

Abstract
BACKGROUND:
Despite the high prevalence and morbidity, tinnitus still remains an obscure symptom. We assessed the efficacy of low-level laser for treatment of tinnitus.
METHODS:
It was a self controlled clinical trial study on 61 outpatients with subjective tinnitus. The patients were irradiated with a 650-nm, 5-mW soft laser for twenty days and twenty minutes per day. The sensation of tinnitus was measured on a Visual Analog Scale (VAS) before and two weeks after treatment and they were compared by means of Wilcoxon signed ranktest.
RESULTS:
Thirty-eight (62.3%) patients were men and twenty-three (37.7%) were women. Fourteen patients (31.8%) worked in noisy environment. The VAS mean difference before and after the treatment was statistically significant (p < 0.0001). The best treatment effect was in the youngest group and there were significant differences between this group and the middle age and older groups (p = 0.018 and 0.001, respectively). The mean VAS score reduction was not statistically significant between male and female patients (p = 0.23). Also, the treatment outcome according to the noise level in patient's workplaces was not significantly different in women (p = 0.693), but it was significant in men (p = 0.029).
CONCLUSIONS:
Transmeatal low-level laser irradiation is effective for the treatment of tinnitus and some variables like age and job can affect the treatment outcome.
Keywords: Tinnitus, Laser Therapy, Low-Level, Workplace
Tinnitus is a perception of sounds without external source. Approximately 14% of the adult population persistently suffers from tinnitus, and 20% of those with such symptoms experience considerable distress.1 Despite its prevalence and morbidity, tinnitus still remains an obscure symptom. Mainly because of the subjective nature of the disorder and our lack of knowledge of its pathophysiology, treatment of tinnitus has been limited, controversial, and quite often unsuccessful. Pharmacological treatment of tinnitus in particular, has proved to be a difficult task, although the effect on tinnitus of many substances has been studied and some used to alleviate tinnitus. However, there are presently no agents specifically recommended for this purpose. Commonly prescribed drugs for tinnitus include sedatives, anticonvulsants, antidepressants, local anesthetics, antihistamines, antipsychotics, and botulinum toxin A, all providing mixed or inconsistent benefits.2 Non-pharmacologic and surgical therapeutic approaches have been used in selected cases. These methods have not shown dramatic therapeutic effects.3 Other modalities that have been proposed for treatment of tinnitus are: antioxidant therapy,4 trans coetaneous electrical stimulation,5 Tinnitus Retraining Therapy (TRT),6 repetitive transcranial magnetic stimulation (rTMS),7 sound therapy,8 and cognitive-behavioral therapy.9 In addition to different standard methods, transmeatal cochlear low-level laser irradiation (TCL) has been introduced as an alternative modality for cochlear dysfunction such as chronic cochlear tinnitus.
The therapeutic mechanism of this method is not completely understood. Some theories proposed that it may be because of increasing in cell proliferation, ATP and collagen production, secretion of growth factors, improving the inner ear blood flow and activating the haircell mitochondria that stimulates repair mechanisms.10 During the last decade, different studies have been conducted for assessing the efficacy of this modality and because of diverse results there is no consensus about it. Meaningful relief of tinnitus intensity has been shown in a range of 15% of patients, up to 67% of patients, however in some other studies the reduction of tinnitus by laser irradiation was not significant.11
The aim of the present study was to evaluate the effectiveness of low-power laser on the treatment of tinnitus in the patients and determine if differences in some variables like age, gender or job, can affect the effectiveness of the treatment.
Methods
This is a self-controlled clinical trial with premeasures and postmeasures. The study included 61 patients, suffering from monolateral or bilateral noise-like tinnitus more than 6 months prior to entry, with no concomitant treatments for tinnitus. Previous pharmacological treatment did not have any effect on tinnitus and patients had quitted treatment at least one month before laser therapy. Complete audiological, and ENT examinations were performed to rule out treatable causes of tinnitus. The sampling method was convenient sampling and the patients were recruited through the Central Clinic of Isfahan, in 2009. Before any study procedure, written informed consent was provided by each patient and the Ethics Committee of the Medical University of Isfahan approved the study protocol.
