

SYNOPSIS
Objectives
On September 11, 2001 (9/11), attacks on the World Trade Center (WTC) killed 341 Fire Department of the City of New York (FDNY) firefighters and injured hundreds more. Previous WTC-related studies reported high rates of comorbid depression and posttraumatic stress disorder (PTSD), identifying disability retirement, alcohol use, and early arrival at the WTC site as correlates. However, those studies did not evaluate risk factors that could have mediated the observed comorbidity. We identified unique risk factors for each condition in an effort to better understand comorbidity.
Methods
We screened retired WTC-exposed firefighters using self-administered questionnaires including the Center for Epidemiologic Studies Depression Scale, the Post Traumatic Stress Disorder Checklist, and the Alcohol Use Disorders Identification Test. We performed regression analyses to compare independent predictors of elevated depression and PTSD risk, and also tested a mediation hypothesis.
Results
From December 2005 to July 2007, 23% and 22% of 1,915 retirees screened positive for elevated depression and PTSD risk, respectively, with comorbidity >70%. Controlling for comorbidity, we identified unique risk factors for (1) depression: problem alcohol use and (2) PTSD: early arrival at the WTC site.
Conclusions
Our data support the premise that PTSD and depression are different responses to trauma with unique risk factors. The data also suggest a hypothesis that PTSD mediates the relationship between early WTC arrival and depression, while depression mediates the relationship between alcohol use and PTSD, a more complex relationship than shown in previous studies. Clinicians should consider these factors when evaluating patients for depression and PTSD.
The September 11, 2001 (9/11), attacks on the World Trade Center (WTC) towers exposed rescue and recovery workers to great physical and psychological harm, resulting in high rates of posttraumatic stress disorder (PTSD), depression, and especially high rates of these disorders concurrently.1–6 During 2002–2003, a Veterans Affairs health-care study found that more than one-third of primary care patients with depressive symptoms had comorbid PTSD.3,4 During 2005–2006, more than half of urban, health-care-seeking women5 with PTSD reported comorbid depression and, in 1995, 55% of survivors of the Oklahoma City bombing1 with PTSD reported comorbid depression. In 2001, a study of Manhattan residents living near Ground Zero at the time of the WTC attacks found that roughly half of those reporting symptoms of PTSD also reported symptoms of depression two to three months after 9/11.2
Alternative explanations for the observed comorbidity include: (1) both conditions are reactions to traumatic events,7 (2) depression is a reaction to severe or prolonged PTSD,8 and (3) symptom overlap between these conditions accounts for the appearance of their co-occurrence.9 Studies have not agreed on whether depression and PTSD are separate constructs or part of a single construct postexposure to trauma.10,11
Previous studies of Fire Department of the City of New York (FDNY) retirees have identified WTC exposure, retirement with a disability pension, and alcohol abuse as risk factors that appeared to be common to both morbidities in multivariable regressions.12,13 However, these models did not control for occurrences of PTSD as a comorbid condition when examining depression, and vice versa. We reexamined these identified risk factors for each disorder (depression and PTSD) controlling for the presence of the other condition in an attempt to clarify whether depression and PTSD represent separate constructs or a single reaction to a traumatic event.
METHODS
Since 1997, the FDNY Bureau of Health Services (BHS) has performed periodic health evaluations on active FDNY members approximately every 18 months, which include both physician examinations and, since 2001, self-administered health questionnaires. In 2005, a more extensive mental health questionnaire incorporated validated instruments, including the Center for Epidemiologic Studies Depression (CES-D) Scale, the PTSD Checklist (PCL-17), and the Alcohol Use Disorders Identification Test (AUDIT). This inclusion occurred simultaneously with outreach to retired WTC-exposed firefighters, who were invited to resume participation in health evaluations. These screenings had been previously limited to the active workforce. Participation in the study required written informed consent and was approved by the Institutional Review Board of Montefiore Medical Center.
Participants
In 2005, expanded mental and physical health screening extended the length of the WTC Medical Monitoring and Treatment Program (MMTP) visit. This expansion was first introduced for retired members in an effort to assess the additional time required for scheduling the active workforce. Thus, this study was limited to retirees who completed the expanded screening and worked at least one shift at any of the designated WTC work sites between September 11, 2001, and July 25, 2002, when the sites were formally closed.
A total of 4,080 retiree candidates were eligible. Recruitment involved contacting retirees through invitational letters and/or by telephone using contact information from the FDNY pension database. Self-enrollment was also possible through the FDNY website. We used data from the first 19 months of the expanded monitoring for the current analysis (December 2005 to July 2007). By the end of the initial enrollment period, 2,574 retired firefighters (63% of those eligible) had returned to FDNY BHS and completed a monitoring exam.
