

Abstract
High tibial osteotomy (HTO) is a surgical procedure used to change the mechanical weight-bearing axis and alter the loads carried through the knee. Conventional indications for HTO are medial compartment osteoarthritis and varus malalignment of the knee causing pain and dysfunction. Traditionally, knee instability associated with varus thrust has been considered a contraindication. However, today the indications include patients with chronic ligament deficiencies and malalignment, because an HTO procedure can change not only the coronal but also the sagittal plane of the knee. The sagittal plane has generally been ignored in HTO literature, but its modification has a significant impact on biomechanics and joint stability. Indeed, decreased posterior tibial slope causes posterior tibia translation and helps the anterior cruciate ligament (ACL)-deficient knee. Vice versa, increased tibial slope causes anterior tibia translation and helps the posterior cruciate ligament (PCL)-deficient knee. A review of literature shows that soft tissue procedures alone are often unsatisfactory for chronic posterior instability if alignment is not corrected. Since limb alignment is the most important factor to consider in lower limb reconstructive surgery, diagnosis and treatment of limb malalignment should not be ignored in management of chronic ligamentous instabilities. This paper reviews the effects of chronic posterior instability and tibial slope alteration on knee and soft tissues, in addition to planning and surgical technique for chronic posterior and posterolateral instability with HTO.
Keywords: Knee, High tibial osteotomy, Tibial slope, Posterior instability, Varus deformity
Introduction
High tibial osteotomy (HTO) has always been performed to correct malalignment of the knee due to osteoarthritis (OA) of the medial compartment associated with pain and functional impairment. Some studies [1, 2] have demonstrated that alignment correction was associated with regeneration of articular cartilage apparently normal, so in the last 10 years HTO has become very popular in association with new cartilage techniques and meniscal graft [3]. In the past years, knee malalignment associated with chronic instability and varus thrust has been considered a contraindication for HTO because of the poor results reported in literature [4, 5]. However, nowadays, chronic instability has become again an indication for HTO, because it allows the surgeon to correct both the coronal and the sagittal alignment, improving the function of an unstable knee. In literature, the sagittal plane of the knee has often been ignored; however, its modification has effects on biomechanics and articular stability. Camarda et al. [6] showed good results in treatment of chronic isolated PLC injury with fibular-based technique; however, when PLC injury is associated with malalignment, soft tissue techniques alone, without correction of the alignment, often give poor results because bone deformity overstresses them [7–10]. Furthermore, soft tissue destruction causes a decrease in neuromuscular joint control, which in time can worsen the malalignment [11]. Other studies [7, 12–15] have underlined that reconstruction of the posterior cruciate ligament (PCL), without repair or reconstruction of the posterolateral corner (PLC), often gives poor results. Some authors [4, 5, 9, 16–18] have reported satisfactory results after HTO in unicompartmental knee OA and varus alignment, whereas there are few studies reporting results of HTO in the unstable knee [10, 18, 19]. For treatment of a PCL/PLC-deficient knee associated with varus malalignment to improve function and stability of the knee, recent studies about the biomechanics of the knee after HTO suggest that this procedure should be performed before soft tissue reconstruction, because soft tissue procedures alone often give poor results [10, 18, 19]. HTO is also useful in treatment of an anterior cruciate ligament (ACL) lesion associated with a varus of the knee [20–28]. The aim of this review is to report on HTO for treatment of a PCL/PLC-deficient knee associated with varus malalignment, in particular to discuss the importance of the tibial slope, because its modifications can improve knee stability and reduce forces on PCL, PLC, and articular cartilage.
Anatomy
This paper reports only the most important information about the anatomy of the tibia, PCL, and PLC. For a complete description of these structures, the reader is advised to consult specific literature.
The tibia is a large bone transmitting, from the knee to the ankle, most of the stress of walking. It has a large subcutaneous surface that allows access to the bone along its entire length. It is surrounded by three compartments of muscle: the anterolateral, the lateral, and the posterior. The medial surface of the tibia is not covered by muscles, providing easier access to the bone [29]. The proximal anteromedial tibial cortex, viewed in cross-section, has an oblique or triangular shape, and it forms an angle of 45 ± 6° with the posterior margin of the tibia, whereas the lateral tibial cortex is nearly perpendicular to the posterior margin of the tibia [13].
The PCL originates from the lateral aspect of the medial condyle, and it inserts on the posterior edge of the tibial plateau. It has two boundle, the anterolateral and the posteromedial [30–32].
Seebacher et al. [33] described three layers in the PLC. The external layer is formed by the biceps femoris and the ileotibial tract. The middle layer is formed by the quadriceps retinaculum and the patellofemoral ligaments. The internal layer consists of a superficial lamina, formed by the lateral collateral ligament (LCL) and the fabellofibular ligament, and a deep lamina, formed by the popliteofibular ligament, the arcuate ligament, and the popliteus muscle with its tendon. The two laminae of the internal layer are the most important stabilizing structures of the PLC.
Biomechanics
There are three geometric variables to consider in the correction of a deformity [34]:
Center of rotation of angulation (CORA)
Angulation correction axis (ACA)
Osteotomy level
CORA is the intersection between the proximal mechanical axis (PMA) and the distal mechanical axis (DMA). It is not under surgeon control, because it is related to the morphology of the deformity.
ACA is the axis around which the deformity is carried. It is partially under the control of the surgeon.
The level of osteotomy is totally under surgeon control.
Paley [34] defined three rules for osteotomies:
If the level of osteotomy and ACA pass for CORA, realignment takes place without translation.
If ACA pass for CORA but the osteotomy is at a different level, realignment takes place with angulation and translation at the osteotomy site.
If osteotomy and ACA are above or below CORA, realignment takes place with translation.
ACA and CORA have to be as close as possible to avoid secondary deformity with translation after osteotomy is performed. Fortunately, in HTO, ACA and CORA are very close to each other, therefore only the angular deformity will be corrected after surgery.
Patients with varus of the knee and posterolateral instability often present so-called hyperextension varus thrust gait, i.e., during the gait cycle the knee with posterolateral instability tends to go into varus and hyperextend with an increase in adduction and a decrease in abduction moments. The result is that the medial compartment narrows and the lateral compartment enlarges due to deficiency of posterolateral soft tissue structures, which in chronic lesions become overused with a further decrease in function. This phenomenon is increased during gait because all the weight is applied through one limb [20, 35, 36].
Effects of a chronic PCL/PLC lesion
Some authors [20, 35] have quantified the range of knee hyperextension with the hyperextension varus thrust: during all the different phases of the gait cycle, the knee with a PCL lesion hyperextends compared with a normal knee. The amount of knee flexion reported by these authors [20, 35] is:
Heel strike with PCL: 1.3 ± 1.6° of knee flexion
Heel strike without PCL: −5.6 ± 2.8° of relative knee flexion (hyperextension)
Midstance with PCL: 14.9 ± 5° of knee flexion
Midstance without PCL: 6.2 ± 10.9° of knee flexion
Off toe with PCL: 6.6 ± 4° of knee flexion
Off toe without PCL: −7.3 ± 4.4° of relative knee flexion (hyperextension)
An isolated chronic PCL lesion causes the tibia to translate posteriorly and to rotate externally about the femur. The amount of tibial posterior translation depends on the grade of PCL lesion: grade I (1–5 mm), grade II (5–10 mm), grade III (>10 mm) [37–39].
A chronic PCL lesion can have effects on osteocartilaginous structures and on soft tissues of the knee. The osteocartilaginous effect is an osteoarthritic degeneration of the medial compartment of the knee due to the aforementioned biomechanical changes and a quantitative reduction of PCL mechanoceptors [40]. After a PCL lesion, the pressure increases by about 30% in the medial compartment of the knee (from 338 N with intact PCL to 445 N in a PCL-deficient knee) [11, 12]. Osteoarthritic changes take place even in the patellofemoral joint, due to an increase in pressure of about 16% (from 398 N with PCL to 440 N without PCL) [41, 42]. Patellofemoral joint pressure increases mainly on the lateral facet because of an internal femoral rotation (depending on external tibial rotation), and on the inferior pole because the posterior tibial translation increases the tension along the patellar tendon; this increases patellar flexion (it becomes more horizontal) by about 4.4° at 14° of knee flexion [38, 39]. Soft tissue effects occur mainly on ACL, which presents a decrease in number, diameter, and density of collagen fibers [43], and on PLC; indeed, forces on PLC increase from 34 ± 25 N with PCL to 63 ± 24 N without PCL at 30° of knee flexion and from 38 ± 46 N with PCL to 86 ± 53 N without PCL at 90° of knee flexion [37]. In literature, meniscal lesions are associated with an acute PCL lesion in 16–28% of cases [44–46] and with a chronic PCL lesion in 36% of cases [45].
The effects of a PCL lesion are more evident when a PLC lesion is also present. This event is not rare, as in 60% of cases PCL and PLC lesions are associated [47]. The final result is chronic posterolateral instability, defined as triple varus by Noyes and Simon [48] (Fig. 1). The first varus is osseous, the second varus is lateral compartment enlargement due to LCL deficiency, and the third varus is associated with hyperextension and is due to PLC deficiency.
Fig. 1.

