

Abstract
A 71-year-old female presented with recurrent sigmoid volvulus. In the current admission, her symptoms were not settling on conservative measures and subsequently went on to have laparotomy. During laparotomy, along with the sigmoid volvulus, there was associated gallbladder torsion. About 500 cases of gallbladder volvulus have been published in literature, however, in our literature search, the authors did not find any similar published case presenting with volvulus involving the gallbladder and the sigmoid colon at the same time. This patient went onto have cholecystectomy and sigmoid colectomy and had a good postoperative recovery and was discharged on the tenth postoperative day.
At 6-week postoperative follow-up, she was doing well with no specific concerns.
Background
We thought this case was rare and interesting because,
-
▶
A theoretical explanation was given several years ago for colonic contractions as a cause for gallbladder volvulus, but in our literature search we could not find a similar case published which makes this case a rare and unique presentation.
-
▶
Two surgical abdominal emergency conditions in one patient at the same time are not common.
-
▶
During laparotomy, even when obvious pathology is found always, one should do a complete thorough inspection of other organs.
Though 500 cases of gallbladder torsion have been published in literature, this case has a unique presentation with sigmoid volvulus and presumably the strong contractions associated with sigmoid obstruction leading to gallbladder torsion. These findings of our case report matched Levine's postulation,1 published 50 years ago.
This case report also reinforces the reader that one has to always be thorough in the clinical approach to think of rarer possibilities, and also to do a complete search during laparotomy for other possible pathologies.
Case presentation
A 71-year-old female presented with a sudden onset central/right iliac fossa pain which was colicky and aching in nature with no radiation. She had non-bilious vomiting for 2 days prior to admission and had opened her bowels regularly during this time. She had a decreased appetite but no weight loss.
A month ago, she was admitted with sigmoid volvulus which was successfully decompressed using colonoscopy. The patient was discharged home when she was able to tolerate diet and fluids and had resumed normal bowel activity. Her other medical history included a caesarean section and hypertension.
On examination her abdomen was mildly distended and a tender lower abdominal swelling was palpable.
An abdominal x-ray showed gaseous distension of the ascending and transverse colon. Her caecum measured roughly 9 cm. There was gas within the descending sigmoid colon and rectum, with stool within the rectum. Blood tests showed a raised white cell count (15.82), slightly raised C reactive protein (10) and low sodium (130).
The day after her admission, she began to complain of a sharp right upper quadrant (RUQ) pain that radiated to her back. She was mildly tender over that area. Her abdomen was still soft, bowel sounds were present and she was tolerating oral sips of fluid. Her blood results now showed a raised alanine transaminase (138). At this stage, an ultrasound (US) scan of her biliary tree was requested on suspicion of cholecystitis.
During the fourth day of her admission, it became evident that she had visible peristalsis with increasing abdominal distension. Her abdomen was soft and only tender in the RUQ.
A gastrograffin enema was performed on day 4 that showed a ‘beak sign’ strongly suggestive of sigmoid volvulus. Based upon the clinical situation of unresolving obstruction with imaging, suggestive of volvulus, she underwent an explorative laparotomy and unfortunately the US scan of her biliary tree had still not happened by this time.
Investigations
A gastrograffin enema – showed a ‘beak sign’ strongly suggestive of sigmoid volvulus.
An US scan was requested as patient had RUQ pain/tenderness, however, this patient symptoms/signs detoriated and she underwent laparotomy before the US scan of her biliary tree happened.
Treatment
During laparotomy, two distinct pathologies were discovered: sigmoid volvulus (figure 1) and torsion of the gallbladder (figure 2). The gallbladder was found to be wrapped by the transverse colon. On releasing the adhesions, it became evident that the gallbladder had twisted anticlockwise. It was hanging freely on its pedicle with no attachment to the liver. A sigmoid colectomy with primary anastomosis and cholecystectomy was performed. The histology of the gallbladder was reported as acute gangrenous cholecystitis.
Figure 1.
