

Abstract
Squamous cell carcinoma (SCC) of urinary tract is a very rare tumour known to be associated with chronic renal calculi and infection. This tumour is highly aggressive and often detected at advanced stage with poor outcome. The authors describe a case report of a 62-year-old male patient who was diagnosed with right nephrolithiasis with non-functioning kidney. Histopathology revealed an unexpected co-existing SCC in renal pelvis. The present case highlights the careful search and use of newer imaging modalities in cases of long-standing renal calculi as they may have co-existing hidden malignancy which may change the treatment plan and prognosis.
Background
Primary neoplasms of the renal collecting system are uncommon accounting for only 4–5% of all urothelial tumours.1 2 Transitional cell type is most frequently diagnosed (85–95%) followed by squamous cell carcinoma (SCC) (6–15%) and adenocarcinoma (7%).3 4 The prognosis for SCC is poor, but stage-to-stage prognosis is not different between patients with urothelial carcinoma and SCC. Vascular invasion, microscopic solid tumour pattern and large tumour size have negative prognostic significance. New treatment modalities are urgently needed for early detection of tumour, and aggressive treatment with surgery followed by adjuvant chemotherapy is needed to improve the prognosis.
Case presentation
A 62-year-old male presented with intermittent colicky pain at the right lumbar region for 6 months. He had a mass in the right lumber region for 3 months along with a history of intermittent fever with chills and rigors. On medication, the patient was relieved of fever. On examination, the patient was pale, his vitals were stable. A ballotable lump of 10×10 cm was palpable in the lumber region. It was tender on deep palpation, overlying skin was normal and renal angle was full.
Investigations
His complete blood counts, erythrocyte sedimentation rate, biochemical investigations and urine analysis were within normal range except for low haemoglobin levels. Intravenous pyelography revealed a non-excretory kidney with a radiopaque shadow in the right lumber region. Ultrasonography revealed grossly enlarged right kidney measuring 16 cm with multiple pockets of thick collections and multiple calculi, largest measuring 2.8 cm at lower pole and renal pelvis (figure 1).
Figure 1.

Intravenous pyelogram showing right non-functioning kidney with calculus.
Differential diagnosis
On the basis of above findings, he was diagnosed with right pyonephrosis with nephrolithiasis. No other differential diagnosis was kept.
Treatment
The patient was planned for nephrectomy under general anaesthesia. Nephrectomy was attempted but could not be done due to thick adhesions surrounding grossly enlarged kidney and poor general condition of the patient. Therefore, pyelolithotomy with removal of stone and drainage of pus was offered to provide symptomatic relief. Preoperatively, a biopsy was also performed from a suspicious thick area of renal pelvis surrounding the stone and was sent for histopathology. Histopathology revealed well-differentiated SCC with keratin pearls involving the renal parenchyma (figures 2 and 3).
Figure 2.
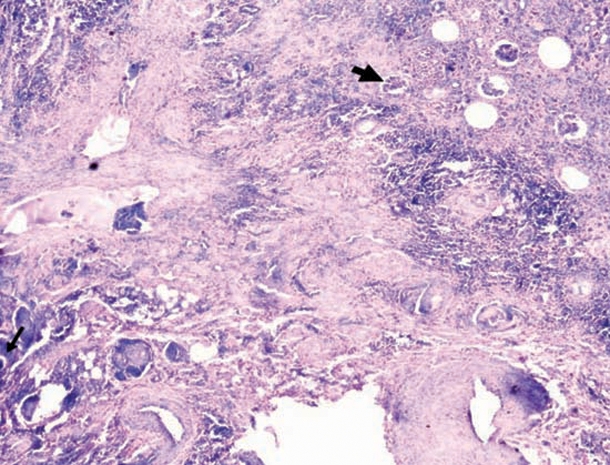
Microphotograph (magnification 10×) showing squamous cell carcinoma (thin arrow) invading glomeruli and interstitium (thick arrow).
Figure 3.
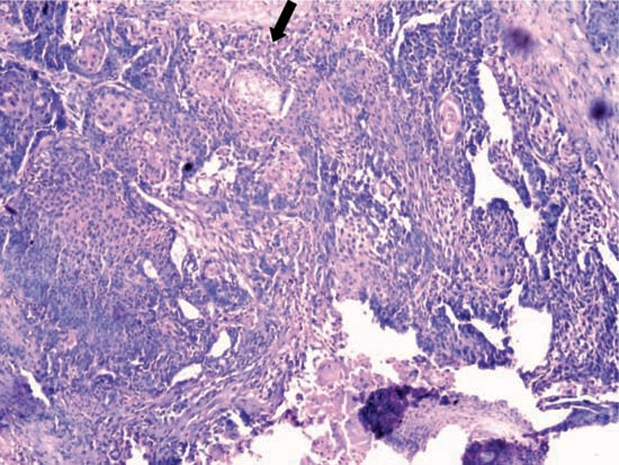
Microphotograph (magnification 40×) showing squamous cell carcinoma with keratin pearls (shown by an arrow).