Posterolateral chronic instability
Observations about posterior tibial slope
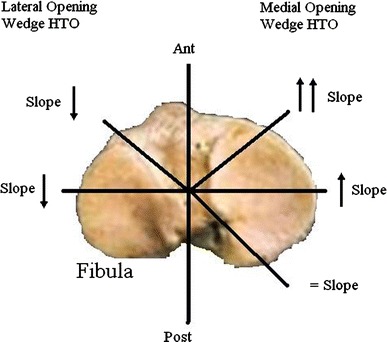
In the normal knee the medial posterior tibial slope is usually 9–11° and the lateral posterior tibial slope is generally 6–11°; however, in literature a wide range of values are reported [21, 49–55] because there are five radiographic techniques described for its evaluation (see the “Imaging” section for further explanation). The sagittal plane of the knee has often been ignored; however, its changes cause important modifications in the biomechanics of the knee and in joint stability. Indeed, with HTO it is possible to modify not only the coronal plane but also the sagittal plane of the knee, causing anterior or posterior translation of the tibia about the femur. This has resulted in a great increase in osteotomy in the last 10 years for treatment of chronic knee instability. The proximal anteromedial tibial cortex, viewed in cross-section, has an oblique or triangular shape and forms an angle of 45 ± 6° with the posterior margin of the tibia, whereas the lateral tibial cortex is nearly perpendicular to the posterior margin of the tibia. Because of these anatomical features, medial opening wedge HTO increases the tibial slope only if the anteromedial gap is equal to the posteromedial gap, whereas the slope does not change if the anteromedial gap is smaller than the posteromedial gap [13]. Because of these same anatomical features, lateral closing wedge osteotomy causes small decreases in posterior tibial slope. Some authors [22, 56–59] have demonstrated that lateral closing wedge HTO causes a decrease in posterior tibial slope, and posterior translation of the tibia, and stabilizes a knee with anterior instability (Fig. 2), whereas medial opening wedge HTO increases the posterior tibial slope, causes anterior translation of the tibia, and stabilizes a knee with posterior instability [21, 60] (Fig. 3). Moreover, medial opening wedge HTO preserves the proximal tibiofibular joint, does not change the length of the posterolateral structures, and prevents proximal migration of the fibula that could increase posterolateral instability.
Fig. 2.

Closing wedge HTO causes a decrease in posterior tibial slope, and posterior translation of the tibia; it stabilizes a knee with anterior instability
Fig. 3.

Opening wedge HTO causes an increase in posterior tibial slope, and anterior translation of the tibia; it stabilizes a knee with posterior instability
As described by Rodner et al. [61], the amount of posterior tibial slope after HTO depends on the position of the plate used to stabilize the osteotomy; for example, an anteromedial plate increases the slope on average by 5.5° and a posteromedial plate tends not to modify the posterior tibial slope (Fig. 4). Noyes et al. [13] calculated the effect of the opening wedge angle of medial HTO on the posterior tibial slope and stated that, if the anteromedial gap is half of the posteromedial gap, the tibial slope does not change. For each increase of 1 mm in the anterior gap, there is an increase of 2° in the posterior tibial slope. Marti et al. [62] reported, for every 10° of varus correction by HTO, an average increase in posterior tibial slope of 2.7° and anterior tibial translation of 6 mm; this was also described by Bonnin in 1990 [63]. Naudie et al. [63] reported an average increase in posterior tibial slope of 8° after opening wedge HTO. Giffin et al. [65] demonstrated that, after anterior opening wedge HTO, the posterior tibial slope increases from 8.8 ± 1.8° to 13.2 ± 2.1°, causing anterior translation of the tibia of 3.6 ± 1.4 mm compared with the starting position. Furthermore, forces on PCL decreased from 34 ± 14 N to 19 ± 15 N with the knee flexed at 30° and from 36 ± 29 N to 22 ± 11 N with the knee flexed at 90°; this is a further demonstration that an increase in posterior tibial slope decreases stress forces on posterior structures.
Fig. 4.
Relationship between tibial slope and kind and site of osteotomy
Nakamura et al. [66] compared the effects of dome osteotomy according to Maquet [67] with opening wedge HTO with emicallotaxis, and found a mean decrease in posterior tibial slope of 5.9° with the former technique and of 0.8° with emicallotaxis 1 year after surgery. Some authors [68–70] have suggested that opening wedge HTO with emicallotaxis and external fixator is the treatment that should be chosen to correct malalignment of the lower limbs. Cullù et al. [71] evaluated changes in the posterior tibial slope with four different methods after dome osteotomy and found a mean decrease in posterior tibial slope of 3.3°. Agneskirchner et al. [72] demonstrated that an increase in posterior tibial slope causes a change in the pressure on the articular tibial cartilage: the pressure increases in the anterior portion and decreases in the posterior portion. This could appear strange: if the tibia translates anteriorly, the pressure on posterior articular cartilage should increase; however, the authors [73] underlined that, between 120° of knee flexion and full extension, femoral condyles roll anteriorly on the tibia, shifting the contact point anteriorly. This study suggests a positive effect of increased posterior tibial slope in decreasing forces on the posterior portion of the articular tibial cartilage.
History and physical examination
Because a PCL lesion is associated with a PLC lesion in 60% of cases [47], if a PCL lesion is suspected or detected, we believe it is mandatory to look for a PLC lesion during history-taking and physical examination. Patients with a PCL lesion usually complain about nonspecific symptoms; the mechanism of injury usually reported is a posterior force applied to the tibia with the knee in flexion (football players or a fall on the flexed knee), and hyperextension or hyperflexion with or without a posteriorly directed tibial force [73]. After an acute PLC lesion, patients usually report an impact to the anteromedial aspect of the knee, contact or noncontact hyperextension, and a varus noncontact force. Because 15% of PLC lesion are associated with a common peroneal nerve injury, it is important to ask the patient about numbness, tingling or muscle weakness, especially in ankle dorsiflexion or great toe extension [74]. Because of the biomechanical changes in PLC after a PCL lesion as previously described (see the “Biomechanics” section for further explanation), patients with a chronic PLC lesion usually do not report either a specific trauma or a PCL lesion that might have occurred several years before. A chronic lesion should be suspected during physical examination; gait analysis is useful for detection and should be systematically performed, we believe.
During physical examination it is important to identify all factors involved in posterolateral chronic instability, because they are all related to surgical outcome:
-
Gait is the first factor to analyze. Patients with posterolateral instability often present so-called hyperextension varus thrust gait (see the “Biomechanics” section). Gait analysis is important to detect PLC-associated lesions because, in some cases, patients with hyperextension varus thrust have poorer results than patients with normal gait [20, 35, 36].
Many tests are described in literature to evaluate the function of PCL and PLC (Table 1).
The posterior sag sign was first described by Mayo Robson in 1903 [75] and then modified by Barton et al. [76]; according to Rubistein et al. [77], the test has 79% sensitivity and 100% specificity. The patient lies in supine position with both knees and hip at 90° of flexion while the examiner holds the heels of the patient and compares side by side the posterior translation of the tibia from a lateral view.
The posterior drawer test was first described by Noulis in 1875 [78] and then popularized by Paessler and Michel [79]; according to Rubistein et al. [77], the test has 90% sensitivity and 99% specificity. The patient lies in supine position with the knee at 90° of flexion; the examiner sits on the foot of the patient and applies a posterior force on the anterior tibial shaft, comparing side by side the posterior tibial translation.
The quadriceps contraction test was first described by Daniel et al. in 1988 [80]; according to Rubistein et al. [77], the test has 54% sensitivity and 97% specificity. The patient lies in supine position with the knee in drawer position and is asked to slide the foot down the table. If a PCL lesion is present, the tibia translates anteriorly more than 2 mm during quadriceps contraction.
The dial test, performed in prone and supine position, was described by Loomer in 1991 [81] and then modified by Veltri and Warren [82]. The patient lies in supine position with both thighs supported by a holder or is allowed to hang off the end of the examining table and stabilized by an assistant at 30° of knee flexion. The examiner externally rotates the lower legs and compares the tibial tuberosity external rotation side by side. In prone position an assistant is not needed, and the thigh–foot angle is measured. The test is positive for a PLC lesion if there is an increase of at least 10–15° in comparison with the other knee at 30° of knee flexion. The test is then performed at 90° of flexion; if a further increase in external rotation is present, a PCL lesion is associated.
The external rotation recurvatum test was described by Hughston and Norwood [83] in 1980. The patient lies in supine position with both knees extended. The examiner holds and lifts the great toes of the patient. If a PLC lesion is present, the affected knee hyperextends and goes into varus and in external rotation compared with the contralateral normal knee.
The varus stress test was described by Palmer in 1938 [84] and then modified by Hughston et al. [85]. The knee is at 30° of flexion, and the examiner grasps the thigh of the patient with one hand and the foot or the lower leg with the other hand and applies a varus force to the knee. The amount of lateral compartment opening indicates the grade of LCL lesion: grade I (0–5 mm), grade II (6–10 mm), grade III (>10 mm).
The posterolateral drawer test was first described by Hughston and Norwood in 1980 [86]. The patient lies in supine position with the knee at 90° of flexion and the foot at 15° of external rotation while the examiner posteriorly translates the tibia. If the affected limb translates posteriorly more than the contralateral limb, a popliteus tendon or popliteofibular ligament injury is suspected.
In the reverse pivot shift test [87], the patient lies in supine position with the knee at 70–80° of flexion with the foot externally rotated. If a PLC lesion is present, the tibia is posteriorly subluxated. The knee is subsequently extended, and at 20° of flexion this subluxation reduces spontaneously. According to Cooper [88], the test is positive in 35% of normal knees, especially under anesthesia, so side-to-side comparison is mandatory to evaluate the real amount of instability.
Table 1.
Clinical tests
| Clinical tests | Sensitivity | Specificity |
|---|---|---|
| Posterior sag [77] | 79% | 100% |
| Posterior drawer [77–79] | 90% | 99% |
| Quadriceps contraction [77, 80] | 54% | 97% |
| Dial test [81, 82] | NA | NA |
| External rotation recurvatum [83] | NA | NA |
| Varus stress [83, 84] | NA | NA |
| Posterolateral drawer [86] | NA | NA |
| Reverse pivot shift [87] | NA | NA |
NA not assessed
Because meniscal injuries are associated with acute PCL lesions in 16–28% of cases [44, 46] and with chronic PCL lesions in 36% of cases [45], we believe that specific meniscal tests should be systematically performed. Even if neurovascular function tests are more important in acute injury, they also should be systematically performed in patients with chronic lesions.
Imaging
Dugdale et al. [89] in 1992 proposed a flowchart for radiological evaluation of the patient with a varus of the knee, which was later modified by Noyes et al. [24]. They stated that the patient should get stress X-rays if physical examination reveals any of the following: positive varus stress test, increased varus during thrust, increased tibial external rotation at 30° of knee flexion, or varus recurvatum during standing or walking. If X-rays are positive, the patient should get supine full-length anteroposterior (A-P) X-rays of both legs to evaluate the real alignment. If physical examination reveals none of the aforementioned features, the patient should get full-length double stance A-P X-rays of both legs. If varus deformity is not present, they suggested that the patient should undergo soft tissue reconstruction; if this deformity is present, it is important to evaluate if a lateral joint line opening is associated. If this is the case, the patient should get stress X-rays; if it is not the case, the authors [89] described two methods to evaluate the amount of correction to perform during surgery.
