

Abstract
The 48,XXYY syndrome is a form of sex chromosome aneuploidy presenting in 1:18,000 males. Tremor has been previously reported in 47,XXY and 47,XYY syndromes, but has not been well described in 48,XXYY syndrome. Ten males with 48,XXYY syndrome had a standardized neurological examination and videotaping, which included the Clinical Rating Scale for Tremor and the International Cooperative Ataxia Rating Scale. All 10 cases had postural and kinetic tremor on physical examination. Other findings included mild gait ataxia, dysarthria, and nystagmus. Three cases are reviewed. Tremor is a common finding in children and young adults with 48,XXYY syndrome. Dosage alteration of genes on the sex chromosomes may be involved in the pathogenesis of this tremor. Karyotyping should be considered in individuals presenting with tremor and a history of developmental delay, learning disabilities, tall stature, or micro-orchidism.
Keywords: XXYY syndrome, sex chromosome abnormality, XYY, XXY, Klinefelter syndrome, tremor
48,XXYY syndrome is a rare form of sex chromosome aneuploidy occurring in approximately 1:18,000 males. 48,XXYY syndrome was previously considered a variant of Klinefelter syndrome (47,XXY) due to a similar physical phenotype including tall stature, hypergonadotropic hypogonadism, and microorchidism. However, a distinct phenotype is now recognized to include additional medical problems and more significant cognitive and psychological impairments.1,2 Tremor has been previously described in case reports in 48,XXYY syndrome3–5 and “essential tremor” has also been reported in children and adults with other common forms of sex chromosome aneuploidy, including 47,XXY and 47,XYY syndromes.6–9 It has been hypothesized that dosage alteration of genes on the sex chromosomes may predispose to the development of tremor.10 In this article, we present the results of standardized neurological examinations in 10 males with 48,XXYY syndrome with tremor to document and further characterize this finding in 48,XXYY syndrome. We also describe three cases and include the first video series of tremor in 48,XXYY syndrome.
SUBJECTS AND METHODS
The 10 subjects in this case series were ascertained during an annual XXYY meeting in New York, in 2007, at which 28 males aged 3–26 years with 48,XXYY and their families were in attendance. All males with 48,XXYY at the meeting with minimal to severe tremor were invited to participate (n = 14); 4 subjects declined due to interest in other activities. The other 14 males with XXYY at the meeting (9 males age 2–13; 5 males age 14+) did not report tremor symptoms and were not evaluated due to time constraints. The 10 subjects signed Institutional Review Board (IRB)-approved consent forms and additional consent for videotaping. Seven of the 10 subjects had been previously evaluated and included in a larger study on medical and psychological features in XXYY syndrome,1 the other three were not included in our previous research. Each subject had a standardized medical history, neurological examination, and was videotaped by a neurologist specializing in movement disorders (D.H.) and a developmental pediatrician with expertise in sex chromosome aneuploidy (N.T.).
The motor portion of the Clinical Rating Scale for Tremor (CRST)11 and the International Cooperative Ataxia Rating Scale (ICARS)12 were performed on each subject, with the entirety of the scales videotaped. The CRST motor portion includes objective assessment of rest, postural, and kinetic tremors, as well as objective functional rating of motor tasks. The ICARS evaluates categories including postural/gait/stance, limb movement, speech, and oculomotor. Higher scores on both of these scales imply worse tremor or ataxia. Statistical analysis to determine Pearson correlation for age and total tremor score (sum of CRST and ICARS scores) was calculated using SPSS. Family history of tremor was ascertained from the parents. Tremor frequency was measured (in Case 1 only) using the CATSYS 2000 system during a visit to UC-Davis per the protocol described in Allen et al.13
RESULTS
Clinical features of the patients are reported in Table 1. The mean age of the subjects was 18.3 ± 4.6. The mean motor CRST score was 10.2 ± 1.6 and the mean total ICARS was 12 ± 1.8. There was no significant correlation between the age of subjects and the severity of symptoms as measured by the total of the CRST and ICARS scores (Pearson r = −0.0002, P = 0.99).
TABLE 1.
