

Abstract
Duplication of appendix is extremely rare anomaly. The reported incidence is 0.004–0.009%. In most of the cases the finding is accidental. Here the authors are presenting a case of type A duplex appendix in a 25-year male patient.
Background
Rare entity.
Case presentation
A 25-year-old male was admitted in emergency with 2-day history of sudden onset severe pain abdomen, vomiting and fever. Local examination showed tenderness in right iliac region. Blood investigation revealed raised total leucocytes count and neutrophilia. Ultrasonography abdomen showed a blind-ended aperistaltic tubular structure with dilated lumen and thickened wall. No appendiceal anomaly was noticed. A diagnosis of acute appendicitis was made. Appendectomy was performed, and tissue was submitted for histopathological examination. Gross examination showed duplication of whole appendix (figure 1A,B). Serosal surface was dull and focally congested also the lumen was obstructed. Microscopic examination of both appendices showed mucosal ulceration, and lumen was filled with fibrinous material and inflammatory cells (figure 2). Neutrophilic infiltrate was also seen.
Figure 1.

(A) Gross photograph showing duplication of appendix. (B) Gross photograph showing cut section of both appendices.
Figure 2.
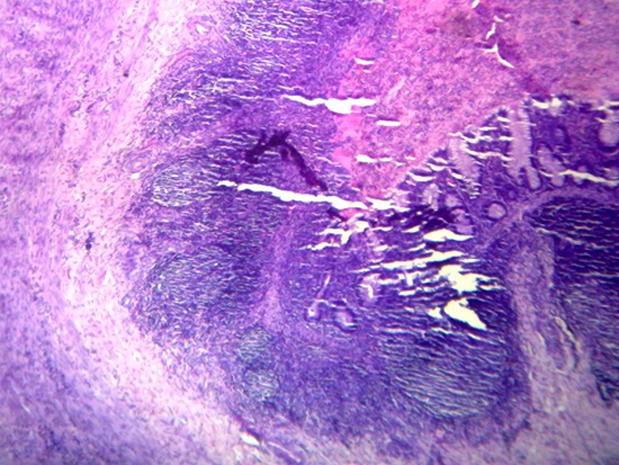
Section showing marked mucosal damage and lumen was filled with fibrinous material and inflammatory cells.
Outcome and follow-up
Patient was discharged in good conditions.
Discussion
Acute appendicitis is one of the most common causes of acute abdomen commonly seen in adolescents. Patients usually present with severe pain in right iliac region, fever and vomiting. Anomalies of appendix are rare and duplication of vermiform appendix is extremely rare. Collins1 studied 50 000 appendectomy specimens and found appendiceal duplication in two cases (0.0004%); however, Kjossev and Losanoff2 got one case in 10 956 specimens (0.009%). Less than 100 cases of appendiceal duplication have been reported in literature till now.2 3 In 1936, Cave4 classified appendiceal duplication for the first time which was modified by Wallbridge in 19635 into three types. Type A consists of various degrees of partial duplication on a normally localised appendix with a single caecum. Type B consists of a single caecum with two completely separate appendices, divided into two further subgroups, type B1 where two appendices are located symmetrically on either side of the ileocaecal valve, resembling the normal arrangement in birds and termed ‘bird-like type’ and type B2 which has a normally located appendix arising from the caecum at the usual site and a second separate rudimentary appendix located along the line of one of the taenia and as such termed ‘taenia-coli type’. Type C consists of a duplicated caecum each with an appendix. However, few cases have been reported that do not fit in Wallbridge classification such as the horse shoe appendix6 7 and triple appendix.8 Our case is consistent with type A variety as both the appendices arose from a common base. Most of the cases were diagnosed accidentally during operation2 9 as in our case; however, in one reported case preoperative diagnosis was made by routine barium examination for other reason.10 These anomalies have clinical and medicolegal significance as Maizels11 described a case in which appendectomy was done twice in 5 months duration in a child. Bluett et al12 reported a case of appendiceal duplication in which barium enema showed a 3–4 cm constriction between caecum and ascending colon which was due to inflammation and mass effect of appendix, and this constriction mimics like colonic carcinoma.
Learning points.
-
▶
Anatomical appendiceal anomalies are rare.
-
▶
They have clinical and medicolegal significance.
-
▶
Preoperative diagnosis is rare.
Footnotes
Competing interests None.
Patient consent Obtained.
References
- 1.Collins DC. A study of 50,000 specimens of the human vermiform appendix. Surg Gynecol Obstet 1955;101:437–45 [PubMed] [Google Scholar]
- 2.Kjossev KT, Losanoff JE. Duplicated vermiform appendix. Br J Surg 1996;83:1259. [PubMed] [Google Scholar]
- 3.Kim EP, McClenathan JH. Unusual duplication of appendix and cecum: extension of the Cave-Wallbridge classification. J Pediatr Surg 2001;36:E18. [DOI] [PubMed] [Google Scholar]
- 4.Cave AJ. Appendix Vermiformis Duplex. J Anat 1936;70:283–92 [PMC free article] [PubMed] [Google Scholar]
- 5.Wallbridge PH. Double appendix. Br J Surg 1962;50:346–7 [DOI] [PubMed] [Google Scholar]
- 6.DasGupta R, Reber PU, Patel AG. Horseshoe appendicitis. Eur J Surg 1999;165:1095–6 [DOI] [PubMed] [Google Scholar]
- 7.Mesko TW, Lugo R, Breitholtz T. Horseshoe anomaly of the appendix: a previously undescribed entity. Surgery 1989;106:563–6 [PubMed] [Google Scholar]
- 8.Tinckler LF. Triple appendix vermiformis – a unique case. Br J Surg 1968;55:79–81 [DOI] [PubMed] [Google Scholar]
- 9.Sobhian B, Mostegel M, Kunc C, et al. [Appendix vermiformis duplex–a rare surprise]. Wien Klin Wochenschr 2005;117:492–4 [DOI] [PubMed] [Google Scholar]
- 10.Peddu P, Sidhu PS. Appearance of a type B duplex appendix on barium enema. Br J Radiol 2004;77:248–9 [DOI] [PubMed] [Google Scholar]
- 11.Maizels G. Duplication of the vermiform appendix. S Afr Med J 1966;40:1123–5 [PubMed] [Google Scholar]
- 12.Bluett MK, Halter SA, Salhany KE, et al. Duplication of the appendix mimicking adenocarcinoma of the colon. Arch Surg 1987;122:817–20 [DOI] [PubMed] [Google Scholar]