Conventional radiology still has an important role in preoperative planning of patients with a PCL/PLC lesion, especially if associated with a varus of the knee. After the report of Dugdale et al. [89], many other radiographic studies have been published in literature to evaluate alignment of the lower limbs, even in patient with posterolateral instability of the knee. We believe that all these patients should get the following imaging study with standard and stress X-rays (Table 2).
Table 2.
Imaging views
| Standard X-ray | Purpose |
|---|---|
| Full-length double stance A-P X-ray [90] | To evaluate femorotibial alignment |
| Full-length double supine A-P X-ray [90] | To eliminate the added varus due to deficiency of the lateral and PL structures |
| Real lateral view X-ray [21, 49, 71, 91] | To evaluate posterior tibial slope |
| Merchant’s view X-ray [92] | To evaluate patellofemoral joint |
| Rosemberg’s view [93] | To evaluate the lateral compartment of the knee |
| Stress X-ray | Purpose |
|---|---|
| Lateral stress view according to the Telos method [94] | To evaluate anterior and posterior tibial translation with regards to the femur |
| Lateral stress view according to the kneeling method [96] | To evaluate anterior and posterior tibial translation with regards to the femur |
| Lateral stress view with hamstring contraction method [97] | To evaluate anterior and posterior tibial translation with regards to the femur |
| Lateral stress view according to gravity method [99] | To evaluate anterior and posterior tibial translation with regards to the femur |
| Axial stress view [100] | To evaluate anterior and posterior tibial translation with regards to the femur |
Standard X-ray
Full-length double stance A-P X-ray is mandatory to evaluate femorotibial alignment, as described by Moreland et al. [90]. An A-P X-ray is taken from the hips to the ankles with the patient standing and the patellae looking forward using a suitable cassette to gradually filter the X-ray beam in order to visualize both hips and ankles properly. Dugdale et al. [89] proposed two methods to quantify the amount of correction to perform if malalignment is present. In both methods, a line along the tibial plateau and its intersection with the desired mechanical axis of the lower extremity are marked; in this section this point is called P for simplicity (see the “Indications and contraindications” and “Discussion” sections for further explanation about the position of P in each patient). Then, a line is traced from the center of the femoral head to P and a line is traced from the center of the tibiotalar joint to P. In the first method the angle formed at the intersection between these two lines represents the amount of correction required (Fig. 5). In the second method the radiographic film is cut along the osteotomy line and along a vertical line that converges with the first, leaving a 2-mm hinge at the medial tibial margin; the distal part of the film is rotated until the femoral head, P, and the tibiotalar joint are along the same line; the overlapping wedge margin is the amount of correction to perform. The authors [89] also demonstrated that, if lateral and/or posterolateral soft tissue structures are insufficient, for every increase of 1 mm in the lateral joint line width, there is 1° of added varus. Supine X-rays are important to eliminate the added varus due to deficiency of the lateral and/or posterolateral structures and to evaluate the real amount of correction to perform. The authors [89] also demonstrated that, after HTO, the mechanical axis of the lower extremity is translated laterally by 3–4 mm for each 1° of valgus correction and that this value depends on the height of the patient.
Fig. 5.

The angle α represents the correction required
Real lateral view X-ray is used to evaluate posterior tibial slope. In literature many methods are described to quantify its value (Fig. 6a–e). Dejour and Bonnin [21] recommend to trace a line along the proximal tibial anatomical axis (PTAA) and a line along the tibial plateau, the angle between these two lines being the tibial slope. In 1974, Moore and Harvey [91] described the tibial plateau angle, recommending to trace a line along the anterior tibial cortex (ATC) and a line along the medial tibial plateau, the angle between these two lines being the tibial slope. Brazier et al. [49] proposed three other methods. In the first, a line is traced along the posterior tibial cortex (PTC) and a line is traced along the medial tibial plateau, the angle between these two lines being the tibial slope. In the second, they recommend to trace a line along the proximal fibular anatomical axis (PFAA) and a line along the medial tibial plateau, the angle between these two lines being the tibial slope. In the third, they trace a line along the fibular shaft axis (FSA) and a line along the medial tibial plateau, the angle between these two lines being the tibial slope. The same authors compared all these techniques and stated that the most reliable are the PTAA and PTC methods. Cullù et al. [71] compared the various methods and found for the same patients higher values using the method described by Moore and Harvey [91] and lower values with PFAA [49].
Fig. 6.
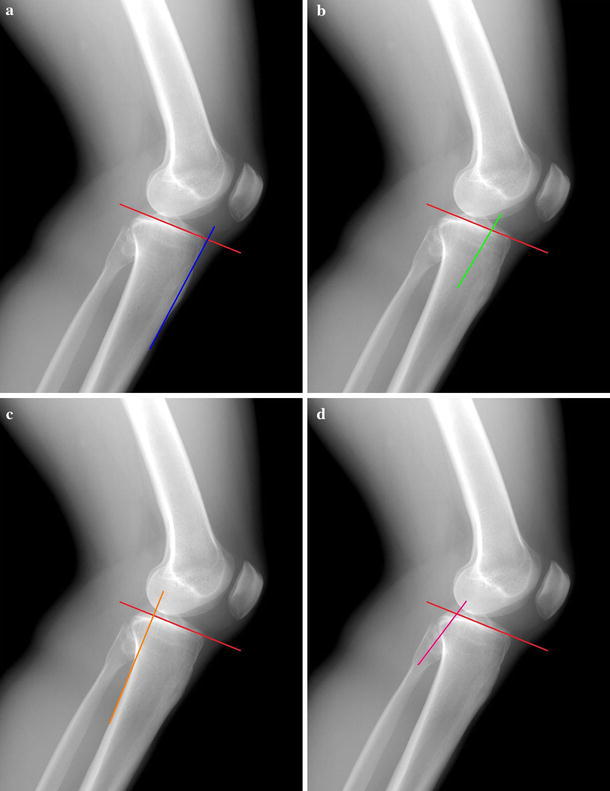
Schematic representation of the radiographic methods for evaluation of posterior tibial slope: aATC anterior tibial cortex, bPTAA proximal tibial anatomical axis, cPTC posterior tibial cortex, dPFAA proximal fibular anatomical axis, eFSA fibular shaft axis
Merchant’s view, described in 1974 [92], is useful to evaluate the patellofemoral joint, which in these patients undergoes degenerative changes, as mentioned above. The patient lies in supine position with the knees at 45° of flexion over the end of the table; the knees are held to maintain the femora parallel to the horizontal. The X-ray collimator is placed above the patient, and the beam is directed proximal to distal, forming a 30° angle with the table. The film cassette is placed about 30 cm below the knees, perpendicular to the tibial shaft.
Rosemberg’s view, described in 1988 [93], is useful to evaluate the lateral compartment of the knee. The patient stands on both legs with thumbs pointing ahead and the patellae touching the film cassette. The knees are at 45° of flexion (25° between the femora and the cassette, and 20° between the tibiae and the cassette), and the X-ray beam is directed posterior to anterior, 10° caudal, so the posterior and the anterior margins of the tibial plateau are superimposed.
Stress X-ray
The lateral stress view according to the Telos method was first described by Jacobsen in 1976 [94]. The patient lies in lateral decubitus position with the knee flexed at 90° and is encouraged to relax. The heel is fixed to a stand, and the arm of the Telos GA II (Telos, Weterstadt, Germany) applies a posterior force to the tibia. In this position, a lateral X-ray is taken. The test is then performed with the knee at 25° of flexion [94]. This method is very important in chronic PCL-deficient knees to evaluate both anterior and posterior tibial translation with regards to the femur, and it is useful to detect fixed posterior tibial subluxation, as described in 2002 by Strobel et al. [95], according to whom it is present in 44% of patients with a PCL lesion.
In the lateral stress view according to the kneeling method [96], the patient knees on a bench with the knee at 90° of flexion; the bench only supports the lower legs up to the tibial tubercle. In this position a lateral X-ray is taken [96].
The lateral stress view with hamstring contraction was described by Chassaing et al. [97] in 1995. The patient lies in lateral decubitus or is in seated position with the knee at 90° of flexion and the heel fixed to a stand. A lateral X-ray is taken while the patient contracts his/her hamstring for at least 10 s [97, 98].
The lateral stress view according to gravity method was described by Staubli and Jacob in 1990 [99]. The patient lies in supine position with the hip and the knee at 90° of flexion, supported by an assistant, with the leg in neutral rotation. In this position, a lateral X-ray is taken.
The axial stress view was described by Puddu et al. [100] in 2000. The patient lies in supine position with both knees at 70° of flexion, feet plantigrade in moderate plantar flexion, and the tibia in neutral rotation. The X-ray beam is directed parallel to the longitudinal patellar axis, from distal to proximal, and the distance between the anterior tibial profile and the center of the femoral groove is measured. The side-to-side difference is the amount of posterior instability.
In 2003, Margheritini et al. [101] compared, with regard to posterior translation, the Telos method with the knee flexed at 25° and 90°, the hamstring contraction method, the gravity view method, and the axial stress view, stating that the most effective methods are Telos view at 90° of knee flexion and hamstring contraction. More recently, Jung et al. in 2006 [98] compared all five of these methods, focusing on posterior translation, side-to-side difference, condyle rotation, time to perform the test, and pain during the test. Considering all these factors, they stated that the most effective methods are Telos view at 90° of knee flexion and the kneeling method, even if they are painful and time-consuming procedures, and Telos is the most expensive but most reliable in detecting posterior tibial subluxation.
