

Abstract
Background
The most commonly used method for unstable slipped capital femoral epiphysis (SCFE) remains in situ fixation. Depending on the surgeon’s preference, screws or Kirschner wires are used for stabilizing the slipped upper femoral epiphysis. The purpose of this study was to evaluate the ability of a single cannulated screw with a proximal threading to ensure stabilization, growth, and remodeling of the slipped epiphysis.
Methods
A retrospective study was performed identifying 23 children treated for unstable SCFE under 50° by means of a single cannulated screw with proximal threading. All patients attended a radiological evaluation immediately after surgery and at physeal closure. The width of the epiphysis cut by the Klein line, the width and length of the femoral neck, the centrocalcar distance (CCD) angle, and the articulotrochanteric distance (ATD) were evaluated.
Results
All patients had a stabilized epiphysis at the last follow-up, with no case of recurring slip. Radiological comparison of the affected side between the preoperative and the last follow-up evaluation showed a statistically significant improvement in the neck length and width.
Conclusion
Fixation of the epiphysis using proximally threaded screws allows the preservation of femoral neck growth. The cannulated screw with proximal threading seems to be a safe and relevant implant to help to restore a close-to-normal hip at skeletal maturity.
Keywords: Slipped capital femoral epiphysis, Fixation, Proximal threading cannulated screw, Growth
Introduction
Slipped capital femoral epiphysis (SCFE) is a common disorder of the adolescent hip. It is characterized by a displacement of the upper femoral epiphysis in a dorsal, medial, and caudal direction. Although a number of nonoperative and operative treatment strategies have been described [1–9], in situ fixation in order to stabilize the physis by effecting a closure of the physis is a treatment recommended by many surgeons.
Depending on the surgeon’s preference, screws [2, 4, 5, 10] or Kirschner wires [11, 12] are used for stabilizing the slipped upper femoral epiphysis. Most authors agree to support the observation that single cannulated screw fixation is associated with a lower complication rate [2, 4] but generates premature growth arrest. Significantly greater shortening of the femoral neck has been reported in patients with screw stabilization compared to other methods [13].
Kirschner wire pinning appears to be less compromising to the growth plate and to the remodeling capacities of the upper femur [14]. Single-pin fixation has been favored increasingly because the overall rate of complications seems to be directly related to the number of pins or screws inserted [14, 15].
In our opinion, the goal of a fixation device used for unstable SCFE should be stabilization while allowing continued growth. The purpose of this study was to evaluate the ability of a single cannulated screw with a proximal threading to ensure stabilization, growth, and remodeling of the slipped epiphysis.
Materials and methods
A retrospective study was performed identifying 23 children treated in our department between 2001 and 2005 for unstable SCFE under 50° by means of a single cannulated screw with proximal threading. Many investigations on the method of fixation in SCFE have been carried out on unstable hips. Unstable SCFE only were selected in this study in order to make a comparison possible. The population consisted of 14 boys and nine girls with a mean age of 11.4 years (range, 5–16 years) at the time of surgery. Clinical history was extracted from the patient files. The mean age at the time of surgery was 10.25 years for the girls (range, 5–13 years) and 12.6 years for the boys (range, 11–16 years). All had a unilateral slip. The left hip was the affected side in 59% of the cases.
Surgical technique
After admission in the department, all patients were initially treated with painkillers and placed at bed rest without any traction until early surgical procedure. All patients were operated within 12 h after admission. The surgical procedure consisted of percutaneous in situ fixation of the epiphysis with a single cannulated screw with a proximal threading. All procedures were performed on a fracture table under fluoroscopic control with the lower limb slightly internally rotated. In none of the cases was a SCFE reduced or manipulated to obtain reduction. The optimal screw location was perpendicular to the physis, with the tip of the screw located at the center of the epiphysis on the anteroposterior (AP) and the lateral views. The contralateral unaffected epiphysis was always fixed using the same cannulated screw and the same technique. The epiphysis was stabilized with a single 6.5-mm cannulated screw with a proximal 30-mm threading (Medicalex, France) (Fig. 1). The screw length varied from 60 to 110 mm.
Fig. 1.

Photograph showing two different sizes of cannulated screws with proximal threading
Postoperatively, all patients were allowed partial weight-bearing on the affected lower limb using crutches for 3–4 weeks.