Clinical features of 10 cases of 48,XXYY syndrome: highest CRST or ICARS score is based on highest particular item on the scale (item in parentheses)
| Case | Age | Motor CRST1 | Highest CRST1 score | Total ICARS2 | Highest ICARS score2 | Age at tremor onset | Family history of tremor? | Neurological exam descriptive features | Other medical features3 | Other psychological features3,4 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 22 | 12 | 2 (action tremor, handwriting) | 21 | 2 (multiple items) | 7 | Yes | Kinetic and postural tremor, nystagmus, mild dysarthria | Epilepsy, sleep apnea, esophageal spasms, hypogonadisma | 3 Borderline cognitive abilities, Autism Spectrum disorder, Obsessive-compulsive behavior, ADHDb—Inattentive |
| 2 | 13 | 18 | 2 (postural tremor) | 20 | 2 (ocular pursuits, spread feet) | 4 | Yes | Kinetic and postural tremor, saccadic pursuits | Cystic fibrosis, G.E. refluxc | 3 Learning disability, ADHD—Combined anxiety disorder |
| 3 | 17 | 19 | 3 (action tremor) | 13 | 3 (finger to nose) | 10 | No | Intention and postural tremor, widened stance | Scoliosis, asthma/allergies, mitral valve prolapse, hypogonadisma | 3 Borderline cognitive abilities, ADHD—Inattentive, autism spectrum disorder, Tic disorder |
| 4 | 24 | 10 | 2 (intention tremor) | 15 | 2 (multiple items) | 16 | No | Mild postural and kinetic tremor, nystagmus, mild gait ataxia | Seizures in childhood, cryptorchidism, inguinal hernia repair, hypogonadisma | 3 Learning disability, poor adaptive functioning, mood disorder |
| 5 | 13 | 8 | 2 (action tremor) | 10 | 2 (intention tremor) | 3 | Yes | Mild postural and kinetic tremor, dysarthria, widened stance | Strabismus, kyphosis, constipation | 3 Mild intellectual disability, obsessive-compulsive disorder, mood disorder, ADHD—combined subtype |
| 6 | 16 | 6 | 1 (multiple items) | 8 | 2 (dysarthria) | 12 | No | Mild kinetic and postural tremor, dysarthria | Asthma/allergies, gilbert’s disease, scoliosis, hypogonadisma | 3 Borderline cognitive abilities, autistic disorder, anxiety disorder |
| 7 | 26 | 12 | 2 (intention tremor) | 15 | 2 (finger to finger, finger to nose) | 15 | Yes | Mild kinetic and postural tremor, dysarthria, mild gait ataxia | 3 Radioulnar synostosis, seizures in childhood, strabismus, hypogonadisma | Mild intellectual disability, mood disorder |
| 8 | 19 | 4 | 1 (multiple items) | 3 | 1 (multiple items) | 9 | No | Unilateral kinetic tremor, widened stance | Hypothyroidism, pes planus, hypogonadisma | 3 Learning disability, ADHD—Combined subtype |
| 9 | 19 | 4 | 1 (multiple items) | 6 | 1 (multiple items) | 11 | Yes | Mild postural and kinetic tremor, dysarthria | Asthma in childhood, hypogonadisma | Learning disability, anxiety disorder |
| 10 | 14 | 9 | 1 (multiple items) | 9 | 1 (multiple items) | 9 | No | Kinetic tremor, leg dysmetria, gait ataxia | Asthma, hypogonadisma | 3 Learning disability, ADHD—Combined |
CRST, Clinical Rating Scale for Tremor. Higher scores indicate increased symptoms.
ICARS, International Cooperative Ataxia Rating Scale. Higher scores indicate increased symptoms.
This feature was noted as the primary indication for genetic testing leading to patient being diagnosed with XXYY.
Early speech delays were present in all patients. Seven of the ten had delayed gross motor milestones.
Hypergonadotropic hypogonadism (testosterone deficiency) characteristic of XXYY syndrome, 6/8 subjects were on testosterone replacement therapy.
Attention Deficit Hyperactivity Disorder.
Gastroesophageal reflux.