MRI
Magnetic resonance imaging (MRI) is useful to evaluate PCL-deficient knees, especially associated lesions and subchondral bone [102]. In 1992, Gross et al. [103] described a classification for PCL lesions that is widely used; however, in 2006, Bellelli et al. [104] proposed a new MRI classification that considers each PCL bundle independently, emphasizing the importance of spin echo (SE) T2 and short T1 inversion recovery (STIR) sequences. To evaluate PLC, LaPrade and Wentorf [12] recommend use of at least 1.5-T MRI scanner. Furthermore, Yu et al. [105] emphasized that using coronal oblique sections (parallel to the popliteus tendon) significantly increases the ability to detect some structures of PLC (i.e., fabellofibular ligament and popliteofibular ligament). LaPrade et al. [106] recommended to use thin-slice (2 mm) proton density coronal oblique sequences to evaluate LCL and popliteus tendon.
Indications and contraindications
In this paper only indications for HTO are discussed; the reader is advised to consult specific literature for indications for conservative treatment and soft tissue procedures.
Incorrect indication is most common, so surgery must be preceded by accurate preoperative planning.
Contraindications to HTO are: inflammatory disease, severe osteoporosis, high body mass index (BMI) (relative contraindication), age greater than 65 years (relative), severe tricompartmental OA, severe medial compartment OA, severe lateral compartment OA, and severe patellofemoral OA (relative).
PCL and PLC lesions are often associated with malalignment of the knee [47], and they should be corrected 6–8 months after HTO (if the knee is still unstable). In literature, poor results for soft tissue procedures alone are reported; this is due to the forces on these structures, which do not decrease if malalignment is not corrected, because bone deformity overstresses them. Instead, HTO reduces these forces and improves the stability and biomechanics of the knee (see the “Biomechanics” section for further explanation).
If femorotibial OA is present, with narrowing of the medial compartment, the point called P in the “Imaging” section should be positioned at 62–66% of the tibial plateau (where 0% indicates the medial margin of the tibial plateau and 100% the lateral margin). This position increases the pressure on the lateral compartment of the knee (most of the weight of the patient bears on the lateral articular cartilage) [28, 68, 89]; indeed, a small overcorrection prevents progression of medial compartment OA and early recurrence of varus deformity [28, 107]. If degenerative narrowing of the medial compartment is not present, the new mechanical axis should split the tibial plateau in two halves [28]. Medial opening wedge HTO improves symptoms of patellofemoral OA because the anterior translation of the tibia reduces the tension on the patellar tendon, the patella becomes less horizontal, and pressure decreases in the lateral facet [38, 39]. So, a patellofemoral pain syndrome is not a contraindication to HTO.
Strobel et al. [95] classified fixed posterior tibial subluxation in three grades: I (3–5 mm), II (6–10 mm), III (>10 mm). In grades I and II, they recommend a brace in extension with a support under the calf to push the tibia anteriorly (Medi Bayreuth, Bayreuth, Germany), because they had good results in 78.4% and 70.1% of patients, respectively. In patients with a grade III lesion, conservative treatment has yielded acceptable result in only 32%, so they recommend surgical treatment. If fixed tibial subluxation is present, they also recommend (especially in soft tissue procedures) to reduce the subluxation before performing any surgical treatment, to avoid overstress of the graft and early failure. HTO modifies the tibial slope, provokes the tibia to translate anteriorly, and reduces this subluxation. Subsequently, if the knee is still unstable, PCL could be reconstructed.
If meniscal lesions are associated, they should be addressed at the same time of HTO.
Some authors [68–70] have suggested that opening wedge HTO with emicallotasis and external fixator is the treatment that should be chosen to correct the malalignment; however, we prefer to use this technique with a circular external fixator (Taylor Spatial Frame; Smith and Nephew, Memphis, TN) only in deformities that need correction greater than 12.5°. If an external fixator is applied, the osteotomy is performed distal to the tibial tubercle and does not change patellar height; instead, medial opening wedge HTO is performed proximal to the tibial tubercle, and if the gap is too large, patella infera (baja) may occur. This circular external fixator has a computer program that aims to achieve triplanar correction of the deformity and correct also the tibial slope in the sagittal plane [108]. An external fixator enables slow correction of the deformity, improving consolidation of even large osteotomy gaps. An external fixator could also be used for treatment of failed medial opening wedge HTO [109].
According to Noyes et al. [24], a preoperative rehabilitation protocol (strengthening of the muscles of the lower limbs and gait retraining) is needed to avoid recurrence of hyperextension varus thrust gait after surgery.
HTO and ACL reconstruction are often associated, and good results are reported even in knees with double varus. If triple varus is present, HTO should be performed before soft tissue reconstruction, in order to avoid a long surgery and increased risk of postoperative complications [24]. We do not have enough patients for statistical analysis, but in our clinical experience, in the patient with a chronic PCL-deficient knee associated with double or triple varus, HTO should be performed before soft tissue procedures. The patient should be evaluated 6–8 months later, and if the knee is still unstable, soft tissue reconstruction should be performed.
Treatment
According to Maquet [67], closing wedge lateral HTO and dome osteotomy slightly decrease the tibial slope and are not useful in treatment of a PCL/PLC-deficient knee. Because opening wedge medial HTO and HTO with external fixator enable the surgeon to modify the tibial slope, they are the only osteotomies that can be performed in patients with a PCL/PLC-deficient knee, and only these osteotomies are discussed in this section. For the description of lateral HTO, dome osteotomy, and soft tissue procedures, the reader is advised to consult the specific literature.
All patients should receive a prophylactic preoperative dose of intravenous antibiotics; general endotracheal anesthesia should be preferred, because it allows the surgeon to get a bone block from the iliac crest, if needed. The patient lies in supine position, and the leg is draped in sterile fashion; if a bone block is needed, the ipsilateral iliac crest is draped in the same fashion. Arthroscopy is performed in all patients to evaluate articular cartilage and menisci and to confirm the indication for HTO [16, 28, 48].
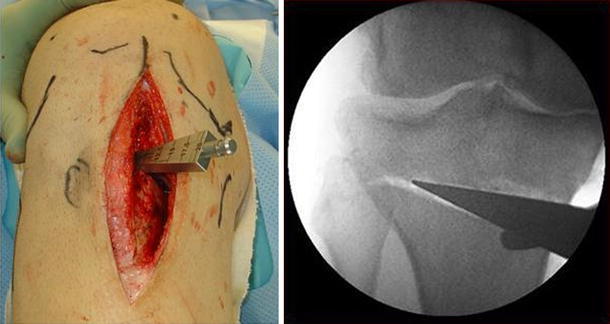
If a plate is used to stabilize the osteotomy, the leg is raised and tourniquet is inflated. A vertical incision is performed just behind the pes anserine, between the medial border of the patellar tendon and the posterior border of the tibia. Sartorius fascia is cut to visualize hamstring tendons. Under fluoroscopic control, a guide wire is positioned from medial to lateral. The wire is placed at the level of the superior aspect of the tibial tubercle, anteromedially, and it arrives about 1 cm below the lateral articular margin of the tibia (Fig. 7). A cortical osteotomy is performed with an oscillating saw, inferiorly to the guide wire, and it will be continued with an osteotome under fluoroscopic control (Fig. 8). When the osteotomy is completed, the medial tibia is opened with a wedge of suitable width (Fig. 9). Wedges have a graduated scale to quantify the angular correction achieved [16, 28, 48]. The position of the wedge is very important in order to correct the deformity in the sagittal plane: a wedge placed anteriorly causes an increase in posterior tibial slope, whereas a posterior wedge tends to slightly decrease the posterior tibial slope [61]. Anterior and posterior gaps of the osteotomy are then measured with a ruler; this is important to calculate the amount of increase in posterior tibial slope after surgery, as described by Noyes et al. [59]. If the anteromedial gap is half of the posteromedial gap, the slope will not change; for each 1 mm of increase of the anterior gap, the posterior tibial slope will increase by 2°. An image intensifier and an alignment rod are used to control coronal and sagittal alignment during axial loading of the joint [28] (Fig. 10). If the anterior gap is greater than 1 cm, it is better to perform an osteotomy to lift the tibial tubercle by the same amount to avoid patella infera (baja). Generally, to fill the osteotomy gap, a carefully shaped bone block from a donor is used (Fig. 11). When correction in the two planes is achieved, the osteotomy is stabilized using a plate with four holes (Arthex, Naples, FL, USA) with two 6.5-mm proximal cancellous screws and two 4.5-mm distal cortical screws (Fig. 12). Under fluoroscopic control, the final result is checked before the tourniquet is deflated; hemostatis and skin suture are then performed [16, 28, 48].
Fig. 7.
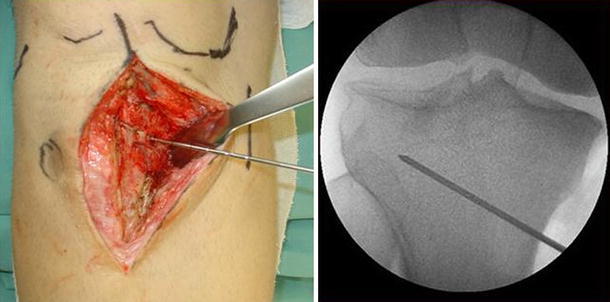
A guide wire is placed from the superior aspect of the tibial tubercle to about 1 cm below the lateral articular margin of the tibia
Fig. 8.
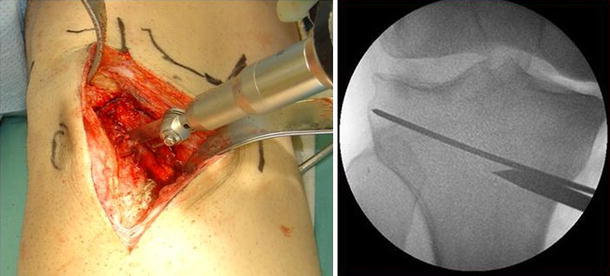
Cortical osteotomy is performed with an oscillating saw, inferior to the guide wire, and it will be continued with an osteotome
Fig. 9.
When the osteotomy is completed, the medial tibia is opened with a wedge of suitable width
Fig. 10.

An image intensifier and an alignment rod are used to control coronal and sagittal alignment during axial loading of the joint
Fig. 11.

To fill the osteotomy gap, a carefully shaped bone block from a donor is used
Fig. 12.