We excluded the following: people who could not be classified in a 9/11 exposure group or first arrived at any of the WTC sites after September 24, 2001 (n=316); those who did not complete all parts of the monitoring visit on the same day (n=218); fire marshals (n=84) due to the distinct nature of their work; people who retired due to a mental health disability (n=31); and females (n=10), because they represent a small proportion of the workforce. The final analytic sample totaled 1,915 (47% of those eligible). We compared characteristics of the final analytic sample with WTC-exposed retirees who did not participate.
Data sources
We obtained age, hire date, retirement date and status (ordinary vs. disability retirement), and rank (e.g., chiefs, captains, lieutenants, and firefighters) from the FDNY employee database. We collected all other variables from the questionnaires.
9/11 exposure
The FDNY-WTC Exposure Intensity Index14 categorized exposure based on first arrival at the WTC site as follows: “Group 1,” the most severely exposed, arriving on the morning of 9/11 and present during the towers' collapse; “Group 2,” arriving during the afternoon of 9/11; “Group 3,” arriving the next day on September 12, 2001; and “Group 4,” or least exposed, arriving any day between days three and 14.
Measures
The 20-item CES-D assesses depressive symptoms; each symptom is scored on a scale of 0 to 3 (0 = none or rarely [less than one day per week], 3 = most or all of the time [five to seven days per week]), with four of the items worded in the positive direction.15 The FDNY version refers to symptom presence in the past month.12
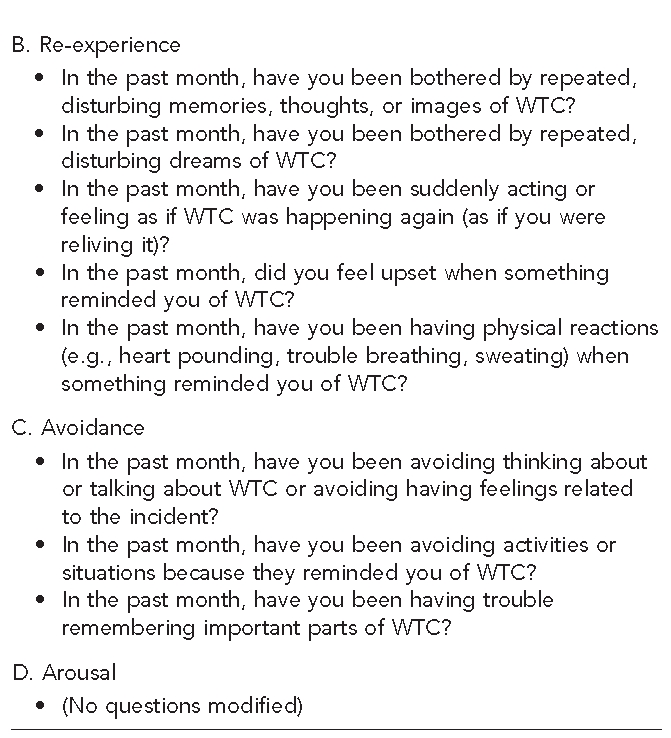
The PCL was designed using 17 items that correspond to the Diagnostic and Statistical Manual of Mental Disorders symptoms of PTSD.16 Using a Likert scale of 1 to 5 (1 = not at all, 5 = extremely), total scores can range from 17 to 85. We modified the PCL in our questionnaire to fit the context of 9/11. For example, we modified questions that referred specifically to a traumatic event to refer to the event as “WTC;” however, the wording of symptoms themselves remained unchanged. Each question was also specific to symptoms in the past month (Figure 1).
Figure 1.
PTSD checklist questions modified to fit context of WTC
Note: Answer choices for all questions were: 1 = not at all, 2 = a little bit, 3 = moderately, 4 = quite a bit, and 5 = extremely.
PTSD = posttraumatic stress disorder
WTC = World Trade Center
Because the CES-D and the PCL cannot determine psychiatric diagnosis, outcomes as determined by cutoff scores on these questionnaires were labeled “elevated depression risk” and “elevated PTSD risk.” Elevated depression and PTSD risk were denoted using cutoff scores of ≥22 and ≥39 on these instruments, respectively, which were previously validated in this population.12,13
We assessed alcohol use disorder using AUDIT, a screening instrument developed by the World Health Organization to detect excessive drinking.17,18 Using 10 items that correspond to International Classification of Diseases, 10th Revision definitions of alcohol dependence and abuse, total scores can range from 0 to 40. We used cutoff scores ≥8 as indicators of harmful use.19
Disability retirement refers to a member retiring with a service-related disability for any physical ailment (e.g., respiratory, musculoskeletal, cardiac, or cancer).