Half of the subjects had a family history of tremor. There was no significant difference in CRST or total ICARS scores between groups when compared based on positive or negative family history.
Case Descriptions
Case 1
A 22-year-old left-handed male reported tremor with handwriting since age 7. He noticed the tremor when playing video games or eating. The tremor had progressively worsened over the last few years and was exacerbated by stress and sleep deprivation. A trial of atenolol 10 mg was stopped due to an episode of syncope, and a trial of primidone was discontinued due to sleepiness. Neither medication improved his tremor symptoms. He was taking propranolol 40 mg per day some improvement in his tremor. He reported balance difficulties with falling and stumbling over the prior 3–4 months.
He was diagnosed with 48,XXYY syndrome at 14 years of age due to a history of a borderline Intelligent Quotient (IQ), autism spectrum disorder, and mild dysmorphic features. He also had sleep apnea, seizures, esophageal spasms, and hypogonadism. Medications included testosterone injections, carbamazepine, methylphenidate, hyoscyamine sulfate, and cetirizine. His father and 4 uncles had tremor. Neurological examination showed persistent but moderate gaze-evoked nystagmus and mild dysarthria. He had postural and kinetic tremor (Fig. 1), with one step deviation on tandem gait. Evaluation of his tremor using the CATSYS system showed that his tremor frequency was 6.5 Hz ± 1.3 Hz.
FIG. 1.
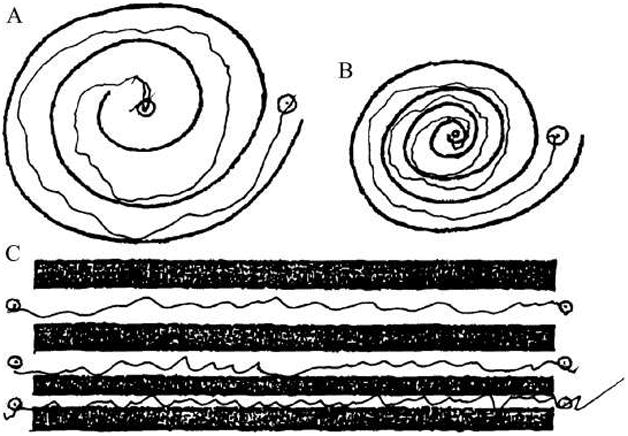
Example of handwriting of spirals and lines in Case 1.
Case 2
A 13-year-old right-handed male presented with tremor that began at 4 years of age. He reported shaking with handwriting and eating, with worsening of tremor during times of sleep deprivation or increased stress. His medical history included a diagnosis of cystic fibrosis at 3 years of age when he presented with rectal prolapse. He was diagnosed with 48,XXYY at 7 years of age due to learning disabilities and attention deficit hyperactivity disorder. He had not been on medications for tremor, and his medications were sertaline, omeprazole, and inhaled tobramycin. Neurological examination showed saccadic ocular pursuit and postural tongue tremor. He had moderate modification of speech fluency. He had postural tremor and kinetic tremor.
Case 3
A 17-year-old right-handed male presented with shaking of the hands since 10 years of age. He noticed his hands shaking when biting his fingernails, writing, or eating ice cream. He no longer used glass cups due to the severity of tremor and the tremor worsened when he was nervous. He also reported worsening problems with his balance. He was diagnosed with 48,XXYY syndrome at 4 years of age due to language delays. His medical history was significant for asthma, scoliosis, hypogonadism, anxiety, and autism. He had no family history of tremor. His medications included fluoxetine and testosterone gel. His examination showed saccadic ocular pursuit and postural and kinetic tremor. He had a widened stance, but was able to tandem without deviations.
DISCUSSION
In this study, 10 males with 48,XXYY were examined and had tremor of varying severity. The tremor was kinetic, postural, or both, and was usually rated as mild on the CRST. The presence of tremor in these males is consistent with other reports from our group, in which a recent review of 95 cases of 48,XXYY syndrome described kinetic tremor in 8% of individuals less than 10 years of age, 62% of individuals aged 11–20 years, and in 71% of individuals were adults.1 In the majority of cases, the tremor most commonly begins in early adolescence. The patients in this study described worsening of tremor over time, which was corroborated by family, but this has not been studied in a longitudinal manner. There was no significant correlation between age and CRST/ICARS scores in our sample. Although the sample size was small, there were also no significant differences in CRST and ICARS scores between those with and without a family history of tremor.