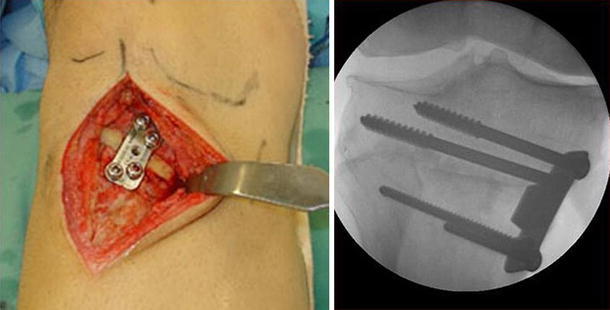
When correction in the two planes is achieved, the osteotomy is stabilized using a plate with four screws
If an external fixator is used for treatment, it is assembled preoperatively on the leg of the patient. Three rings, 4 cm larger than the diameter of the tibia, are used. The first is positioned at the level of the fibular head, the second 5 cm below the tibial tubercle, and the third 3 cm proximal to the ankle joint. The first and the second ring are joined with two tethered rods, and the second and the third rings are joined with four tethered rods. The proximal ring is held at an angle equal to the correction needed plus 5° (to give some overcorrection). The apparatus is then sterilized [108]. During surgery, a tourniquet is not needed. A 3-cm incision is made 10 cm below the fibular head posterolaterally, the plane between soleus and peronei is developed, and an oblique fibular osteotomy is performed with an oscillating saw. The external fixator is then applied to the leg of the patient, and the first ring is stabilized with two wires and one half-pin across the tibia. The second ring is stabilized with one wire and one half-pin across the tibia; it is important to avoid transfixing the branches of the superficial peroneal nerve, so the wire should be placed slightly more laterally than the medial aspect of the tibia. The third ring is stabilized with two wires that pass across the tibia and the fibula to avoid distal tibiofibular subluxation. Then, a 1.5-cm incision is performed anteriorly just distal to the tibial tuberosity, periosteum is elevated on both sides, and a tibial osteotomy is performed with an oscillating saw, a drill, a Gigli saw or an osteotome [108]. The required correction can be achieved acutely during surgery by rotating the first two rings until they are parallel to each other [108]. Otherwise, if the osteotomy gap is too large, the correction can be performed gradually, beginning on the 7–10th postoperative day, with emicallotaxis technique [68–70]. The result is verified under image intensifier, a small amount of compression is performed, the rods are tightened, and the skin is closed [68–70, 108]. The amount of posterior tibial slope increase should be 2–8° to avoid ACL overstress and pressure increase on anterior tibial articular cartilage [72, 73].
Postoperative protocol
The patient should be encouraged not to drink alcohol or smoke. If a plate is used to stabilize the osteotomy, the knee is protected for 6 weeks in an articulated brace. During this period, the patient carries out exercises aimed at completely regaining range of motion and reinforcing “core stability” [110]. Only toe-touch gait with crutches is allowed. After 6 weeks, if there are no problems at X-ray control, the patient is encouraged to increase weight-bearing progressively until 12 weeks, at which time a second X-ray control is recommended [7]. If a circular external fixator is applied, partial weight-bearing is allowed immediately without any brace [108].
Discussion
Clinical tests for diagnosis of PCL and PLC lesions have low sensitivity and, in some cases, also low specificity; for these reasons, we advise the clinician to perform all the tests described in this paper to rule out such lesions. We believe that, during physical examination, it is important to look for meniscal and neurovascular lesions, because they are often associated [44–46]. Complete history-taking and physical examination are mandatory in evaluation of all patients, but in a patient with a PCL/PLC lesion, associated with varus malalignment, they have particular value.
All radiographic methods described to evaluate the posterior tibial slope need to trace a line along the medial tibial plateau. This is an easy and reproducible procedure on the medial plateau because it is flat, whereas the lateral tibial plateau is convex and cannot be easily used to quantify the posterior tibial slope. We agree with Jung et al. [98] that the most effective stress X-rays are Telos at 90° of knee flexion and the kneeling method. These authors considered also compliance and patient pain, which are important factors that could influence the results of these examinations. Although the Telos method at 90° of knee flexion is the most painful, time consuming, and expensive, it is the most reliable for evaluation of fixed posterior tibial subluxation. The kneeling method could be an effective and less expensive option, but if fixed posterior tibial subluxation is present, the Telos method should be preferred [98].
Yu et al. [105] reported that fabellofibular ligament, arcuate ligament, and popliteus tendon are difficult to visualize on MRI, and also with coronal oblique sections, less that half of these structures could be imaged. LaPrade et al. [106] demonstrated that the sensitivity of a 1.5-T MRI scanner for diagnosis of a PLC lesion is 66.7–100% and specificity is 66.7–100%, depending on the anatomical structures. Use of coronal, sagittal, and coronal oblique sections and several different MRI sequences is important to increase the ability to detect lesions of these structures. At least a 1.5-T MRI scanner should be used to evaluate a knee with a suspected PLC lesion [12]. Several papers [12, 105, 106] suggest that MRI diagnosis of a PCL lesion is difficult, even with the most advanced technologies. We believe that stress radiographs are mandatory in evaluation of an unstable knee but do not help the clinician to identify the injured structures. MRI does not solve this problem, because it cannot fully visualize posterolateral structures in at least 50% of patients [105]. This is still a problem in PLC lesion diagnosis.
In literature, there are different positions described for the mechanical axis of the lower extremity after HTO. In agreement with Noyes et al. [28], we suggest that, if narrowing of the medial compartment is present, the mechanical axis should be placed laterally to the center of the knee (most of the weight of the patient bears on the lateral articular cartilage). A small valgus hypercorrection is needed to avoid early recurrence of the deformity [28, 107]. If OA of the medial compartment is not present, the mechanical axis should cross the center of the knee.
There are three causes of failure of HTO in a varus knee: inability to correct the deformity during surgery, a “tibial teeter-totter effect” (advanced medial tibiofemoral OA and obliquity), and gradual collapse of the medial compartment over years, in which the overall alignment drifts back to varus because of continued medial tibiofemoral OA [28].
Medial opening wedge HTO has some disadvantages such as an unstable construct, implant failure, delayed union, and nonunions. During surgery, it is impossible to predict exactly the position of the mechanical axis during weight-bearing, and overcorrection may occur, requiring revisional surgery [28].
Some authors [7–10] have underlined that soft tissue techniques alone, without correction of the alignment of the lower limbs, often give poor results, because bone deformity overstresses these structures. Other studies [7, 12–15] have underlined that reconstruction of the PCL without repair or reconstruction of the PLC often gives poor results. Some authors [5, 6, 8, 16–18] have reported satisfactory results after HTO for unicompartmental OA and varus alignment, whereas there are few studies about the results of HTO in the unstable knee [10, 18, 19, 28]. However, in the last 10 years, there has been increasing interest in HTO for treatment of chronic knee instability, because HTO makes it possible to correct both coronal and sagittal deformities. This has occurred because changes in posterior tibial slope (sagittal plane) cause changes in knee biomechanics and in joint stability. An increase in posterior tibial slope causes anterior tibial translation about the femur and stabilizes a knee with posterior instability [21, 63]. Some studies [22, 56–59] have demonstrated that closing wedge HTO causes a decrease in posterior tibial slope, whereas opening wedge HTO causes an increase in posterior tibial slope with anterior tibial translation [13, 61–65]. For these reasons, some authors [19–24] suggest to perform closing wedge HTO in a varus chronic ACL-deficient knee. Furthermore, HTO associated with ACL reconstruction showed good results in young patients with varus malalignment and ACL lesions [21, 22, 24–27]. Other studies [24, 61–65] have underlined the efficacy of opening wedge HTO in the varus chronic PCL-deficient knee, associated or not with a PLC lesion. In agreement with other authors [64], in the varus chronic PCL-deficient knee, associated or not with a PLC lesion, we suggest to perform opening wedge medial HTO to correct varus deformity and increase tibial slope. After 6–8 months, if the knee is still unstable, we suggest to perform soft tissue reconstruction. We believe that evaluation of the deformity in the coronal and sagittal planes is essential for treatment of a complex instability of the knee, and before performing any kind of soft tissue surgery, correct bone alignment should be obtained, in both coronal and sagittal planes.
HTO with an external fixator and emicallotaxis does not modify patellar height, and it enables deformity correction independently in the coronal and sagittal planes. The patient can walk earlier, weight-bearing X-rays can be obtained to evaluate alignment of the lower limbs, the mechanical axis can be corrected at any time during the elongation phase if needed without a second surgery being performed, and a tourniquet is not needed at time of surgery. However, the external fixator is uncomfortable for the patient and is not easy to wear under normal clothes, and pin tract infection may occur. Because the external fixator is not rigid, 5° of overcorrection reduces the failure rate in case of loss of correction [108].
For these reasons, we suggest HTO with an external fixator only if correction greater than 12.5° is needed, because medial opening wedge HTO in these cases is associated with a higher rate of complications such as delayed unions, nonunions, and unstable osteotomy, due to too large an osteotomy gap [108, 109].
Conclusions
HTO is an effective and reliable procedure for treatment of the PCL/PLC-deficient knee associated with varus malalignment. If the knee is still unstable, soft tissue procedures should be performed 6–8 months after correction of the malalignment. HTO allows the surgeon to modify both the coronal and the sagittal plane of the knee; an increased posterior tibial slope stabilizes the joint, and reduces forces on posterolateral structures and on posterior articular cartilage. However, more biomechanical and clinical studies are needed in the future.
Acknowledgments
The authors would like to thank Valeria Radini for help in preparation of the manuscript.