Data analysis
We analyzed demographic and other variables in relation to elevated depression and PTSD risk. Bivariate analyses of categorical variables used Chi-square tests with odds ratios (ORs) and 95% confidence intervals (CIs) or McNemar's test, as appropriate. We measured the correlation between two continuous variables using Pearson's r. We performed logistic regression analyses to identify independent predictors of (1) elevated depression risk and (2) elevated PTSD risk. Initially, we entered all variables that showed statistically significant associations in bivariate analyses into the multivariate model. We removed the four variables whose p-values were >0.05. Analyses were performed using SAS® version 9.1.3.20
We used the modeling method proposed by Baron and Kenny to assess a mediation hypothesis, defined as testing that “a given variable [may] … function as a mediator [or confounder] to the extent that it accounts for the relation between the predictor and the criterion” or outcome.21
RESULTS
Characteristics of the study population
The 1,915 retired male firefighters averaged 47.0 years of age on 9/11 (standard deviation = 6.9; range: 28.0–73.4). On 9/11, 83% were married; 8% were separated, divorced, or widowed; 6% were single; and 3% were living with a partner. Nearly all were Caucasian (95%); approximately 64% had retired with a disability pension. Most participants arrived at the WTC site on 9/11 (72%), with the majority arriving after the collapse of the WTC towers, during the afternoon of 9/11 (56%). By the end of day two, more than 88% reported working at the WTC site. Approximately 40% worked at the WTC site for five or more months. About 78% reported the WTC collapse was the most emotionally terrible, frightening, or horrible event they had ever experienced.
We compared characteristics of the 1,915 participants with 2,127 nonparticipating retirees who met the study criteria for inclusion. The primary difference between participants and nonparticipants was that the former were more likely to live in the tristate area (New York, New Jersey, and Connecticut) (p<0.01). Participants were also, on average, older (47.0 vs. 45.4 years, p<0.01) and more likely to have retired as chiefs (6% vs. 4%, p<0.01). The groups were similar in the proportion of members who were present during the morning of the WTC collapse (16% vs. 17%, p=0.21) and in those retiring with disability benefits (65% vs. 64%, p=0.81).
Rates of elevated PTSD and depression risk
We identified elevated depression and PTSD risk in 23% and 22% of this sample, respectively, with the majority of cases occurring comorbidly (Figure 2). Of all individuals with elevated depression risk (n=434), 71% were also identified with elevated PTSD risk. Conversely, of all individuals with elevated PTSD risk (n=422), 73% were also identified with elevated depression risk. CES-D (depression) scores were strongly correlated with PCL (PTSD) scores (r=0.83, p<0.01). About 80% of those with elevated PTSD risk reported the WTC collapse was their most emotionally terrible, frightening, or horrible lifetime event. Table 1 shows adjusted and unadjusted ORs for the association between selected characteristics and both elevated PTSD and depression risk.
Figure 2.
Prevalence of elevated PTSD risk (22.0%) and elevated depression risk (22.7%) in 9/11-exposed retired firefighters (n=1,915)a
Note: Venn Diagram not to scale
aPercentages do not add up to 100% due to rounding.
PTSD = posttraumatic stress disorder
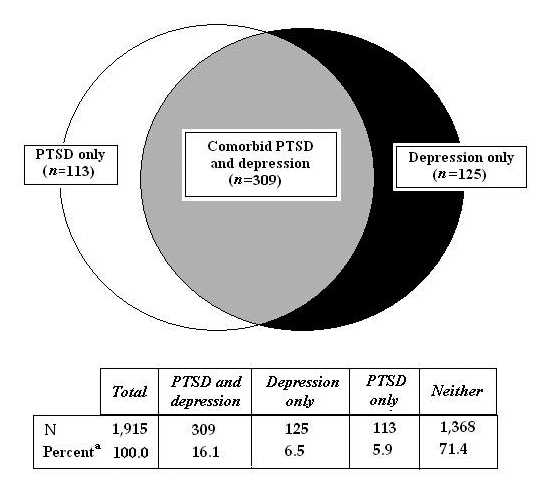
Table 1.
Bivariate and multivariable analyses for prevalence of current (30-day) depression and PTSD in 9/11-exposed firefighters, by selected characteristics

aThese bivariate models satisfy conditions 1 and 2 if the variable is significantly associated with depression/PTSD (95% CI is in the range of significance).
bAdjusted for variables remaining significant in model: age group on 9/11, exposure group, retirement status, and AUDIT scores.