Follow-up assessments
All patients attended a radiological evaluation immediately after surgery and at physeal closure. The mean follow-up was 31 months (range, 14–61 months). Preoperative, postoperative, and last follow-up AP and lateral projection radiographs were reviewed by an independent observer to evaluate growth and remodeling of the upper femur: the width of the epiphysis cut by the Klein line, the width and length of the femoral neck, the centrocalcar distance (CCD) angle, and the articulotrochanteric distance (ATD). The grade of the slip was defined as mild (<30°), moderate (30°–50°), or severe (>50°) using the lateral head-shaft angle as described by Southwick [16]. The length of the femoral neck was determined as the distance between the intertrochanteric line and the femoral head across the center of the femoral head. The width of the femoral neck was measured at the narrowest part of the neck, perpendicularly to the femoral neck axis. The CCD angle was measured between the line parallel to the femoral neck through the center of the femoral head and the axis of the femoral diaphysis. The ATD was defined as the distance between the summit of the greater trochanter and the summit of the femoral head. Radiological abnormalities such as avascular necrosis and chondrolysis was also noted. Measurements of the proximal femur should vary according to the amount of hip rotation at the time of taking the radiograph. We paid special attention to obtaining AP views with the patella strictly forward. However, the period between all the examinations was long. There was surely some inaccuracy in our measurements, but we could not perform a computed tomography (CT) scan for all patients.
Statistical analysis
The difference between the affected and the unaffected operated sides was evaluated using Student’s t-test for dependent samples. A P-value equal to or below 0.05 was considered to be statistically significant.
Results
On preoperative radiographs, there were 17 mild (<30°) and six moderate (<50°) unilateral SCFE. The average slip angle was 23° for the mildly and 46° for the moderately affected hips.
Despite the fact that there was no attempt of reduction maneuver, the immediate postoperative radiographs revealed that there were 22 cases of mild SCFE and only one case of a moderate SCFE. At the last follow-up, there were two cases of moderate SCFE as one hip developed a progressive slip despite the screw fixation. At the last follow-up, the average slip angle was 12° (21 cases) for mild SCFE and 48° (2 cases) for moderate SCFE.
The radiological assessments are recorded in Table 1.
Table 1.
Preoperative and last follow-up radiological assessments
| Radiological parameters | Affected side | Unaffected side | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Width of epiphysis cut by the Klein line (mm) | Mean CCD angle (°) | Mean neck length (mm) | Mean neck width (mm) | ATD (mm) | Width of epiphysis cut by the Klein line (mm) | Mean CCD angle (°) | Mean neck length (mm) | Mean neck width (mm) | ATD (mm) | |
| Preoperative | 1 | 134 | 56 | 34 | 21 | 5 | 135 | 56 | 34 | 25 |
| Last follow-up | 6 | 134 | 61 | 41 | 19 | 7 | 135 | 67 | 38 | 25 |
| Last follow-up−preoperative | 5 | 0 | 5 | 7 | −2 | 2 | 0 | 11 | 5 | −1 |
The average distance of the upper epiphysis cut by the Klein line on the affected side was 1 mm on the preoperative radiograph and 5 mm on the last follow-up radiograph.
On the unaffected side, the portion of epiphysis cut by the Klein line widened from 5.38 mm on the preoperative X-ray to 7 mm on postoperative evaluation. The progression with time of the width of epiphysis cut by the Klein line was statistically significantly lower on the unaffected than on the affected side (P = 0.004), revealing the remodeling effect on the affected side.
The preoperative CCD angle was 134° (range, 112–154°). At the last follow-up, it was 134° (range, 120–150°) (NS). On the unaffected side, the CCD angle remained at 135.5° pre- and postoperative evaluation.
At the last follow-up, both the affected and unaffected femoral necks had continued to grow. On the affected side, the length of the femoral neck was 56 mm (range, 32–70 mm) on the preoperative radiographs and 61 mm (range, 50–74 mm) at the last follow-up (P = 0.0016). The average growth was 5 mm. At the last follow-up, the mean length of the femoral neck was 67 mm on the unaffected side. On the unaffected side, the neck growth averaged 7 mm between the preoperative and the last follow-up evaluations. The unaffected side grew more than the affected side (P = 0.03).