Conflict of interest
None.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
References
- 1.Fujisawa Y, Masuhara K, Shiomi S. The effect of high tibial osteotomy on osteoarthritis of the knee. An arthroscopic study of 54 knee joints. Orthop Clin North Am. 1979;10:585–608. [PubMed] [Google Scholar]
- 2.Odenbring S, Egund N, Lindstrand A, Lohmander LS, Willen H. Cartilage regeneration after proximal tibial osteotomy for medial gonarthrosis. An arthroscopic, roentgenographic, and histologic study. Clin Orthop Relat Res. 1992;277:210–216. [PubMed] [Google Scholar]
- 3.Noyes FR, Barber-Westin SD, Rankin M. Meniscal transplantation in symptomatic patients less than 50 years old. J Bone Joint Surg Am. 2004;86:1392–1404. doi: 10.2106/00004623-200407000-00006. [DOI] [PubMed] [Google Scholar]
- 4.Coventry MB, Ilstrup DM, Wallrichs SL. Proximal tibial osteotomy: a critical long-term study of 87 cases. J Bone Joint Surg Am. 1993;75:196–201. doi: 10.2106/00004623-199302000-00006. [DOI] [PubMed] [Google Scholar]
- 5.Naudie D, Bourne RB, Rorabeck CH, Bourne TJ. The install award. Survivorship of the high tibial valgus osteotomy. A 10–22 year followup study. Clin Orthop Relat Res. 1999;367:18–27. [PubMed] [Google Scholar]
- 6.Camarda L, Condello V, Madonna V, Cortese F, D’Arienzo M, Zorzi C. Results of isolated posterolateral corner reconstruction. J Orthop Traumatol. 2010;11(2):73–79. doi: 10.1007/s10195-010-0088-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Christel P. Basic principles for surgical reconstruction of the PCL in chronic posterior knee instability. Knee Surg Sports Traumatol Arthrosc. 2003;11:289–296. doi: 10.1007/s00167-003-0407-2. [DOI] [PubMed] [Google Scholar]
- 8.Insall JN, Joseph DM, Msika C. High tibial osteotomy for varus gonarthritis. A long-term follow-up study. J Bone Joint Surg Am. 1984;66:1040–1048. [PubMed] [Google Scholar]
- 9.Neyret P, Donell ST, Dejour H. Results of partial meniscectomy related to the state of the anterior cruciate ligament. Review at 20–35 years. J Bone Joint Surg Br. 1993;75:36–40. doi: 10.1302/0301-620X.75B1.8421030. [DOI] [PubMed] [Google Scholar]
- 10.Goradia VK, Van Allen J. Chronic lateral knee instability treated with a high tibial osteotomy. Arthroscopy. 2002;18:807–811. doi: 10.1053/jars.2002.35270. [DOI] [PubMed] [Google Scholar]
- 11.Lephart SM, Pincivero DM, Rozzi SL. Proprioception of the ankle and knee. Sports Med. 1998;25:149–155. doi: 10.2165/00007256-199825030-00002. [DOI] [PubMed] [Google Scholar]
- 12.LaPrade RF, Wentorf F. Diagnosis and treatment of posterolateral knee injuries. Clin Orthop Relat Res. 2002;402:110–121. doi: 10.1097/00003086-200209000-00010. [DOI] [PubMed] [Google Scholar]
- 13.Noyes FR, Goebel SX, West J. Opening wedge tibial osteotomy: the 3-triangle method to correct axial alignment and tibial slope. Am J Sports Med. 2005;33:378–387. doi: 10.1177/0363546504269034. [DOI] [PubMed] [Google Scholar]
- 14.Strobel MJ, Weiler A, Eichhorn HJ. Diagnosis and therapy of fresh and chronic posterior cruciate ligament lesions. Chirurg. 2000;71:1066–1081. doi: 10.1007/s001040051182. [DOI] [PubMed] [Google Scholar]
- 15.Krudwig WK, Witzel U, Ullrich K. Posterolateral aspect and stability of the knee joint. II. Posterolateral instability and effect of isolated and combined posterolateral reconstruction on knee stability: a biomechanical study. Knee Surg Sports Traumatol Arthrosc. 2002;10:91–95. doi: 10.1007/s00167-001-0269-4. [DOI] [PubMed] [Google Scholar]
- 16.Hernigou P, Medevielle D, Debeyre J, Goutallier D. Proximal tibial osteotomy for osteoarthritis with varus deformity. A 10–13 year follow-up study. J Bone Joint Surg Am. 1987;69:332–354. [PubMed] [Google Scholar]
- 17.Nagel A, Insall JN, Scuderi GR. Proximal tibial osteotomy: a subjective outcome study. J Bone Joint Surg Am. 1996;78:1353–1358. doi: 10.2106/00004623-199609000-00009. [DOI] [PubMed] [Google Scholar]
- 18.Badhe NP, Forster IW. High tibial osteotomy in knee instability: the rationale of treatment and early results. Knee Surg Sports Traumtol Arthrosc. 2002;10:38–43. doi: 10.1007/s001670100244. [DOI] [PubMed] [Google Scholar]
- 19.Fowler PJ, Kirkley A, Roe J. Osteotomy of the proximal tibia in the treatment of chronic anterior cruciate ligament insufficiency. J Bone Joint Surg Br. 1994;76B(Supp):26. [Google Scholar]
- 20.Noyes FR, Dunworth LA, Andriacchi TP, Andrews M, Hewett TE. Knee hyperextension gait abnormalities in unstable knees. Recognition and preoperative gait retraining. Am J Sports Med. 1996;24:35–45. doi: 10.1177/036354659602400107. [DOI] [PubMed] [Google Scholar]
- 21.Dejour H, Bonnin M. Tibial translation after anterior cruciate ligament rupture. Two radiological tests compared. J Bone Joint Surg Br. 1994;76:745–749. [PubMed] [Google Scholar]
- 22.Lerat JL, Moyen B, Garin C, Mandrino A, Besse JL, Brunet-Guedj E. Anterior laxity and internal arthritis of the knee. Results of the reconstruction of the anterior cruciate ligament associated with tibial osteotomy. Rev Chir Orthop Reparatrice Appar Mot. 1993;79:365–374. [PubMed] [Google Scholar]
- 23.Dejour H, Neyret P, Bonnin M. Instability and osteoarthritis. In: Fu FH, Harner CD, Vince KG, editors. Knee surgery. Baltimore: Williams & Wilkins; 1994. pp. 859–875. [Google Scholar]
- 24.Noyes FR, Barber-Westin SD, Hewett TE. High tibial osteotomy and ligament reconstruction for varus angulated anterior cruciate ligament-deficient knees. Am J Sports Med. 2000;28:282–296. doi: 10.1177/03635465000280030201. [DOI] [PubMed] [Google Scholar]
- 25.Lattermann C, Jakob RP. High tibial osteotomy alone or combined with ligament reconstruction in anterior cruciate ligament-deficient knees. Knee Surg Sports Traumatol Arthrosc. 1996;4:32–38. doi: 10.1007/BF01565995. [DOI] [PubMed] [Google Scholar]
- 26.Neuschwander DC, Drez D, Jr, Paine RM. Simultaneous high tibial osteotomy and ACL reconstruction for combined genu varum and symptomatic ACL tear. Orthopedics. 1993;16:679–684. doi: 10.3928/0147-7447-19930601-08. [DOI] [PubMed] [Google Scholar]
- 27.Noyes FR, Barber-Westin SD, Simon R. High tibial osteotomy and ligament reconstruction in varus angulated, anterior cruciate ligament-deficient knees. A 2–7 year follow-up study. Am J Sports Med. 1993;21:2–12. doi: 10.1177/036354659302100102. [DOI] [PubMed] [Google Scholar]
- 28.Noyes FR, Barber-Westin SD, Hewett TE. High tibial osteotomy and ligament reconstruction for varus angulated anterior cruciate ligament-deficient knees. Am J Sports Med. 2000;28:282–296. doi: 10.1177/03635465000280030201. [DOI] [PubMed] [Google Scholar]
- 29.Hoppenfeld S, deBoer P (2003) The tibia and fibula. In: Surgical exposures in orthopaedics: the anatomic approach, 3rd edn. Lippincott, Williams & Wilkins
- 30.Ahmad CS, Cohen ZA, Levine WN, Gardner TR, Ateshian GA, Mow VC. Codominance of the individual posterior cruciate ligament bundles. An analysis of bundle lengths and orientation. Am J Sports Med. 2003;31:221–225. doi: 10.1177/03635465030310021101. [DOI] [PubMed] [Google Scholar]
- 31.Takahashi M, Matsubara T, Doi M, Suzuki D, Nagano A. Anatomical study of the femoral and tibial insertions of the anterolateral and posteromedial bundles of human posterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc. 2006;14:1055–1059. doi: 10.1007/s00167-006-0192-9. [DOI] [PubMed] [Google Scholar]
- 32.Amis AA, Gupte CM, Bull AM, Edwards A. Anatomy of the posterior cruciate ligament and the meniscofemoral ligaments. Knee Surg Sports Traumatol Arthrosc. 2006;14:257–263. doi: 10.1007/s00167-005-0686-x. [DOI] [PubMed] [Google Scholar]
- 33.Seebacher JR, Inglis AE, Marshall JL, Warren RF. The structure of the posterolateral aspect of the knee. J Bone Joint Surg Am. 1982;64:536–541. [PubMed] [Google Scholar]
- 34.Paley DR. Principles of deformity correction. berlin: Springer; 1992. [Google Scholar]
- 35.Miller MD, Cooper DE, Fanelli GC, Harner CD, LaPrade RF. Posterior cruciate ligament: current concepts. Instr Course Lect. 2002;51:347–351. [PubMed] [Google Scholar]
- 36.Chang A, Hayes K, Dunlop D, Hurwitz D, Song J, Cahue S, Genge R, Sharma L. Thrust during ambulation and the progression of knee osteoarthritis. Arthritis Rheum. 2004;50:3897–3903. doi: 10.1002/art.20657. [DOI] [PubMed] [Google Scholar]