PTSD = posttraumatic stress disorder
OR = odds ratio
CI = confidence interval
Ref. = referent group
AUDIT = Alcohol Use Disorders Identification Test
NA = not applicable
Testing for mediation
Following the Baron and Kenny steps, results from unadjusted logistic regression models demonstrated strong statistically significant associations between exposure groups and elevated depression risk. Those who initially arrived at the WTC site earlier were more likely to be identified with elevated depression risk than those who arrived on a later day (OR range: 1.6–3.5). After adjusting for elevated PTSD risk, the magnitude of the associations with exposure groups was substantially reduced (OR range: 1.2–1.6) and was no longer statistically significant (Table 2). The association between elevated depression and PTSD risk, however, remained statistically significant (p<0.01). When elevated PTSD risk was replaced as the dependent variable and elevated depression risk as the new potential mediator, the magnitude of association between elevated depression risk and exposure groups 1 and 2 remained similar, and statistically significant (p<0.01).
Table 2.
Comorbidity adjusted odds ratios for prevalence of current (30-day) depression and PTSD in 9/11-exposed firefighters, by selected characteristics

Note: If PTSD did not mediate the relationship between exposure and depression, the ORs for depression by exposure would not be expected to substantially change after adjustment for PTSD. Similarly, if depression did not mediate the relationship between alcohol use disorders and PTSD, the association between alcohol use disorders and PTSD would not be expected to substantially change after adjustment for depression.
PTSD = posttraumatic stress disorder
OR = odds ratio
AOR = adjusted odds ratio
CI = confidence interval
Ref. = referent group
AUDIT = Alcohol Use Disorders Identification Test
Similarly, while unadjusted alcohol use disorder was associated with PTSD risk (OR=2.0), when adjusted for elevated depression risk, the association was no longer observed (OR=1.1). In the adjusted model, elevated depression risk was significantly associated with PTSD risk (p<0.01). Alcohol use disorder remained statistically significant with a similar OR when elevated depression risk was replaced as the dependent variable, adjusting for elevated PTSD risk (Table 2).
Additional models of elevated depression and PTSD risk, including exposure group, alcohol abuse, and disability retirement, can be found in Tables 1 and 2. Multivariable models adjusting for the alternate comorbid outcome demonstrated that exposure status was a unique risk factor for elevated PTSD risk, and alcohol use disorder was a unique risk factor for elevated depression risk. Disability retirement was a risk factor for both elevated PTSD risk and elevated depression risk, even when controlling for comorbidity.
DISCUSSION
In this study of retired WTC-exposed firefighters, we found high rates of PTSD and depression risk and high comorbidity. While we cannot rule out potential confounding factors from other traumatic events, 80% of those with elevated PTSD risk reported the WTC collapse was the most emotionally terrible event of their lifetime. Other studies have shown WTC exposure to be associated with increased rates of depression or PTSD,22–26 but this is the first report of such high prevalence rates occurring comorbidly in 9/11 first responders. In fact, four to six years after 9/11, these rates were as high as those reported in Vietnam veterans,27 clearly supporting continued monitoring and treatment for trauma-induced mental health consequences in this population.
Screening instruments validated separately for depression and PTSD share some similar symptom questions and, therefore, it has been suggested that the presence of one condition raises the risk for the other due to symptom question overlap rather than true comorbidity between these conditions.9 Yet, the investigator is faced with the fact that these validated questionnaires are widely used, cannot easily be changed, and that distinct differences in overall symptom profile are widely acknowledged and used by clinicians to identify each disease separately or comorbidly. Shared vulnerabilities were noticed in earlier WTC studies2,7,12,13 and in other non-WTC studies,28 but those analyses did not evaluate risk factors that might have mediated comorbidity in an effort to identify unique correlates for each condition.
To further understand the relationship between 9/11 trauma and mental health risk in retired FDNY firefighters, we analyzed correlations between selected characteristics and elevated depression and PTSD risk. As shown in previous studies,12,13 multivariable logistic regression models not controlling for comorbidity (Table 2) identified WTC exposure, retirement with a disability pension, and alcohol use disorder as associated with current elevated depression and PTSD risk. We then explored mediation analyses using these variables as characteristics of interest using two methods: (1) a series of logistic regressions controlling for the variable suspected of having a confounder role and (2) logistic regressions on the population stratified by mental health status.