On preoperative radiographs, the neck width was 34 mm (±4 mm) on the affected side and 33 mm (±4 mm) on the unaffected side (P = 0.24, NS). At the last follow-up, the neck width was 41 mm (±5 mm) and 38 mm (±4 mm), respectively. The difference was significant (P = 0.004), revealing the enlargement of the femoral neck on the affected side.
The ATD on the slipped side decreased by an average of 2 mm from 20 mm (±7 mm) on preoperative radiographs to 19 mm (±7 mm) at the last follow-up. On the unaffected side, this distance decreased by an average of 1 mm from 25 mm (±7 mm) to 24 mm (±7 mm). At the last follow-up, there was no statistically significant difference between the normal and slipped side relative to the evolution of the ATD (P = 0.44).
There were no cases occurrences of chondrolysis or avascular necrosis at the last follow-up.
In eight patients (six boys and two girls), the growth of the femoral neck over the unthreaded portion of the screw left the epiphysis with no mechanical support, as if the epiphysis was “growing away”. The screw had to be changed once for a longer one in seven of these patients. In the last patient (aged 5 years at the time of diagnosis), the screw had to be changed three times and screwed further once (Fig. 2).
Fig. 2.
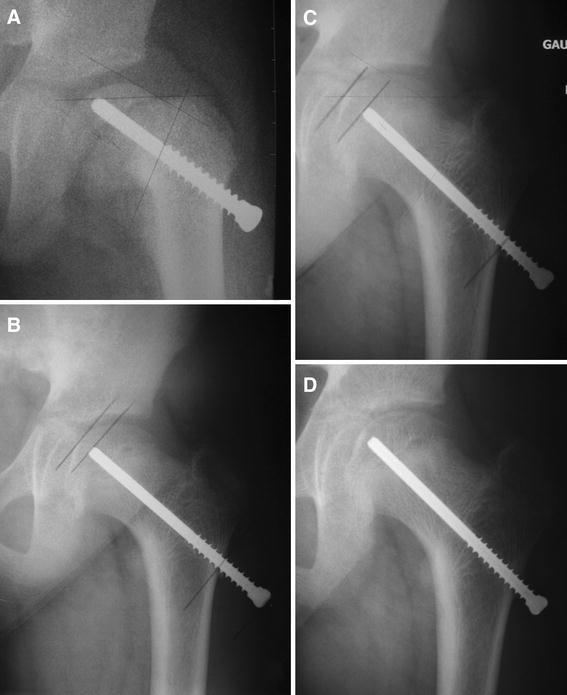
a Immediate post-operative anteroposterior (AP) view showing the slipped capital femoral epiphysis (SCFE) fixed with one cannulated screw with proximal threading. b Same patient; anteroposterior view 8 months after surgery. c Same patient; anteroposterior view 16 months after surgery. d Same patient; anteroposterior view 20 months after initial fixation. Between parts c and d, the screw has been screwed in further in order to keep the tip of the screw in the epiphysis and, therefore, to avoid further slippage
Discussion
The purpose of this study was to evaluate the ability of a single cannulated screw with a proximal threading to ensure stabilization, growth, and remodeling of the slipped epiphysis.
The type of implant used to fix the epiphysis remains controversial. Screw fixation seems to be associated with a lower complication rate [2, 4, 10, 17, 18]. Therefore, single-screw fixation is, at present, the most common treatment for SCFE [19]. The implant commonly used is a distally threaded cannulated screw. The main consequence of the use of distally threaded screws is the femoral neck length shortening. Morscher et al. [13] showed significantly greater shortening of the femoral neck in patients treated with screws than in patients treated with other methods (1.2 vs. 0.6 cm). The neck length itself is important for hip function. An unphysiological offset may influence the biomechanical function of the muscles around the hip and may lead to stress concentration, which might result in the development of osteoarthritis [13]. Moreover, it has been recently demonstrated that the disturbed upper femoral contour and shape resulting from SCFE may lead to femoroacetabular impingement [20–22]. Ideally, epiphyseal fixation in SCFE should be performed with the implant that is less compromising for growth and remodeling of the proximal femur. Seller et al. [14] reported that the averaged femoral neck lengths were 5.7 mm shorter in the affected hips than in the unaffected hips at the last follow-up in their patients treated with Kirschner wires. It is less than the difference reported by Morscher et al. [13] after fixation with distally threaded screws (1.2 cm).