- 37.Hoher J, Harner CD, Vogrin TM, Baek GH, Carlin GJ, Woo SL. In situ forces in the posterolateral structures of the knee under posterior tibial loading in the intact and posterior cruciate ligament-deficient knee. J Orthop Res. 1998;16:675–681. doi: 10.1002/jor.1100160608. [DOI] [PubMed] [Google Scholar]
- 38.Li G, Gill TJ, DeFrate LE, Zayontz S, Glatt V, Zarins B. Biomechanical consequences of PCL deficiency in the knee under simulated muscle loads-an in vitro experimental study. J Orthop Res. 2002;20:887–892. doi: 10.1016/S0736-0266(01)00184-X. [DOI] [PubMed] [Google Scholar]
- 39.Kumagai M, Mizuno Y, Mattessich SM, Elias JJ, Cosgarea AJ, Chao EY. Posterior cruciate ligament rupture alters in vitro knee kinematics. Clin Orthop Relat Res. 2002;395:241–248. doi: 10.1097/00003086-200202000-00029. [DOI] [PubMed] [Google Scholar]
- 40.Safran MR, Allen AA, Lephart SM, Borsa PA, Fu FH, Harner CD. Proprioception in the posterior cruciate ligament deficient knee. Knee Surg Sports Traumatol Arthrosc. 1999;7:310–317. doi: 10.1007/s001670050169. [DOI] [PubMed] [Google Scholar]
- 41.Skyhar MJ, Warren RF, Ortiz GJ, Schwartz E, Otis JC. The effects of sectioning of the posterior cruciate ligament and the posterolateral complex on the articular contact pressures within the knee. J Bone Joint Surg Am. 1993;75:694–699. doi: 10.2106/00004623-199305000-00008. [DOI] [PubMed] [Google Scholar]
- 42.Ramaniraka NA, Terrier A, Theumann N, Siegrist O. Effects of the posterior cruciate ligament reconstruction on the biomechanics of the knee joint: a finite element analysis. Clin Biomech (Bristol, Avon) 2005;20:434–442. doi: 10.1016/j.clinbiomech.2004.11.014. [DOI] [PubMed] [Google Scholar]
- 43.Ochi M, Murao T, Sumen Y, Kobayashi K, Adachi N. Isolated posterior cruciate ligament insufficiency induces morphological changes of anterior cruciate ligament collagen fibrils. Arthroscopy. 1999;15:292–296. doi: 10.1016/s0749-8063(99)70037-x. [DOI] [PubMed] [Google Scholar]
- 44.Fowler PJ, Messieh SS. Isolated posterior cruciate ligament injuries in athletes. Am J Sports Med. 1987;15:553–557. doi: 10.1177/036354658701500606. [DOI] [PubMed] [Google Scholar]
- 45.Geissler WB, Whipple TL. Intraarticular abnormalities in association with posterior cruciate ligament injuries. Am J Sports Ed. 1993;21:846–849. doi: 10.1177/036354659302100615. [DOI] [PubMed] [Google Scholar]
- 46.Hamada M, Shino K, Mitsuoka T, Toritsuka Y, Natsu-Ume T, Horibe S. Chondral injury associated with acute isolated posterior cruciate ligament injury. Arthroscopy. 2000;16:59–63. doi: 10.1016/s0749-8063(00)90128-2. [DOI] [PubMed] [Google Scholar]
- 47.Fanelli GC, Edson CJ. Posterior cruciate ligament injuries in trauma patients: Part II. Arthroscopy. 1995;11:526–529. doi: 10.1016/0749-8063(95)90127-2. [DOI] [PubMed] [Google Scholar]
- 48.Noyes FR, Simon R. The role of high tibial osteotomy in the anterior cruciate ligament-deficient knee with varus alignment. In: DeLee JC, Drez D, editors. Orthopaedic sports medicine. Philadelphia: Principles and Practice; 1994. pp. 1401–1443. [Google Scholar]
- 49.Brazier J, Migaud H, Gougeon F, Cotten A, Fontaine C, Duquennoy A. Evaluation of methods for radiographic measurement of the tibial slope. A study of 83 healthy knee. Rev Chir Orthop Reparatrice Appar Mot. 1996;82:195–200. [PubMed] [Google Scholar]
- 50.Lecuire F, Lerat JL, Bousquet G, Dejour H, Trillat A. The treatment of genu recurvatum. Rev Chir Orthop Reparatrice Appar Mot. 1980;66:95–103. [PubMed] [Google Scholar]
- 51.Insall JN. Total knee arthroplasty in rheumatoid arthritis. Ryumachi. 1993;33:472. [PubMed] [Google Scholar]
- 52.Paley D, Herzenberg JE, Tetsworth K, McKie J, Bhave A. Deformity planning for frontal and sagittal plane corrective osteotomies. Orthop Clin North Am. 1994;25:425–465. [PubMed] [Google Scholar]
- 53.Matsuda S, Miura H, Nagamine R, Urabe K, Ikenoue T, Okazaki K, Iwamoto Y. Posterior tibial slope in the normal and varus knee. Am J Knee Surg. 1999;12:165–168. [PubMed] [Google Scholar]
- 54.Chiu KY, Zhang SD, Zhang GH. Posterior slope of tibial plateau in Chinese. J Arthroplasty. 2000;15:224–227. doi: 10.1016/s0883-5403(00)90330-9. [DOI] [PubMed] [Google Scholar]
- 55.Genin P, Weill G, Julliard R. The tibial slope. Proposal for a measurement method. J Radiol. 1993;74:27–33. [PubMed] [Google Scholar]
- 56.Amendola A, Rorabeck CH, Bourne RB, Apyan PM. Total knee arthroplasty following high tibial osteotomy for osteoarthritis. J Arthroplasty. 1989;4(Suppl):S11–S17. doi: 10.1016/s0883-5403(89)80002-6. [DOI] [PubMed] [Google Scholar]
- 57.Levigne Ch, Bonnin M (1991) Osteotomie tibiale de valgisation pour arthrose femoro-tibale interne. In: 7e’mes journees lyonnaise de chirurgie di genu, Lyon, pp 142–168
- 58.Boileau P, Neyret PH (1991) Resultats des osteotomies tibialis de valgisation assoiees aux plasties du ligament croise’ anterieur dans le traitment des laxites anterieures chronique evoluees. In: 7emes journees lyonnaises de chirurgie du genu, Lyon, pp 232–249
- 59.Hohmann E, Bryant A, Imhoff AB. The effect of closed wedge high tibial osteotomy on tibial slope: a radiographic study. Knee Surg Sports Traumatol Arthrosc. 2006;14:454–459. doi: 10.1007/s00167-005-0700-3. [DOI] [PubMed] [Google Scholar]
- 60.Giffin JR, Stabile KJ, Zantop T, Vogrin TM, Woo SL, Harner CD. Importance of tibial slope for stability of the posterior cruciate ligament-deficient knee. Am J Sports Med. 2007;35:1443–1449. doi: 10.1177/0363546507304665. [DOI] [PubMed] [Google Scholar]
- 61.Rodner CM, Adams DJ, Diaz-Doran V, Tate JP, Santangelo SA, Mazzocca AD, Arciero RA. Medial opening wedge tibial osteotomy and the sagittal plane: the effect of increasing tibial slope on tibiofemoral contact pressure. Am J Sports Med. 2006;34:1431–1441. doi: 10.1177/0363546506287297. [DOI] [PubMed] [Google Scholar]
- 62.Marti CB, Gautier E, Wachtl SW, Jakob RP. Accuracy of frontal and sagittal plane correction in open-wedge high tibial osteotomy. Arthroscopy. 2004;20:366–372. doi: 10.1016/j.arthro.2004.01.024. [DOI] [PubMed] [Google Scholar]
- 63.Bonnin M (1990) La subluxation tibiale anterieure en appui monopodal dans les ruptures du ligament croise anterieur. Etude clinic et biomechanique (thesis). Université Claude Bernard, Lyon
- 64.Naudie DD, Amendola A, Fowler PJ. Opening wedge high tibial osteotomy for symptomatic hyperextension-varus thrust. Am J Sports Med. 1994;32:60–70. doi: 10.1177/0363546503258907. [DOI] [PubMed] [Google Scholar]
- 65.Giffin JR, Vogrin TM, Zantop T, Woo SL, Harner CD. Effects of increasing tibial slope on the biomechanics of the knee. Am J Sports Med. 2004;32:376–382. doi: 10.1177/0363546503258880. [DOI] [PubMed] [Google Scholar]
- 66.Nakamura E, Mizuta H, Kudo S, Takagi K, Sakamoto K. Open-wedge osteotomy of the proximal tibia hemicallotasis. J Bone Joint Surg Br. 2001;83:1111–1115. doi: 10.1302/0301-620x.83b8.11993. [DOI] [PubMed] [Google Scholar]
- 67.Maquet P. Valgus osteotomy for osteoarthritis of the knee. Clin Orthop Relat Res. 1976;120:143–148. [PubMed] [Google Scholar]
- 68.Viskontas DG, MacLeod MD, Sanders DW. High tibial osteotomy with use of the Taylor Spatial frame external fixator for osteoarthritis of the knee. Can J Surg. 2006;49:245–250. [PMC free article] [PubMed] [Google Scholar]
- 69.Ohsawa S, Hukuda K, Inamori Y, Yasui N. High tibial osteotomy for osteoarthritis of the knee with varus deformity utilizing the hemicallotasis method. Arch Orthop Trauma Surg. 2006;126:588–593. doi: 10.1007/s00402-006-0130-9. [DOI] [PubMed] [Google Scholar]
- 70.Klinger HM, Lorenz F, Harer T. Open wedge tibial osteotomy by hemicallotasis for medial compartment osteoarthritis. Arch Orthop Trauma Surg. 2001;121:245–247. doi: 10.1007/s004020000216. [DOI] [PubMed] [Google Scholar]
- 71.Cullù E, Aydogdu S, Alparslan B, Sur H. Tibial slope changes following dome-type high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2005;13:38–43. doi: 10.1007/s00167-004-0501-0. [DOI] [PubMed] [Google Scholar]
- 72.Agneskirchner JD, Hurschler C, Stukenborg-Colsman C, Imhoff AB, Lobenhoffer P. Effect of high tibial flexion osteotomy on cartilage pressure, joint kinematics: a biomechanical study in human cadaveric knees. Winner of the AGA-DonJoy Award 2004. Arch Orthop Trauma Surg. 2004;124:575–584. doi: 10.1007/s00402-004-0728-8. [DOI] [PubMed] [Google Scholar]