Regression analyses in this study demonstrated increased elevated depression and PTSD risk with earlier WTC arrival time, but elevated PTSD risk mediated the relationship between elevated depression risk and WTC-exposure group when either of the aforementioned methods was applied. Although we did not find a dose-response gradient between WTC exposure and elevated depression risk, we noted that the prevalence of elevated depression risk (22.7%) was much higher in WTC-exposed retired FDNY firefighters than in other WTC-exposed populations (range: 9.7%–16.1%),2,22,29 a sample of older white Brooklyn residents (10%),30 and in the 12-month prevalence of a national sample of men (4%) and men ≥60 years of age (2.1%).31
Alcohol abuse has been previously identified as associated with increased risk of depression.32 The association between alcohol abuse and PTSD, however, is not as well understood, with studies presenting different interpretations.33,34 Our study found alcohol abuse to be associated with both elevated depression and PTSD risk. The association between alcohol abuse and elevated PTSD risk, however, was no longer statistically significant after adjusting for elevated depression risk. This finding is consistent with the hypothesis that the association between alcohol use and elevated PTSD risk was mediated by elevated depression risk.
Elevated risk for PTSD and depression was also associated with disability retirement for physical injuries or illnesses in multivariable models, supporting previous research finding associations among PTSD, depression, and a range of physical ailments.35 With a large proportion of our sample having retired with disability, this may also explain, in part, the higher rates of elevated depression risk when compared with national samples, with presumably far lower rates of disability. Extensive examination of the effect of disability retirement was beyond the scope of this study, but warrants future investigation.
Consistent with Blanchard et al., our models suggest that elevated depression and PTSD risk may be separate constructs.10 After controlling for comorbidity in the current study, we identified unique correlates for each condition, which support the premise that depression and PTSD are independent responses to trauma.
Limitations
Our findings add to the growing understanding of traumatic events, but our study had several limitations. First, we did not specifically account for exposure to traumatic events unrelated to 9/11, occurring before 9/11, or occurring between 9/11 and the date of the health evaluation. This factor was partially addressed by modifying the PCL so that subject answers to questions were clearly in the context of 9/11. We also examined each member's most stressful lifetime event (with 78% of the cohort and 80% of those with elevated PTSD risk identifying the WTC collapse). Despite these efforts, it is possible that other lifetime events could impact PTSD development, regardless of whether these events were identified as the “most stressful.”
A second limitation was the cross-sectional study design, which prevented drawing conclusions about the direction of potential mediation and also prevented differentiation between chronic and delayed-onset morbidity.36 Third, screening questionnaires are not clinical diagnoses, which is why we used the qualifier “elevated risk” to describe depression and PTSD prevalence based on our questionnaire results. Previous studies, however, have shown the CES-D and the PCL to have good correspondence with clinical diagnoses.37–43 Finally, the generalizability of these results is limited to retired WTC-exposed male firefighters until further studies can be performed on other trauma-exposed populations.
CONCLUSIONS
Our findings have important clinical implications. First, they support previous reports of high levels of comorbid depression and PTSD in trauma-exposed populations. Our analyses extend these observations by supporting the premise that depression and PTSD are distinct responses to trauma. Past studies identified alcohol abuse as being associated with PTSD,33–35 whereas our data suggest that alcohol abuse may result from mediation through depression. Similarly, past studies identified WTC arrival time as associated with depression, but our data indicate that this association may derive from mediation through PTSD. Awareness of risk factors for both elevated depression and PTSD risk, such as physical injury severe enough to result in disability retirement, allows for earlier detection and earlier opportunities for intervention.
For those with depression and PTSD, interventions need to be carefully designed, promoted, and monitored, as previous studies have associated comorbidity with greater psychiatric impairment, greater likelihood of hospital discharge against medical advice,44 lower health satisfaction,45 greater risk for somatization symptoms,46 and delayed response to intervention.45 Treatment regimens may also be different, with far less evidence supporting the use of medication in the absence of depression.47 Due to the important impact that comorbidity has on diagnosis and treatment, our findings of extensive comorbidity suggest that it may be prudent for clinicians to consider these factors and screen for both depression and PTSD.
Footnotes
This work was supported by the National Institute for Occupational Safety and Health RO1-OH07350. The authors are grateful to Carmen Nunez, Michelle Reddan, Rebecca Sagendorf, Malachy Corrigan, and the entire Fire Department of the City of New York Bureau of Health Services staff for their contributions to this project.