Baughman first described “essential tremor” in two 47,XXY males in 1969,7 and Daly described intention tremor in 10/12 males with 47,XYY.14 Tremor in 47,XYY and 47,XXY males was subsequently quantified in a blinded, controlled study using tremor recording equipment, in which physiologic tremor was found in 83% of the 47,XYY males and 64% of the 47,XXY males. Intention tremor was less frequent, although present in 50% of 47,XYY and 57% of 47,XXY.15 Based on these studies, tremor may be a common feature in the phenotype of males with sex chromosome aneuploidy, yet is often not included in clinical descriptions of these genetic syndromes.16–18
The tremor in sex chromosome aneuploidy is not consistent with essential tremor (ET) or other well-defined tremor disorders. The diagnostic criteria for ET require the presence of both postural and kinetic tremor, the exclusion of “other basal ganglionic disorders,” the absence of psychogenic features,19 and require the exclusion of cerebellar involvement and drugs or conditions known to worsen physiologic tremor.20 ET is rare in childhood (1/500 children).21 The age of onset of tremor, associated chromosomal abnormality, and presence of other cerebellar signs in our cases, suggest that the tremor associated with 48,XXYY is a different entity than ET.
Volumetric neuroimaging data are not yet available for 48,XXYY; however, studies in 47,XXY show a significantly decreased caudate volume compared with 46,XY (in addition to smaller frontal and temporal lobe volumes),22 as well as decreases in cerebellar lobe volumes.23 Thus, basal ganglionic or cerebellar dysfunction may by involved in tremor symptoms in both 47,XXY and 48,XXYY. In 48,XXYY, review of 35 brain MRI’s obtained for clinical reasons showed a 46% incidence of T2 white matter hyperintensities and a 23% incidence of enlarged ventricles. In that study, males with XXYY with white matter hyperintensities did not have increased rates of tremor when compared with those without white matter findings.1
The phenotype of 48,XXYY and other forms of supernumerary sex chromosome aneuploidy are thought to result from gene dosage effects of X chromosome genes that escape X-inactivation and/or overexpression of Y chromosome genes from the extra sex chromosomes. However, the specific genes associated with the abnormal phenotypic features have not been identified. We hypothesize that tremor in 48,XXYY syndrome results from dysregulation of a sex chromosome gene, leading to altered neurodevelopment or neurophysiology and subsequent tremor. Similar findings of tremor in both 47,XXY and 47,XYY suggest that overexpression of genes homologous on the X and Y chromosomes (pseudoautosomal regions)24 are likely involved.10 Understanding gene dysregulation in 48,XXYY might serve to enhance understanding regarding the etiology of kinetic and postural tremor in these patients and other patients with sex chromosome disorders.