- 73.Petrigliano FA, McAllister DR. Isolated posterior cruciate ligament injuries of the knee. Sports Med Arthrosc Rev. 2006;14:206–212. doi: 10.1097/01.jsa.0000212325.23560.d2. [DOI] [PubMed] [Google Scholar]
- 74.LaPrade RF, Terry GC. Injuries to the posterolateral aspect of the knee: association of anatomic injury patterns with clinical instability. Am J Sports Med. 1997;25:433–438. doi: 10.1177/036354659702500403. [DOI] [PubMed] [Google Scholar]
- 75.Mayo Robson AW. Ruptured cruciate ligament and their repair by operation. Ann Surg Engl. 1903;37:716–718. [PMC free article] [PubMed] [Google Scholar]
- 76.Barton TM, Torg JS, Das M. Posterior cruciate ligament insufficiency. A review of the literature. Sports Med. 1984;1:419–430. doi: 10.2165/00007256-198401060-00002. [DOI] [PubMed] [Google Scholar]
- 77.Rubinstein RA, Jr, Shelbourne KD, McCarroll JR, VanMeter CD, Rettig AC. The accuracy of the clinical examination in the setting of posterior cruciate ligament injuries. Am J Sports Med. 1994;22:550–557. doi: 10.1177/036354659402200419. [DOI] [PubMed] [Google Scholar]
- 78.Strobel M, Stedtfeld HW, Feagia JA, Telger TC. Diagnostic evaluation of the knee. New York: Springer; 1990. [Google Scholar]
- 79.Paessler HH, Michel D. How new is the Lachman test? Am J Sports Med. 1992;20:95–98. doi: 10.1177/036354659202000122. [DOI] [PubMed] [Google Scholar]
- 80.Daniel DM, Stone ML, Barnett P, Sachs R. Use of the quadriceps active test to diagnose posterior cruciate-ligament disruption and measure posterior laxity of the knee. J Bone Joint Surg Am. 1988;70:386–391. [PubMed] [Google Scholar]
- 81.Loomer RL. A test for knee posterolateral rotatory instability. Clin Orthop Relat Res. 1991;264:235–238. [PubMed] [Google Scholar]
- 82.Veltri DM, Warren RF. Anatomy, biomechanics, and physical findings in posterolateral knee instability. Clin Sports Med. 1994;13:599–614. [PubMed] [Google Scholar]
- 83.Hughston JC, Norwood LA., Jr The posterolateral drawer test and external rotational recurvatum test for posterolateral rotatory instability of the knee. Clin Orthop Relat Res. 1980;147:82–87. [PubMed] [Google Scholar]
- 84.Palmer I. On injuries the ligaments of the knee joint. A clinical study. Acta Chir Scand Suppl. 1938;53:282. [Google Scholar]
- 85.Hughston JC, Andrews JR, Cross MJ, Moschi A. Classification of knee ligament instabilities: Part II. The lateral compartment. J Bone Joint Surg Am. 1976;58:173–179. [PubMed] [Google Scholar]
- 86.Hughston JC, Norwood LA., Jr The posterolateral drawer test and external rotational recurvatum test for posterolateral rotator instability of the knee. Clin Orthop Relat Res. 1980;136:82–87. [PubMed] [Google Scholar]
- 87.Jakob RP, Hassler H, Staubli HU. Observations on rotator instability of the lateral compartment of the knee. Experimental studies of the functional anatomy and pathomechanism of the true and reverse pivot shift sign. Acta Orthop Scand. 1981;52:1–32. doi: 10.3109/ort.1981.52.suppl-191.01. [DOI] [PubMed] [Google Scholar]
- 88.Cooper DE. Tests for posterolateral instability of the knee in normal subjects. J Bone Joint Surg Am. 1991;73:30–36. [PubMed] [Google Scholar]
- 89.Dugdale TW, Noyes FR, Styer D. Preoperative planning for high tibial osteotomy. The effect of lateral tibiofemoral separation and tibiofemoral length. Clin Orthop Relat Res. 1992;274:248–264. [PubMed] [Google Scholar]
- 90.Moreland JR, Bassett LW, Hanker GJ. Radiographic analysis of the axial alignment of the lower extremity. J Bone Joint Surg Am. 1987;69:745–749. [PubMed] [Google Scholar]
- 91.Moore TM, Harvey JP., Jr Roentgenographic measurement of tibial-plateau depression due to fracture. J Bone Joint Surg Am. 1974;56:155–160. [PubMed] [Google Scholar]
- 92.Merchant AC, Mercer RL, Jacobsen RH, Cool CR. Roentgenographic analysis of patellofemoral congruence. J Bone Joint Surg Am. 1974;56:1391–1396. [PubMed] [Google Scholar]
- 93.Rosenberg TD, Paulos LE, Parker RD, Coward DB, Scott SM. The forty-five-degree posteroanterior flexion weight-bearing radiograph of the knee. J Bone Joint Surg Am. 1988;70:1479–1483. [PubMed] [Google Scholar]
- 94.Jacobsen K. Stress radiographical measurement of the anteroposterior, medial and lateral stability of the knee joint. Acta Orthop Scand. 1976;47:334–335. doi: 10.3109/17453677608992002. [DOI] [PubMed] [Google Scholar]
- 95.Strobel MJ, Weiler A, Schulz MS, Russe K, Eichhorn HJ. Fixed posterior subluxation in posterior cruciate ligament-deficient knees: diagnosis and treatment of a new clinical sign. Am J Sports Med. 2002;30:32–38. doi: 10.1177/03635465020300011901. [DOI] [PubMed] [Google Scholar]
- 96.Louisia S, Siebold R, Canty J, Bartlett RJ. Assessment of posterior stability in total knee replacement by stress radiographs: prospective comparison of two different types of mobile bearing implants. Knee Surg Sports Traumatol Arthrosc. 2005;6:476–482. doi: 10.1007/s00167-004-0567-8. [DOI] [PubMed] [Google Scholar]
- 97.Chassaing VDF, Touzard R, et al. Etude radiologique du L.C.P’.a 90 de flexion. Rev Chir Orthop. 1995;81:35–38. [Google Scholar]
- 98.Jung TM, Reinhardt C, Scheffler SU, Weiler A. Stress radiography to measure posterior cruciate ligament insufficiency: a comparison of five different techniques. Knee Surg Sports Traumatol Arthrosc. 2006;14:1116–1121. doi: 10.1007/s00167-006-0137-3. [DOI] [PubMed] [Google Scholar]
- 99.Staubli HU, Jakob RP. Posterior instability of the knee extension. A clinical and stress radiographic analysis of acute injuries of the posterior cruciate ligament. J Bone Joint Surg Br. 1990;2:225–230. doi: 10.1302/0301-620X.72B2.2312560. [DOI] [PubMed] [Google Scholar]
- 100.Puddu G, Gianni E, Chambat P, De Paulis F. The axial view in evaluating tibial translation in cases of insufficiency of the posterior cruciate ligament. Arthroscopy. 2000;16:217–220. doi: 10.1016/s0749-8063(00)90040-9. [DOI] [PubMed] [Google Scholar]
- 101.Margheritini F, Mancini L, Mauro CS, Mariani PP. Stress radiography for quantifying posterior cruciate ligament deficiency. Arthroscopy. 2003;19:706–711. doi: 10.1016/s0749-8063(03)00399-2. [DOI] [PubMed] [Google Scholar]
- 102.Puddu G, Cipolla M, Cerullo G, Franco V, Gianni E. Osteotomies: the surgical treatment of the valgus knee. Sports Med Arthrosc. 2007;15:15–22. doi: 10.1097/JSA.0b013e3180305c76. [DOI] [PubMed] [Google Scholar]
- 103.Gross ML, Grover JS, Bassett LW, Seeger LL, Finerman GA. Magnetic resonance imaging of the posterior cruciate ligament. Clinical use to improve diagnostic accuracy. Am J Sports Med. 1992;20:732–737. doi: 10.1177/036354659202000615. [DOI] [PubMed] [Google Scholar]
- 104.Bellelli A, Mancini P, Polito M, David V, Mariani PP. Magnetic resonance imaging of posterior cruciate ligament injuries: a new classification of traumatic tears. Radiol Med (Torino) 2006;111:828–835. doi: 10.1007/s11547-006-0076-6. [DOI] [PubMed] [Google Scholar]
- 105.Yu JS, Salonen DC, Hodler J, Haghighi P, Trudell D, Resnick D. Posterolateral aspect of the knee: improved MR imaging with a coronal oblique technique. Radiology. 1996;198:199–204. doi: 10.1148/radiology.198.1.8539378. [DOI] [PubMed] [Google Scholar]
- 106.LaPrade RF, Gilbert TJ, Bollom TS, Wentorf F, Chaljub G. The magnetic resonance imaging appearance of individual structures of the posterolateral knee. A prospective study of normal knees and knees with surgically verified grade III injuries. Am J Sports Med. 2000;28:191–199. doi: 10.1177/03635465000280020901. [DOI] [PubMed] [Google Scholar]
- 107.Akizuki S, Shibakawa A, Takizawa T, Yamazaki I, Horiuchi H. The long-term outcome of high tibial osteotomy: a 10–20 year follow-up. J Bone Joint Surg Br. 2008;90:592–596. doi: 10.1302/0301-620X.90B5.20386. [DOI] [PubMed] [Google Scholar]
- 108.Catagni MA, Guerreschi F, Ahmad TS, Cattaneo R. Treatment of genu varum in medial compartment osteoarthritis of the knee using the Ilizarov method. Orthop Clin North Am. 1994;25:509–514. [PubMed] [Google Scholar]
- 109.Watanabe K, Tsuchiya H, Matsubara H, Kitano S, Tomita K. Revision high tibial osteotomy with the Taylor spatial frame for failed opening-wedge high tibial osteotomy. J Orthop Sci. 2008;13:145–149. doi: 10.1007/s00776-007-1200-8. [DOI] [PubMed] [Google Scholar]
- 110.Kibler WB, Press J, Sciascia A. The role of core stability in athletic function. Sports Med. 2006;36:189–198. doi: 10.2165/00007256-200636030-00001. [DOI] [PubMed] [Google Scholar]