REFERENCES
- 1.North CS, Nixon SJ, Shariat S, Mallonee S, McMillen JC, Spitznagel EL, et al. Psychiatric disorders among survivors of the Oklahoma City bombing. JAMA. 1999;282:755–62. doi: 10.1001/jama.282.8.755. [DOI] [PubMed] [Google Scholar]
- 2.Galea S, Ahern J, Resnick H, Killpatrick D, Bucuvalas M, Gold J, et al. Psychological sequelae of the September 11 terrorist attacks in New York City. N Engl J Med. 2002;346:982–7. doi: 10.1056/NEJMsa013404. [DOI] [PubMed] [Google Scholar]
- 3.Campbell DG, Felker BL, Liu CF, Yaneo EM, Kirchner JE, Chan D, et al. Prevalence of depression-PTSD comorbidity: implications for clinical practice guidelines and primary care-based interventions. J Gen Intern Med. 2007;22:711–8. doi: 10.1007/s11606-006-0101-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gerrity MS, Corson K, Dobscha SK. Screening for posttraumatic stress disorder in VA primary care patients with depression symptoms. J Gen Intern Med. 2007;22:1321–4. doi: 10.1007/s11606-007-0290-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gill JM, Page GG, Sharps P, Campbell JC. Experiences of traumatic events and associations with PTSD and depression development in urban health care-seeking women. J Urban Health. 2008;85:693–706. doi: 10.1007/s11524-008-9290-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Salcioglu E, Basoglu M, Livanou M. Post-traumatic stress disorder and comorbid depression among survivors of the 1999 earthquake in Turkey. Disasters. 2007;31:115–29. doi: 10.1111/j.1467-7717.2007.01000.x. [DOI] [PubMed] [Google Scholar]
- 7.Fullerton CS, Ursano RJ, Wang L. Acute stress disorder, posttraumatic stress disorder, and depression in disaster or rescue workers. Am J Psychiatry. 2004;161:1370–6. doi: 10.1176/appi.ajp.161.8.1370. [DOI] [PubMed] [Google Scholar]
- 8.Ginzburg K, Ein-Dor T, Solomon Z. Comorbidity of posttraumatic stress disorder, anxiety and depression: a 20-year longitudinal study of war veterans. J Affect Disord. 2010;123:249–57. doi: 10.1016/j.jad.2009.08.006. [DOI] [PubMed] [Google Scholar]
- 9.Franklin CL, Zimmerman M. Posttraumatic stress disorder and major depressive disorder: investigating the role of overlapping symptoms in diagnostic comorbidity. J Nerv Ment Dis. 2001;189:548–51. doi: 10.1097/00005053-200108000-00008. [DOI] [PubMed] [Google Scholar]
- 10.Blanchard EB, Buckley TC, Hickling EJ, Taylor AE. Posttraumatic stress disorder and comorbid major depression: is the correlation an illusion? J Anxiety Disord. 1998;12:21–37. doi: 10.1016/s0887-6185(97)00047-9. [DOI] [PubMed] [Google Scholar]
- 11.O'Donnell ML, Creamer M, Pattison P. Posttraumatic stress disorder and depression following trauma: understanding comorbidity. Am J Psychiatry. 2004;161:1390–6. doi: 10.1176/appi.ajp.161.8.1390. [DOI] [PubMed] [Google Scholar]
- 12.Chiu S, Webber MP, Zeig-Owens R, Gustave J, Lee R, Kelly RJ, et al. Validation of the Center for Epidemiologic Studies Depression Scale in screening for major depressive disorder among retired firefighters exposed to the World Trade Center disaster. J Affect Disord. 2010;121:212–9. doi: 10.1016/j.jad.2009.05.028. [DOI] [PubMed] [Google Scholar]
- Chiu S, Webber MP, Zeig-Owens R, Niles J, Gustave J, Lee R, et al. Performance characteristics of the Posttraumatic Stress Disorder Checklist in retired firefighters exposed to the World Trade Center disaster. Ann Clin Psychiatry. In press 2011. [PubMed] [Google Scholar]
- 14.Prezant DJ, Weiden M, Banauch GI, McGuinness G, Rom WN, Aldrich TK, et al. Cough and bronchial responsiveness in firefighters at the World Trade Center site. N Engl J Med. 2002;347:806–15. doi: 10.1056/NEJMoa021300. [DOI] [PubMed] [Google Scholar]
- 15.Radloff LS. The CES-D Scale: a self-report depression scale for research in the general population. Appl Psych Meas. 1977;1:385–401. [Google Scholar]
- 16.Weathers FW, Litz BT, Herman DS, Huska JA, Keane TM. The PTSD Checklist (PCL): reliability, validity, and diagnostic utility; Paper presented at the Annual Meeting of the International Society for Traumatic Stress Studies; 1993 Oct 24–27; San Antonio, Texas. [Google Scholar]