Outcome and follow-up
Postoperative recovery was uneventful and patient was relieved of symptoms. The patient received three cycles of chemotherapy and was then lost from follow-up.
Discussion
Primary neoplasms of the renal collecting system are uncommon and most of them are malignant. Majority of these cases comprise of transitional cell carcinoma. Pure SCC is very rare, though it is the second most common tumour in the renal pelvis.5 Only 350 cases have been described in literature.6 SCC is often associated with renal calculi or infection, and it usually presents at an advanced stage with pain or palpable mass.7 The incidence of co-existing urinary stone disease varies from 18% in USA to 100% in Hong Kong.7 8 The relevant medical history of SCC often includes episodes of chronic pyelonephritis or nephrolithiasis. Urinary calculi are accepted as a main carcinogenic factor for SCC. Chronic irritation and infection are believed to induce reactive changes in the urothelium and lead to neoplasia via metaplasia and leukoplakia. Staghorn stones are more likely to be associated with renal pelvis neoplasms. Ureteral obstruction is the main cause of presenting symptoms. Diagnosis is difficult because imaging techniques usually reveal only calculi and hydronephrosis due to obstruction. Therefore, the initial diagnosis of SCC is mostly based on the histological analysis as was in our case.
Some authors reported that the treatment of choice is nephrectomy with total ureterectomy including a bladder cuff around the ureteral orifice.9 However, others suggested nephrectomy and only partial ureterectomy.10 Chemotherapy conveys little benefit and the value of radiotherapy is debatable. SCC of upper urinary tract is generally considered as an aggressive tumour. Studies have reported that the average survival time is less than 12 months and most patients die within 2 years after diagnosis.
Learning points.
-
▶
SCC of kidney is an uncommon tumour with poor prognosis and is often associated with renal calculi, infection and chronic pyelonephritis.
-
▶
The initial diagnosis of SCC of kidney is difficult because imaging techniques usually reveal only calculi and hydronephrosis due to obstruction.
-
▶
Patients with of long-standing renal stones should be carefully examined with newer imaging modalities like contrast enhanced CT or MRI for early detection of co-existing SCC and need aggressive treatment to improve the prognosis.
Acknowledgments
Dr Ritesh Kamal is thanked for his co-operation in preparing the manuscript.
Footnotes
Competing interests None.
Patient consent Obtained.
References
- 1.Murphy DM, Zincke H, Furlow WL. Primary grade 1 transitional cell carcinoma of the renal pelvis and ureter. J Urol 1980;123:629–31 [DOI] [PubMed] [Google Scholar]
- 2.Murphy DM, Zincke H, Furlow WL. Management of high grade transitional cell cancer of the upper urinary tract. J Urol 1981;125:25–9 [DOI] [PubMed] [Google Scholar]
- 3.Latham HS, Kay S. Malignant tumors of the renal pelvis. Surg Gynaecol Obstet 1974;138:613–22 [Google Scholar]
- 4.Utz DC, McDonald JR. Squamous cell carcinoma of the kidney. J Urol 1957;78:540–52 [DOI] [PubMed] [Google Scholar]
- 5.Kandemir O, Tatlisen A, Kontas O, et al. Sarcomatoid squamous cell carcinoma of the right renal pelvis with liver metastasis: case report. J Urol 1995;153:1895–6 [PubMed] [Google Scholar]
- 6.Nativ O, Reiman HM, Lieber MM, et al. Treatment of primary squamous cell carcinoma of the upper urinary tract. Cancer 1991;68:2575–8 [DOI] [PubMed] [Google Scholar]
- 7.Li MK, Cheung WL. Squamous cell carcinoma of the renal pelvis. J Urol 1987;138:269–71 [DOI] [PubMed] [Google Scholar]
- 8.Blacher EJ, Johnson DE, Abdul-Karim FW, et al. Squamous cell carcinoma of renal pelvis. Urology 1985;25:124–6 [DOI] [PubMed] [Google Scholar]
- 9.Dutkiewicz S, Kalczak M. Planoepithelial squamous cell carcinoma of the renal pelvis. Int Urol Nephrol 1994;26:631–5 [DOI] [PubMed] [Google Scholar]
- 10.Mhiri MN, Rebai T, Turki L, et al. Association between squamous cell carcinoma of the renal pelvis and calculi. Br J Urol 1989;64:201–2 [DOI] [PubMed] [Google Scholar]