

An 89-year-old woman presented with chest pain, shortness of breath, and cough. She had recently been treated for bronchitis. A noteworthy aspect of her medical history was hypothyroidism. Upon her hospital admission, auscultation revealed bibasilar crackles. Chest radiography disclosed pulmonary congestion and a slightly enlarged cardiac silhouette. Electrocardiography showed sinus rhythm and an anterior infarct of indeterminate age. Blood tests showed elevated creatine kinase–MB (8.8 ng/mL) and elevated cardiac troponin T values (2.43 ng/mL). Cardiac magnetic resonance (CMR) imaging revealed left and right ventricular apical akinesia and basal hyperkinesia, with severely impaired biventricular systolic function (Fig. 1). Delayed-enhancement imaging showed full-thickness viable myocardium in both ventricles, indicating that no myocardial infarction had occurred (Fig. 2).
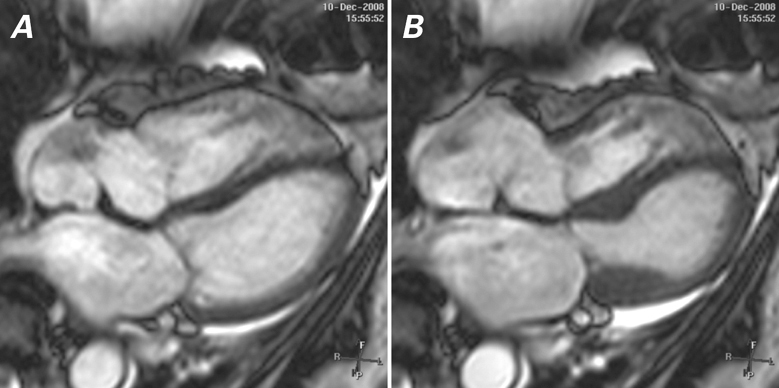
Fig. 1 Cardiac magnetic resonance imaging (4-chamber views) shows apical ballooning of the right and left ventricles at A ) end-diastole and B ) end-systole. Real-time motion image is available at www.texasheart.org/journal.
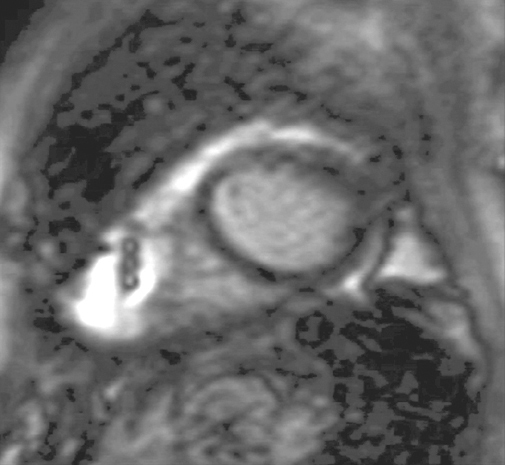
Fig. 2 Delayed-enhancement cardiac magnetic resonance imaging of the distal left and right ventricles shows absence of scarring. Real-time motion image is available at www.texasheart.org/journal.
Because of the patient's age, cardiac catheterization was deferred. Takotsubo cardiomyopathy (transient apical ballooning syndrome) was diagnosed. The patient was treated with aspirin, β-blockers, and angiotensin-converting enzyme inhibitors. At 4 weeks, follow-up echocardiography showed normal left and right ventricular systolic function.
Comment
Takotsubo cardiomyopathy is an acute syndrome that mimics ST-segment-elevation myocardial infarction1 and is often preceded by emotional or physical stress. The syndrome is characterized by transient wall-motion abnormalities that affect the apical left ventricle and sometimes also the right ventricle. Right ventricular involvement presents regional wall-motion abnormalities similar to those of isolated left ventricular involvement. When present, however, right ventricular involvement is associated with a longer, more complicated hospital course.2,3 Most patients recover completely within a few weeks.
Our case is special because CMR provided a means for the comprehensive evaluation of wall-motion abnormalities in both ventricles, as well as for the evaluation of myocardial viability.4 Takotsubo cardiomyopathy commonly occurs in women, and CMR can be particularly advantageous in providing vital information for establishing the diagnosis and, in selected cases, for obviating the need of invasive angiography.
Supplementary Material
References
- 1.Desmet WJ, Adriaenssens BF, Dens JA. Apical ballooning of the left ventricle: first series in white patients. Heart 2003;89 (9):1027–31. [DOI] [PMC free article] [PubMed]
- 2.Elesber AA, Prasad A, Bybee KA, Valeti U, Motiei A, Lerman A, et al. Transient cardiac apical ballooning syndrome: prevalence and clinical implications of right ventricular involvement. J Am Coll Cardiol 2006;47(5):1082–3. [DOI] [PubMed]
- 3.Prasad A, Lerman A, Rihal CS. Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): a mimic of acute myocardial infarction. Am Heart J 2008;155(3):408–17. [DOI] [PubMed]
- 4.Teraoka K, Kiuchi S, Takada N, Hirano M, Yamashina A. Images in cardiovascular medicine. No delayed enhancement on contrast magnetic resonance imaging with Takotsubo cardiomyopathy. Circulation 2005;111(16):e261–2. [DOI] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.