- 17.Saunders JB, Aasland OG, Babor TF, de la Fuente JR, Grant M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption—II. Addiction. 1993;88:791–804. doi: 10.1111/j.1360-0443.1993.tb02093.x. [DOI] [PubMed] [Google Scholar]
- 18.Saunders JB, Aasland OG, Amundsen A, Grant M. Alcohol consumption and related problems among primary health care patients: WHO collaborative project on early detection of persons with harmful alcohol consumption—I. Addiction. 1993;88:349–62. doi: 10.1111/j.1360-0443.1993.tb00822.x. [DOI] [PubMed] [Google Scholar]
- 19.Babor TF, Higgins-Biddle JC, Saunders JB, Monteiro MG, editors. AUDIT—the Alcohol Use Disorders Identification Test: guidelines for use in primary health care. 2nd ed. Geneva: Department of Mental Health and Substance Dependence, World Health Organization; 2001. [Google Scholar]
- 20.SAS Institute, Inc. SAS®: Version 9.1.3 for Windows. Cary (NC): SAS Institute, Inc.; 2009. [Google Scholar]
- 21.Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51:1173–82. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- 22.Stellman JM, Smith RP, Katz CL, Sharma V, Charney DS, Herbert R, et al. Enduring mental health morbidity and social function impairment in World Trade Center rescue, recovery, and cleanup workers: the psychological dimension of an environmental health disaster. Environ Health Perspect. 2008;116:1248–53. doi: 10.1289/ehp.11164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Tapp LC, Baron S, Bernard B, Driscoll R, Mueller C, Wallingford K. Physical and mental health symptoms among NYC transit workers seven and one-half months after the WTC attacks. Am J Ind Med. 2005;47:475–83. doi: 10.1002/ajim.20177. [DOI] [PubMed] [Google Scholar]
- 24.Agronick G, Stueve A, Vargo S, O'Donnell L. New York City young adults' psychological reactions to 9/11: findings from the Reach for Health longitudinal study. Am J Community Psychol. 2007;39:79–90. doi: 10.1007/s10464-007-9093-4. [DOI] [PubMed] [Google Scholar]
- 25.Chemtob CM, Nomura Y, Abramovitz RA. Impact of conjoined exposure to the World Trade Center attacks and to other traumatic events on the behavioral problems of preschool children. Arch Pediatr Adolesc Med. 2008;162:126–33. doi: 10.1001/archpediatrics.2007.36. [DOI] [PubMed] [Google Scholar]
- 26.Perrin MA, DiGrande L, Wheeler K, Thorpe L, Farfel M, Brackbill R. Differences in PTSD prevalence and associated risk factors among World Trade Center disaster rescue and recovery workers. Am J Psychiatry. 2007;164:1385–94. doi: 10.1176/appi.ajp.2007.06101645. [DOI] [PubMed] [Google Scholar]
- 27.Beckham JC, Moore SD, Feldman ME, Hertzberg MA, Kirby AC, Fairbank JA. Health status, somatization, and severity of posttraumatic stress disorder in Vietnam combat veterans with posttraumatic stress disorder. Am J Psychiatry. 1998;155:1565–9. doi: 10.1176/ajp.155.11.1565. [DOI] [PubMed] [Google Scholar]
- 28.Chen YS, Chen MC, Chou FH, Sun FC, Chen PC, Tsai KY, et al. The relationship between quality of life and posttraumatic stress disorder or major depression for firefighters in Kaohsiung, Taiwan. Qual Life Res. 2007;16:1289–97. doi: 10.1007/s11136-007-9248-7. [DOI] [PubMed] [Google Scholar]
- 29.Gross R, Neria Y, Tao XG, Massa J, Ashwell L, Davis K, et al. Posttraumatic stress disorder and other psychological sequelae among World Trade Center clean up and recovery workers. Ann N Y Acad Sci. 2006;1071:495–9. doi: 10.1196/annals.1364.051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Cohen CI, Goh KH, Yaffee RA. Depression outcome among a biracial sample of depressed urban elders. Am J Geriatr Psychiatry. 2009;17:943–52. doi: 10.1097/JGP.0b013e3181b970c7. [DOI] [PubMed] [Google Scholar]
- 31.Kessler RC, Akiskal HS, Ames M, Birnbaum H, Greenberg P, Hirschfeld RM, et al. Prevalence and effects of mood disorders on work performance in a nationally representative sample of U.S. workers. Am J Psychiatry. 2006;163:1561–8. doi: 10.1176/appi.ajp.163.9.1561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Abraham HD, Fava M. Order of onset of substance abuse and depression in a sample of depressed outpatients. Compr Psychiatry. 1999;40:44–50. doi: 10.1016/s0010-440x(99)90076-7. [DOI] [PubMed] [Google Scholar]