In the present study, all patients had a stabilized epiphysis at the last follow-up, with no case of recurring slip. All but two patients had closed physeal plates on hip radiographs. The cannulated screw with a proximal threading was efficient in stabilizing SCFE without any complications.
Radiological comparison of the affected side between the preoperative and the last follow-up evaluations showed a statistically significant improvement of the neck length and width. However, these measurements were significantly higher in the unaffected side. The proximal threading seems to allow a significant growth of the proximal femur on the affected side but the remaining growth potential is lower than in the unaffected side. Our findings are very close to those reported by Seller et al. in their series of patients treated with Kirschner wires [14]. Fixation of the epiphysis using proximally threaded screws allows the preservation of the femoral neck growth as if Kirschner wires had been used. Placing a single screw in the femoral neck is de facto associated with a lower risk of intra-operative complication [23] in comparison to placing Kirschner wires that need repetition of the procedure three times. With multiple pins, the possibility that one or more will protrude into the joint is increased and pin protrusion can be associated with the development of chondrolysis. Guzzanti et al. [24] have used a modified cannulated screw with a short distal threaded segment placed entirely within the epiphysis. They kept the screw head at 2–3 cm lateral to the lateral femoral cortex in order to allow continued physeal growth. This is also a seducing stabilizing method which allowed significant remodeling of the proximal femur anatomy in their series. The principle is similar and the results comparable to the current series.
Unaffected contralateral side hips were used as controls to compare the femoral growth after screw fixation. It would have also been interesting to compare our patients with patients treated with distal threaded screws to verify the effect of proximal threaded screws. However, in our hands, all patients with unstable SCFE are now treated with proximal threading cannulated screws. We did not have a population of patients treated with distal threaded screws to make a comparison study possible.
Interestingly, the width of the epiphysis crossed by the Klein line significantly improved with time, suggesting a significant remodeling of the epiphysis. On the other hand, one could argue that this improvement of the upper femoral morphology was also due to the intra-operative partial reduction of the slippage. Indeed, despite the care taken not to reduce the epiphysis, the immediate postoperative radiographs revealed that, in five cases, the slippage improved from a moderate to a mild grade. However, trying to prevent proximal growth plate closure is, for us, crucial in order to improve the proximal femoral shape and decrease the risk of femoroacetabular impingement.
Proximal threading cannulated screws seem to allow continued physeal growth and to improve the shape of the proximal femoral anatomy. We now routinely use proximal threading cannulated screws for all SCFE. In our opinion, there is no additional risk to using this device, even in older patients. A physeal closure is more likely to occur close to skeletal maturity, but the growth potential is less significant. Therefore, one may object to using this type of fixation in older patients due to the risk of further slippage and the limited benefit on the shape of the proximal femur. However, the proximal threading cannulated screws may significantly improve the management of young SCFE patients.
Prophylactic pinning of the contralateral unaffected side was performed, as patients who are first seen with unilateral SCFE are at a 2.3 times greater risk for the development of a contralateral slip than those who have never had a slip [25]. Some authors recommend prophylactic pinning of the contralateral hip because of this increased risk of contralateral slip and the noted association between SCFE and the development of osteoarthritis [26–28].
The management of SCFE is still a controversial topic in pediatric orthopedics. It is clear that there is a premature development of advanced osteoarthritis of the adult hip joint in SCFE patients [29]. It is, therefore, mandatory to restore a normal anatomy and function of the hip before irreversible articular lesions are made. Significant improvement of the surgical management has been recently performed. In our opinion, the cannulated screw with proximal threading seems to be a safe and relevant implant to help restore a close-to-normal hip at skeletal maturity.
Acknowledgments
Each author certifies that his or her institution has approved the reporting of this case report, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
Conflict of interest
Each author certifies that he or she has no commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
Footnotes
Level of evidence: level IV.