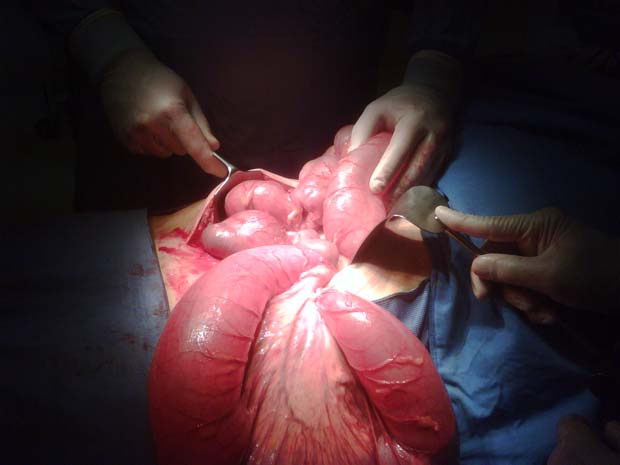
Sigmoid volvulus.
Figure 2.

Gangrenous torted gallbladder.
Outcome and follow-up
During her postoperative stay in intensive transport unit, she developed acute coronary syndrome which was treated. She was discharged back to the ward on the fifth postoperative day. She made an uneventful recovery and was discharged home, 10 days postoperatively.
Discussion
Since Wendell's first description of gallbladder volvulus in 1898, approximately 500 cases have been reported in the literature. It occurs due to torsion of the gallbladder along its long axis resulting in a compromised vascular supply and subsequent necrosis of the gallbladder. Based on the degree of rotation, the volvulus is described as incomplete if it is less than 180° and complete if greater than 180° rotation.2
Gallbladder volvulus occurs commonly in the older population with a female to male ratio of 3:1.3 Its occurrence in children was first published in 1925 and since then several cases have been reported with boys being affected more frequently than girls.3
The exact factors for the gallbladder to tort are unknown. Presence of a redundant mesentery is a common feature in all these patients. Only gallbladders which possess a mesentery or which hang free with a mesentery restricted to cystic duct can undergo torsion.1 A congenital redundant mesentery is noted in 5% of individuals. In the older population, liver atrophy, loss of visceral fat, visceroptosis or spinal deformities can lead to a redundant mesentery predisposing to volvulus of the gallbladder.2 3 Strong peristaltic waves from surrounding organs like the stomach, duodenum and colon can precipitate a free-lying gallbladder to tort.1 In our patient, the gallbladder was hanging freely from the liver with a thin mesentry restricted to cystic duct and peristaltic waves from the sigmoid volvulus may have contributed to the anticlockwise torsion of the gallbladder.
Clinically incomplete torsion often presents with right sided abdominal pain and vomiting, mimicking biliary colic. Complete torsion can present suddenly with excruciating RUQ pain. Occasionally a very low-lying, floating gallbladder can present as appendicitis. In most cases, it is an intraoperative diagnosis made at the time of laparotomy/laparoscopy.
Radiological findings are similar to that of cholecystitis. Features suggestive of gallbladder volvulus on CT scan include a cystic duct located to the right of the gallbladder, a conical structure at the neck and an unusual position of the gallbladder, especially a horizontal lie.4
Treatment is cholecystectomy. An early diagnosis and treatment can have a significant impact on morbidity and mortality.
Learning points.
-
▶
A high index of suspicion is required to make the diagnosis of volvulus of the gallbladder, especially in older patients presenting with RUQ pain.
-
▶
Both clinicians and radiologists should consider it as a differential for patients presenting with signs suggestive of biliary pathology and no demonstrable gallstones on imaging.
-
▶
Investigations and treatment should be instigated early to prevent perforation or sepsis and reduce the mortality of the condition.
-
▶
During an emergency laparotomy, a thorough inspection should always be carried out despite obvious pathology.
Footnotes
Competing interests None.
Patient consent Obtained.
References
- 1.Levene A. Acute torsion of the gallbladder: postmortem findings in two cases. Br J Surg 1958;45:338–40 [DOI] [PubMed] [Google Scholar]
- 2.Sleiber AC, Bauer IJ. Volvulus of the gallbladder. Am J Gaslroenlerol 1983:78:96–8 [PubMed] [Google Scholar]
- 3.Nakao A, Matsuda T, Funabiki S, et al. Gallbladder torsion: case report and review of 245 cases reported in the Japanese literature. J Hepatobiliary Pancreatic Surg 1999;6:418–21 [DOI] [PubMed] [Google Scholar]
- 4.Katz DS, Yam B, Hines JJ, et al. Uncommon and unusual gastrointestinal causes of acute abdomen: CT diagnosis. Semin ultrasound CT MR 2008;29:386–98 [DOI] [PubMed] [Google Scholar]