Materials and Methods
In this cross-sectional study, 82 patients with acne vulgaris and 82 healthy companions (with no acne) at the age of 14–30, who referred to Razi hospital skin clinic and a specific office for skin disease in Rasht, were enrolled into the study. Patients were matched for age and sex by patient group. In case group, Inclusion criterion was the diagnosis of acne including presence of white head comedo and black head comedo, papule, pustule, pseudocyst and scar, and all individuals between 14 and 30 years old individuals accepted and signed our agreement based on Helsinki contract. Exclusion criteria were: (1) patients or healthy individuals with history of a known mental disorder; (2) patients with somatic diseases such as heart, pulmonary and joint diseases, diabetes and epilepsy that affect their mental status; (3) patients who used topical or systemic medicines disposing acne during one month before refer for acne; these medicines included anabolic steroids, corticosteroids (topical, oral, injection), corticotropin, phenytoin, phenobarbital, lithium, isoniazid, iodides, bromides, cyclosporin, and azathiopreine.
HADS questionnaire was completed by both groups and their anxiety score(HAD-A) and depression score (HAD-D) were calculated. Severity of acne was identified in patients and data were analyzed by SPSS ver 14.0 software. Mean of anxiety and depression scores in two groups of being less and more than 20 years old, men and women, married and single patients and healthy individuals were compared between two groups by t-test and different levels of anxiety and depression frequency were compared by Chi-square test.
To adjust the confounding effect of age, sex, marital status, severity of acne, and scar of it on anxiety and depression scores, we used multivariate evaluated using analysis of covariance t -test.
HADS questionnaire includes 14 questions (seven questions related to anxiety and seven questions related to depression) [Figure 1] and each question scores 0 to 3 depending on the severity of the problem. Summing anxiety score, HAD-A(Anxiety subscale), and summing depression scores, HAD-D (depression subscale) were achieved.
Figure 1.
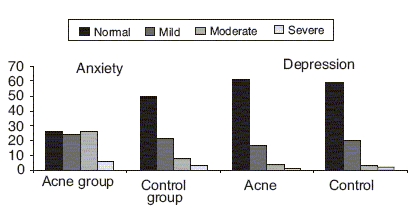
Frequency distribution of anxiety and depression Level in two groups of study
HADS interpretation: 0-7 scores: normal; 8-10 scores: mild; 11-14 score: moderate; 15-21 scores: severe. Internal consistency according to α-Chronbach for Persian copy of HADS questionnaire based on Montazeri et al. study for HAD-D and HAD-A is 0.86 and 0.78, respectively.[11]
GAGS is a simple, accurate, fast method for the determination of severity of acne, and it requires no special equipment and is relatively cost-effective. Its personal and interpersonal differences is low and it was first used by Doshi and his colleagues in 1997 in USA.[12]
Results
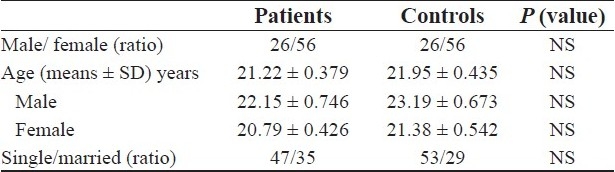
Patients group included 82 patients (26 men and 56 women) with the age range of 20.46-21.97 years and mean age of 21.22 years and control group included 82 patients with the age range of 21.08 - 22.82 years and mean age of 21.95 years. There was no significant difference between two groups in sex, age, and marital status. Among 82 patients with acne, 38 cases were with mild acne (46.3%), 37 cases were with moderate acne (45.2%), and seven cases were with severe acne (8.5%) [Table 1].
Table 1.
Demographic characteristics of two groups characteristics
Anxiety was seen in 68.3% of the patients and depression was seen in 25.6% of the patients. There was a significant difference in anxiety prevalence between patients group and control groups (P <0.001). Mean scores of anxiety and depression were 9.26 ± 0.382 and 7.10 ± 0.339, respectively, and mean score of anxiety was more in patients group than control group (P = 0.001) [Table 2 part 1].
Table 2.
Frequency distribution of anxiety and depression scores in two group by demographic variables
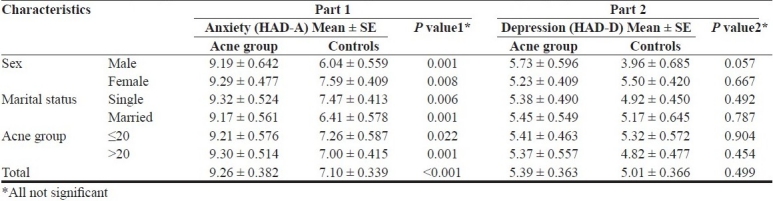
Prevalence and mean scores of anxiety and depression had no relationship with severity of acne and sex, age, marital status, and scar of acne (using analysis of covariance test) [Table 1].
In patients group, there was no significant difference in incidence of anxiety and depression and mean of their scores between women and men, married people and single ones, and two groups of being ≤ 20 years old and > 20 years old. Severity of anxiety and depression was not related to the severity of acne and its scar [Table 2 part 2].