- 33.Shipherd JC, Stafford J, Tanner LR. Predicting alcohol and drug abuse in Persian Gulf War veterans: what role do PTSD symptoms play? Addict Behav. 2005;30:595–9. doi: 10.1016/j.addbeh.2004.07.004. [DOI] [PubMed] [Google Scholar]
- 34.Hien DA, Jiang H, Campbell AN, Hu MC, Miele GM, Cohen LR, et al. Do treatment improvements in PTSD severity affect substance use outcomes? A secondary analysis from a randomized clinical trial in NIDA's Clinical Trials Network. Am J Psychiatry. 2010;167:95–101. doi: 10.1176/appi.ajp.2009.09091261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.O'Toole BI, Catts SV. Trauma, PTSD, and physical health: an epidemiological study of Australian Vietnam veterans. J Psychosom Res. 2008;64:33–40. doi: 10.1016/j.jpsychores.2007.07.006. [DOI] [PubMed] [Google Scholar]
- 36.Ginzburg K, Ein-Dor T, Solomon Z. Comorbidity of posttraumatic stress disorder, anxiety and depression: a 20-year longitudinal study of war veterans. J Affect Disord. 2010;123:249–57. doi: 10.1016/j.jad.2009.08.006. [DOI] [PubMed] [Google Scholar]
- 37.Cook JM, Elhai JD, Arean PA. Psychometric properties of the PTSD Checklist with older primary care patients. J Trauma Stress. 2005;18:371–6. doi: 10.1002/jts.20038. [DOI] [PubMed] [Google Scholar]
- 38.Cuijpers P, Boluijt P, van Straten A. Screening of depression in adolescents through the Internet: sensitivity and specificity of two screening questionnaires. Eur Child Adolesc Psychiatry. 2008;17:32–8. doi: 10.1007/s00787-007-0631-2. [DOI] [PubMed] [Google Scholar]
- 39.Forbes D, Creamer M, Biddle D. The validity of the PTSD checklist as a measure of symptomatic change in combat-related PTSD. Behav Res Ther. 2001;39:977–86. doi: 10.1016/s0005-7967(00)00084-x. [DOI] [PubMed] [Google Scholar]
- 40.Haringsma R, Engels GI, Beekman AT, Spinhoven P. The criterion validity of the Center for Epidemiological Studies Depression Scale (CES-D) in a sample of self-referred elders with depressive symptomatology. Int J Geriatr Psychiatry. 2004;19:558–63. doi: 10.1002/gps.1130. [DOI] [PubMed] [Google Scholar]
- 41.Wada K, Tanaka K, Theriault G, Satoh T, Mimura M, Miyaoka H, et al. Validity of the Center for Epidemiologic Studies Depression Scale as a screening instrument of major depressive disorder among Japanese workers. Am J Ind Med. 2007;50:8–12. doi: 10.1002/ajim.20403. [DOI] [PubMed] [Google Scholar]
- 42.Watson LC, Lewis CL, Kistler CE, Amick HR, Boustani M. Can we trust depression screening instruments in healthy ‘old-old’ adults? Int J Geriatr Psychiatry. 2004;19:278–85. doi: 10.1002/gps.1082. [DOI] [PubMed] [Google Scholar]
- 43.Yeager DE, Magruder KM, Knapp RG, Nicholas JS, Frueh BC. Performance characteristics of the posttraumatic stress disorder checklist and SPAN in Veterans Affairs primary care settings. Gen Hosp Psychiatry. 2007;29:294–301. doi: 10.1016/j.genhosppsych.2007.03.004. [DOI] [PubMed] [Google Scholar]
- 44.Holtzheimer PE, III, Russo J, Zatzick D, Bundy C, Roy-Byrne PP. The impact of comorbid posttraumatic stress disorder on short-term clinical outcome in hospitalized patients with depression. Am J Psychiatry. 2005;162:970–6. doi: 10.1176/appi.ajp.162.5.970. [DOI] [PubMed] [Google Scholar]
- 45.Rauch SA, Favorite T, Giardino N, Porcari C, Defever E, Liberzon I. Relationship between anxiety, depression, and health satisfaction among veterans with PTSD. J Affect Disord. 2010;121:165–8. doi: 10.1016/j.jad.2009.05.026. [DOI] [PubMed] [Google Scholar]
- 46.Andreski P, Chilcoat H, Breslau N. Post-traumatic stress disorder and somatization symptoms: a prospective study. Psychiatry Res. 1998;79:131–8. doi: 10.1016/s0165-1781(98)00026-2. [DOI] [PubMed] [Google Scholar]
- 47.Institute of Medicine. Treatment of PTSD: an assessment of the evidence. Washington: National Academies Press; 2007. [Google Scholar]