There are several genes on the X chromosome that have been associated with tremor in other disorders. Fragile X-associated tremor/ataxia syndrome (FXTAS) is associated with tremor, ataxia, and peripheral neuropathy due to elevated levels of mRNA from the X-chromosome FMR1 gene in individuals with the fragile X premutation.25,26 Our subjects have a similar tremor and some subjects manifested cerebellar signs, such as mild gait ataxia, nystagmus, and dysarthria. However, the early age of presentation and lack of neuropathic features suggest that the tremor is caused by a different mechanism. Also, other studies suggest that the FMR1 gene is always X-inactivated on the second X-chromosome in males with 47,XXY.27,28 Interestingly, a recent case report of a male presenting with atypical kinetic tremor being evaluated for FXTAS was instead found to have 47,XXY.29
Other X-chromosome disorders associated with tremor are located in the Xq22-27 region, and include Pelizaeus-Merzbacher disease (mutation of the PLP1 gene), Cabezas syndrome (X-linked mental retardation with short stature and hypogonadism; CUL4B gene), and leukoencephalopathy with chondroplasia.30–32 X-linked Spinal Bulbar Muscular Atrophy (Kennedy’s disease) results from a polyglutamine expansion mutation in the androgen receptor gene on the X chromosome and is also associated with tremor and hypogonadism.33 Although these disorders share some clinical features with 48,XXYY such as onset of tremor in childhood, cognitive deficits, and/or hypogonadism, they also have more significant neurological impairments and/or more progressive neurological disease than our 48,XXYY patients. The mechanism of hypogonadism is also different. Additionally, with the exception of some cases of Pelizaeus-Merzbacher disorder in which PLP1 duplication occurs, genetic mechanisms underlying the pathophysiology of these conditions do not involve increased gene dosage. The association of hypogonadism and tremor in Cabezas syndrome and Kennedy’s disease is also interesting; however, it is important to point out that 47,XYY is not associated with hypogonadism and most likely shares a common tremor pathophysiology with 48,XXYY. Genes on the Y chromosome have not yet been linked to tremor.
Current medical practice significantly under ascertains cases of sex chromosome aneuploidy, especially in the pediatric population. It is estimated that up to 75% of individuals with 47,XXY and 88% of 47,XYY remain undiagnosed in their lifetime, with less than half of known cases diagnosed before adulthood.34 These disorders are very common, with a prevalence of 1:650 for 47,XXY and 1:1,000 for 47,XYY. The 48,XXYY has a lower prevalence rate (1:18,000) and the rate of lifetime diagnosis is unknown. Clinically, the presence of tremor in a patient with a history of early developmental delays, learning disabilities, tall stature, or associated physical features such as micro-orchidism should prompt chromosome analysis to evaluate for sex chromosome aneuploidy. Future studies in this disorder may include prevalence and natural history studies, gene expression studies, medication trials, and direct comparison with patients with ET.
Supplementary Material
All three cases demonstrate postural tremor and kinetic tremor with finger-to-nose and pouring water. There was no tremor at rest.
Acknowledgments
We acknowledge grant support by Bonfils-Stanton Foundation, The XXYY Project, K23 NS052487 for D.A.H., and UC-Davis M.I.N.D. Institute. We acknowledge P. Adams for technical assistance. We thank all participants and their families. N.R.T. currently receives research support from the University of Colorado CTRC and The Children’s Hospital Research Institute.
Footnotes
Potential conflict of interest: The authors report no conflict of interest.
Additional Supporting Information may be found in the online version of this article.
Author Roles: Nicole Tartaglia: Research Project: Conception, obtaining, funding, organization, and execution; statistical analysis: Execution; Manuscript: Writing and revisions. Mariya Borodyanskya: Research Project: Organization, execution, and records review; Manuscript: Review, critique, revisions. Deborah Hall: Research Project: Execution; statistical analysis: Execution, video edition; Manuscript: Writing and revisions.