References
- 1.Thomsen L, Vialle R, Maillet M, Mary P, Damsin JP, Filipe G. The progressive longitudinal traction reduction of unstable slipped capital femoral epiphysis: preliminary results in 11 patients. J Child Orthop. 2007;1(2):121–125. doi: 10.1007/s11832-007-0030-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rostoucher P, Bensahel H, Pennecot GF, Kaewpornsawan K, Mazda K. Slipped capital femoral epiphysis: evaluation of different modes of treatment. J Pediatr Orthop B. 1996;5(2):96–101. doi: 10.1097/01202412-199605020-00008. [DOI] [PubMed] [Google Scholar]
- 3.Rao SB, Crawford AH, Burger RR, Roy DR. Open bone peg epiphysiodesis for slipped capital femoral epiphysis. J Pediatr Orthop. 1996;16(1):37–48. doi: 10.1097/01241398-199601000-00008. [DOI] [PubMed] [Google Scholar]
- 4.de Sanctis N, Di Gennaro G, Pempinello C, Corte SD, Carannante G. Is gentle manipulative reduction and percutaneous fixation with a single screw the best management of acute and acute-on-chronic slipped capital femoral epiphysis? A report of 70 patients. J Pediatr Orthop B. 1996;5(2):90–95. doi: 10.1097/01202412-199605020-00007. [DOI] [PubMed] [Google Scholar]
- 5.Aronsson DD, Loder RT. Treatment of the unstable (acute) slipped capital femoral epiphysis. Clin Orthop Relat Res. 1996;322:99–110. [PubMed] [Google Scholar]
- 6.Fish JB. Cuneiform osteotomy of the femoral neck in the treatment of slipped capital femoral epiphysis. A follow-up note. J Bone Joint Surg Am. 1994;76(1):46–59. doi: 10.2106/00004623-199401000-00007. [DOI] [PubMed] [Google Scholar]
- 7.Ward WT, Stefko J, Wood KB, Stanitski CL. Fixation with a single screw for slipped capital femoral epiphysis. J Bone Joint Surg Am. 1992;74(6):799–809. [PubMed] [Google Scholar]
- 8.Aronson DD, Carlson WE. Slipped capital femoral epiphysis. A prospective study of fixation with a single screw. J Bone Joint Surg Am. 1992;74(6):810–819. [PubMed] [Google Scholar]
- 9.Weiner DS, Weiner S, Melby A, Hoyt WA., Jr A 30-year experience with bone graft epiphysiodesis in the treatment of slipped capital femoral epiphysis. J Pediatr Orthop. 1984;4(2):145–152. doi: 10.1097/01241398-198403000-00001. [DOI] [PubMed] [Google Scholar]
- 10.Jamil W, Allami MK, Varghese B, Almaiyah M, Giannoudis P. Screw placement in slipped upper femoral epiphysis: is good the enemy of better? J Child Orthop. 2007;1(3):181–186. doi: 10.1007/s11832-007-0036-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Strong M, Lejman T, Michno P, Sulko J. Fixation of slipped capital femoral epiphyses with unthreaded 2-mm wires. J Pediatr Orthop. 1996;16(1):53–55. doi: 10.1097/01241398-199601000-00010. [DOI] [PubMed] [Google Scholar]
- 12.Seller K, Raab P, Wild A, Krauspe R. Risk–benefit analysis of prophylactic pinning in slipped capital femoral epiphysis. J Pediatr Orthop B. 2001;10(3):192–196. [PubMed] [Google Scholar]
- 13.Morscher E, Staubli A, Meyer S, Imhoff A. 5.) 10-year results after epiphyseolysis capitis femoris. A) 10-year results with nails and screws in epiphyseolysis capitis femoris. Orthopade. 1979;8(1):60–64. [PubMed] [Google Scholar]
- 14.Seller K, Wild A, Westhoff B, Raab P, Krauspe R. Clinical outcome after transfixation of the epiphysis with Kirschner wires in unstable slipped capital femoral epiphysis. Int Orthop. 2006;30(5):342–347. doi: 10.1007/s00264-006-0110-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kumm DA, Lee SH, Hackenbroch MH, Rütt J. Slipped capital femoral epiphysis: a prospective study of dynamic screw fixation. Clin Orthop Relat Res. 2001;384:198–207. doi: 10.1097/00003086-200103000-00023. [DOI] [PubMed] [Google Scholar]