Discussion and Conclusion
In different studies, presence of some mental disorders in patients with acne was reported, including low self esteem, avoidance, hastiness and anxiety, depression, shame, suicidal thoughts and attempts, and difficulties in applying for a job.[1,7]
Prevalence of anxiety and depression in patients with acne is different in some studies. In our patients, prevalence of anxiety was 68.3% in acne patients which show a significant difference with control group (P<0.001). Considerable clinical anxiety (moderate to severe HAD-A≥10) was 39% in patients group and 13.5% in control group with a significant difference (P = 0.001). This result was similar to those of Yazici et al. study.[6,8,10] in Turkey in which HADS was used to determine anxiety and depression.[2–4] In our study, depression was seen in 25.6% of the patients with no significant difference with control group.
There was no relationship between severity of acne and severity of anxiety and depression. This result was similar to those of Aktan, Niemerir, and Yazici study[6,8,10] and is contrast to the results of some studies in which there was a positive relationship between severity of acne and severity of anxiety and depression.[3,4,5]
Also, the severity of anxiety and depression was not related to age, sex, marital status, and scar of acne. These results were contrast to the results of some studies in which prevalence of anxiety and depression was more in women than men.[6,10]
Psychosocial problems such as low self esteem, anxiety and depression, and decrease in social relationships in patients with acne are considered to be due to disorder of self body image. In self-body image, some parts of the body including face play an important role. Existence of even a minor lesion in this part may be unpleasant for the patient and seems large.[3,6] This image can cause mental disorders including depression and anxiety, low self esteem, and decrease in social relationships.
Improvement in mental disorders following treatment of acne, specially oral isotretinoin, has been reported in patients with acne along with the improvement of self body image.[1,5,6,7]
According to existence of some mental disorders in patients with acne, independent of age, sex, marital status, severity of acne and its scar, evaluation and screening of these disorders in all patients with acne who referred for treatment are suggested. This can be done by simple questionnaires such as HADS with high sensitivity and specificity, which is not very time consuming.
These questionnaires can be used as a tool to evaluate the effect of treatment besides clinical signs. Studies in the field of evaluation of the effect of different treatments of acne using these questionnaires are suggested.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil.
References
- 1.Simpson NB, Cunliffe WJ. Disorders of the sebaceous glands. In: Burms T, editor. Rook's text book of dermatology. 7th ed. Vol. 3. Turin, Italy: Blackwell Science; 2004. pp. 43–15. [Google Scholar]
- 2.Schulpis K, Georgala S, Papakonstantinou ED, Michas T. Psychological and sympatho- adrenal status in patients with cystic acne. J Eur Acad Dermatol Venereol. 1999;13:24–7. [PubMed] [Google Scholar]
- 3.Wu SF, Kinder BN, Trunnell TN, Fulton JE. Role of anxiety and anger in acne patients: A relationship with the severity of the disorder. J Am Acad Dermatol. 1988;18:325–32. doi: 10.1016/s0190-9622(88)70047-x. [DOI] [PubMed] [Google Scholar]
- 4.Pearl A, Arroll B, Lello J, Birchall NM. The impact of acne: A study of adolescent's Attitudes, Perception and Knowledge. N Z Med J. 1998;111:269–71. [PubMed] [Google Scholar]
- 5.Grahame V, Dick DC, Morton CM, Watkins O, Power KG. The psychological correlates of treatment efficacy in acne. Dermatol Psychosom. 2002;3:119–25. [Google Scholar]
- 6.Yazici K, Baz K, Yazici AE, Köktürk A, Tot S, Demirseren D, et al. Disease -specific Quality of life is associated with anxiety and depression in patients with acne. J Eur Acad Dermatol Venereol. 2004;18:435–9. doi: 10.1111/j.1468-3083.2004.00946.x. [DOI] [PubMed] [Google Scholar]
- 7.Cotterill JA, Cunliffe WJ. Suicide in dermatological patients and psoriasis. Br J Dermatol. 1997;137:246–50. doi: 10.1046/j.1365-2133.1997.18131897.x. [DOI] [PubMed] [Google Scholar]
- 8.Niemeier V, Kupfer J, Demmelbauer-Ebner M, Stangier U, Effendy I, Gieler U. Coping with acne vulgaris: Evaluation of the chronic skin disorder questionnaire in patients with acne. Dermatology. 1998;196:108–15. doi: 10.1159/000017842. [DOI] [PubMed] [Google Scholar]
- 9.Kellett SC, Gawkrodger DJ. The psychological and emotional impact of acne and the effect of treatment with isotretinoin. Br J Dermatol. 1999;140:273–82. doi: 10.1046/j.1365-2133.1999.02662.x. [DOI] [PubMed] [Google Scholar]
- 10.Aktan S, Ozmen E, Sanli B. Anxiety, depression and nature of acne vulgaris in adolescents. Int J Dermatol. 2000;39:354–7. doi: 10.1046/j.1365-4362.2000.00907.x. [DOI] [PubMed] [Google Scholar]
- 11.Montazeri A, Vahdaninia M, Ebrahimi M, Jarvandi S. The hospital Anxiety and Depression Scale (HADS): Translation and validation study of the Iranian version. Health Qual Life Outcomes. 2003;1:14. doi: 10.1186/1477-7525-1-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Doshi A, Zaheer A, Stiller MJ. A comparison of current acne grading system: And proposal of novel system. Int Dermatol. 1997;36:416–8. doi: 10.1046/j.1365-4362.1997.00099.x. [DOI] [PubMed] [Google Scholar]