References
- 1.Tartaglia N, Davis S, Hench A, et al. A new look at XXYY syndrome: medical and psychological features. Am J Med Genet A. 2008;146:1509–1522. doi: 10.1002/ajmg.a.32366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Visootsak J, Graham JM., Jr Klinefelter syndrome and other sex chromosome aneuploidies. Orphanet J Rare Disease. 2006;1(42) doi: 10.1186/1750-1172-1-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Donati F, Gasser S, Mullis P, Braga S, Vassella F. 48,XXYY syndrome in a boy with essential tremor. Comparison with 120 cases from the literature. Monatsschr Kinderheilkd. 1992;140:216–219. [PubMed] [Google Scholar]
- 4.Baughman F, Mann JD. Ascertainment of seven YY males in a private neurology practice. JAMA. 1972;222:446–448. [PubMed] [Google Scholar]
- 5.Izumi S, Tsubahara A. Improvement of peripheral neuropathy by testosterone in a patient with 48,XXYY syndrome. Tokai J Exp Clin Med. 2000;25:39–44. [PubMed] [Google Scholar]
- 6.Boltshauser E, Meyer M, Deonna T. Klinefelter syndrome and neurological disease. J Neurol. 1978;219:253–259. doi: 10.1007/BF00312978. [DOI] [PubMed] [Google Scholar]
- 7.Baughman F. Klinefelter syndrome and essential tremor. Lancet. 1969;2:545. doi: 10.1016/s0140-6736(69)90244-x. [DOI] [PubMed] [Google Scholar]
- 8.Jakubowski L, Sabatowska M, Filipiak-Miastkowska I, et al. Neurological aspects of two patients with non-mosaic and mosaic polysomy of the X and Y chromosomes. Neurol Neurochir Pol. 1999;33:169–175. [PubMed] [Google Scholar]
- 9.Telfeian A, Boockvar J, Simuni T, Jaggi J, Skolnick B, Baltuch G. Efficacy of unilateral deep brain stimulation of the thalamic ventralis intermedius nucleus in a patient with bipolar disorder associated with klinefelter syndrome and essential tremor. Case report. J Neurosurg. 2000;93:127–128. doi: 10.3171/jns.2000.93.1.0127. [DOI] [PubMed] [Google Scholar]
- 10.Deng H, Le W, Jankovic J. Genetics of essential tremor. Brain. 2007;130:1456–1464. doi: 10.1093/brain/awm018. [DOI] [PubMed] [Google Scholar]
- 11.Fahn S, Tolosa E, Marin C. Clinical rating scale for tremor. In: Jankovic J, Tolosa E, editors. Parkinson’s disease and movement disorders. Baltimore-Munich: Urban & Schwarzenberg; 1998. pp. 225–234. [Google Scholar]
- 12.Trouillas P, Takayanagi T, Hallett M, et al. International cooperative ataxia rating scale for pharmacological assessment of the cerebellar syndrome. The Ataxia Neuropharmacology Committee of the World Federation of Neurology. J Neurol Sci. 1997;145:205–211. doi: 10.1016/s0022-510x(96)00231-6. [DOI] [PubMed] [Google Scholar]
- 13.Allen EG, Juncos J, Letz R, et al. Detection of early FXTAS motor symptoms using the CATSYS computerised neuromotor test battery. J Med Genet. 2008;45:290–297. doi: 10.1136/jmg.2007.054676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Daly R, Matthews C. Impaired motor function in XYY males. Neurology. 1974;24:655–658. doi: 10.1212/wnl.24.7.655. [DOI] [PubMed] [Google Scholar]
- 15.Boisen E, Rasmussen L. Tremor in XYY and XXY men. Acta Neurol Scand. 1978;58:66–73. doi: 10.1111/j.1600-0404.1978.tb02861.x. [DOI] [PubMed] [Google Scholar]
- 16.Simpson JL, Swerdloff RS, Samango-Sprouse CA, Rogol A. Management of Genetic Syndromes. 2. Hoobken, NJ: Wiley-Liss; 2005. Klinefelter syndrome; pp. 323–334. [Google Scholar]
- 17.Bojesen A, Gravholt CH. Klinefelter syndrome in clinical practice. Nat Clin Pract. 2007;4:192–204. doi: 10.1038/ncpuro0775. [DOI] [PubMed] [Google Scholar]
- 18.Geerts M, Steyaert J, Fryns JP. The XYY syndrome: a follow-up study on 38 boys. Genet Counsel (Geneva, Switzerland) 2003;14:267–279. [PubMed] [Google Scholar]
- 19.Louis E, Ford B, Lee H, Andrew H, Cameron G. Diagnostic criteria for essential tremor: a population perspective. Arch Neurol. 1998;55:823–828. doi: 10.1001/archneur.55.6.823. [DOI] [PubMed] [Google Scholar]