- 16.Southwick WO. Osteotomy through the lesser trochanter for slipped capital femoral epiphysis. J Bone Joint Surg Am. 1967;49(5):807–835. [PubMed] [Google Scholar]
- 17.Goodman WW, Johnson JT, Robertson WW., Jr Single screw fixation for acute and acute-on-chronic slipped capital femoral epiphysis. Clin Orthop Relat Res. 1996;322:86–90. [PubMed] [Google Scholar]
- 18.Uglow MG, Clarke NM. The management of slipped capital femoral epiphysis. J Bone Joint Surg Br. 2004;86(5):631–635. doi: 10.1302/0301-620X.86B5.15058. [DOI] [PubMed] [Google Scholar]
- 19.Loder RT. Slipped capital femoral epiphysis in children. Curr Opin Pediatr. 1995;7(1):95–97. doi: 10.1097/00008480-199502000-00018. [DOI] [PubMed] [Google Scholar]
- 20.Leunig M, Horowitz K, Manner H, Ganz R. In situ pinning with arthroscopic osteoplasty for mild SCFE: a preliminary technical report. Clin Orthop Relat Res. 2010;468:3160–3167. doi: 10.1007/s11999-010-1408-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Leunig M, Casillas MM, Hamlet M, Hersche O, Nötzli H, Slongo T, Ganz R. Slipped capital femoral epiphysis: early mechanical damage to the acetabular cartilage by a prominent femoral metaphysis. Acta Orthop Scand. 2000;71(4):370–375. doi: 10.1080/000164700317393367. [DOI] [PubMed] [Google Scholar]
- 22.Fraitzl CR, Käfer W, Nelitz M, Reichel H. Radiological evidence of femoroacetabular impingement in mild slipped capital femoral epiphysis: a mean follow-up of 14.4 years after pinning in situ. J Bone Joint Surg Br. 2007;89(12):1592–1596. doi: 10.1302/0301-620X.89B12.19637. [DOI] [PubMed] [Google Scholar]
- 23.Morrissy RT. Slipped capital femoral epiphysis technique of percutaneous in situ fixation. J Pediatr Orthop. 1990;10(3):347–350. doi: 10.1097/01241398-199005000-00010. [DOI] [PubMed] [Google Scholar]
- 24.Guzzanti V, Falciglia F, Stanitski CL. Slipped capital femoral epiphysis in skeletally immature patients. J Bone Joint Surg Br. 2004;86(5):731–736. doi: 10.1302/0301-620X.86B5.14397. [DOI] [PubMed] [Google Scholar]
- 25.Castro FP, Jr, Bennett JT, Doulens K. Epidemiological perspective on prophylactic pinning in patients with unilateral slipped capital femoral epiphysis. J Pediatr Orthop. 2000;20(6):745–748. doi: 10.1097/01241398-200011000-00009. [DOI] [PubMed] [Google Scholar]
- 26.Boyer DW, Mickelson MR, Ponseti IV. Slipped capital femoral epiphysis. Long-term follow-up study of one hundred and twenty-one patients. J Bone Joint Surg Am. 1981;63(1):85–95. [PubMed] [Google Scholar]
- 27.Hägglund G, Bylander B, Hansson LI, Kärrholm J, Selvik G, Svensson K. Longitudinal growth of the distal fibula in children with slipped capital femoral epiphysis. J Pediatr Orthop. 1986;6(3):274–277. doi: 10.1097/01241398-198605000-00003. [DOI] [PubMed] [Google Scholar]
- 28.Plötz GM, Hippe P, Hassenpflug J. “Recurrent” epiphysiolysis capitis femoris—need for simultaneous stabilization of both hip joints. Z Orthop Ihre Grenzgeb. 1998;136(6):534–541. doi: 10.1055/s-2008-1045182. [DOI] [PubMed] [Google Scholar]
- 29.Abraham E, Gonzalez MH, Pratap S, Amirouche F, Atluri P, Simon P. Clinical implications of anatomical wear characteristics in slipped capital femoral epiphysis and primary osteoarthritis. J Pediatr Orthop. 2007;27(7):788–795. doi: 10.1097/BPO.0b013e3181558c94. [DOI] [PubMed] [Google Scholar]