- 20.Cersosimo M, Koller W. Essential tremor. In: Watts R, Koller W, editors. Movement disorders. 2. New York: McGraw-Hill; 2004. pp. 437–438. [Google Scholar]
- 21.Jankovic J, Madisetty J, Vuong K. Essential tremor among children. Pediatrics. 2004;114:1203–1205. doi: 10.1542/peds.2004-0031. [DOI] [PubMed] [Google Scholar]
- 22.Giedd JN, Clasen LS, Wallace GL, et al. XXY (Klinefelter syndrome): a pediatric quantitative brain magnetic resonance imaging case-control study. Pediatrics. 2007;119:e232–e240. doi: 10.1542/peds.2005-2969. [DOI] [PubMed] [Google Scholar]
- 23.Lenroot RK, Shaw P, Clasen LS, Mackie S, Pierson R, Giedd JN. Comparison of cerebellar anatomy in a pediatric XXY population to XY males with and without ADHD. J Intellect Disabil Res. 2007;51:655. [Google Scholar]
- 24.Graves JA, Wakefield MJ, Toder R. The origin and evolution of the pseudoautosomal regions of human sex chromosomes. Hum Mol Genet. 1998;7:1991–1996. doi: 10.1093/hmg/7.13.1991. [DOI] [PubMed] [Google Scholar]
- 25.Hagerman PJ, Hagerman RJ. Fragile X-associated tremor/ataxia syndrome (FXTAS) Ment Retard Dev Disabil Res Rev. 2004;10:25–30. doi: 10.1002/mrdd.20005. [DOI] [PubMed] [Google Scholar]
- 26.Berry-Kravis E, Goetz CG, Leehey MA, et al. Neuropathic features in fragile X premutation carriers. Am J Med Genet A. 2007;143:19–26. doi: 10.1002/ajmg.a.31559. [DOI] [PubMed] [Google Scholar]
- 27.Paduch D. Faststart high fidelity PCR system simplifies study of epigenetics and DNA methylation. Biochemica. 2005;2:19. [Google Scholar]
- 28.Pena SD, Sturzeneker R. Molecular barr bodies: methylation-specific PCR of the human X-linked gene FMR-1 for diagnosis of Klinefelter syndrome. J Androl. 2003;24:809. doi: 10.1002/j.1939-4640.2003.tb03128.x. author reply 810. [DOI] [PubMed] [Google Scholar]
- 29.Harlow TL, Rodnitzky RL, Gonzalez-Alegre P. From essential tremor to Klinefelter through fragile X, an unexpected journey. Mov Disord. 2008;23:1328–1329. doi: 10.1002/mds.22033. [DOI] [PubMed] [Google Scholar]
- 30.Kim SJ, Yoon JS, Baek HJ, et al. Identification of proteolipid protein 1 gene duplication by multiplex ligation-dependent probe amplification: first report of genetically confirmed family of Pelizaeus-Merzbacher disease in Korea. J Korean Med Sci. 2008;23:328–331. doi: 10.3346/jkms.2008.23.2.328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Neubauer BA, Stefanova I, Hubner CA, et al. A new type of leukoencephalopathy with metaphyseal chondrodysplasia maps to Xq25-q27. Neurology. 2006;67:587–591. doi: 10.1212/01.wnl.0000230133.11951.75. [DOI] [PubMed] [Google Scholar]
- 32.Tarpey PS, Raymond FL, O’Meara S, et al. Mutations in CUL4B, which encodes a ubiquitin E3 ligase subunit, cause an X-linked mental retardation syndrome associated with aggressive outbursts, seizures, relative macrocephaly, central obesity, hypogonadism, pes cavus, and tremor. Am J Hum Genet. 2007;80:345–352. doi: 10.1086/511134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.La Spada AR, Wilson EM, Lubahn DB, Harding AE, Fischbeck KH. Androgen receptor gene mutations in X-linked spinal and bulbar muscular atrophy. Nature. 1991;352:77–79. doi: 10.1038/352077a0. [DOI] [PubMed] [Google Scholar]
- 34.Abramsky L, Chapple J. 47,XXY (Klinefelter syndrome) and 47,XYY: estimated rates of and indication for postnatal diagnosis with implications for prenatal counselling. Prenat Diagn. 1997;17:363–368. doi: 10.1002/(sici)1097-0223(199704)17:4<363::aid-pd79>3.0.co;2-o. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
All three cases demonstrate postural tremor and kinetic tremor with finger-to-nose and pouring water. There was no tremor at rest.