Inclusion criteria were an age of at least 15 years and a document diagnosis of chronic subjective tinnitus (monolateral or bilateral). Exclusion criteria were conductive hearing loss, tympanic membrane perforation, any ear discharge, and a history of ear surgery.
Patients were asked to complete a questionnaire that consisted of demographic data.
The name of laser irradiation source was TINNImed. The TINNImed is a 5mw medical soft laser transmitter connected by a fiberoptic cable and an adapter with a soft silicone tip to the ear. The laser beam is then directed through the tympanic membrane into the cochlea.
The silicone part of the device was located in the external auditory meatus of the ear with more severe tinnitus (in patients with bilateral tinnitus) and patients were irradiated according to a defined treatment protocol. In the active laser, the output was 5 mW, and the wave-length was 650 nm. Each patient was irradiated twenty times for twenty consecutive days and the duration of irradiation was 20 minutes a day. Continuous beam were applied for patients and it was fixed toward the external meatus only. The primary outcome variable was the sensation of tinnitus that was measured on a Visual Analog Scale. The VAS consisted of 100-mm lines with extremes that indicated the words “total absence” and “maximum” of tinnitus loudness. The pretherapeutic degree of tinnitus was defined on the VAS for each patient (baseline).
All patients underwent audiometric assessment, VAS, and microscopic examination of the external auditory meatus and tympanic membrane before and two weeks after laser treatment. We asked all patients to describe any side effects during and after the treatment.
We estimated that recruitment of 51 patients would provide 90% power to find a meaningful difference between the effects of treatment on tinnitus intensity at a significance of p < 0.05. For calculating the sample size, one of the previous studies was used.12 As we anticipated a dropout rate of 20%, the sample size was increased to 61 subjects. Normal distribution of VAS data was assessed with the Kolmogrov-Smirov and it was not normal. All data were descriptively analyzed.
We calculated the difference between two measures of tinnitus severity for each patient and converted it to a percent value. We categorized patients according to age and job and we assessed the treatment effect in these sub-groups. Age categories were group 1 (18-30 years), group 2 (31-50 years), and group3 (> 50 years). In addition, we divided patients according to the noise level in their workplaces into high (patients who worked in some industrial factories with high level noise in their work-places) and low level noise workplace.
The effect of laser therapy on the treatment outcome scores were assessed by means of the nonparametric Wilcoxon signed ranktest. For assessment of the outcome in patient's sub-groups, according to job and age categories, ANOVA (analysis of variance) was used and for comparison of the treatment effect between male and female participants, t-test was used. Missing data were replaced with the last observation values. Statistical analyses were performed using the SPSS (ver. 18.0), and the level of significance was defined at α = 0.05 (2-tailed).
Results
Treatment was well tolerated in all participants and adverse or side effect was not observed. All sixty-one patients completed the treatment and were included in the analysis. The mean age of the subjects was 40.5 ± 15.3 years (range: 18-80). Thirty-eight (62.3%) patients were men and twenty-three (37.7%) were women. Fourteen patients (31.8%) worked in noisy environments and the others did not. VAS scores were calculated pre- and post-treatment and the mean of tinnitus severity before treatment was 82.3 ± 18.3 percent (range: 40-100%). Because VAS distribution was not normal, non-parametric Wilcoxon signed rank-test was used. The mean difference was 35.9% ± 38.7% and was statistically significant (p < 0.0001). In eleven patients (seven men and four women) tinnitus was completely disappeared, as the VAS reduction was seen in thirty patients and twenty patients did not report any relief. None of the patients reported that the tinnitus severity has increased.
When the outcome in different age categories by means of one- way ANOVA was assessed, Post hoc tests revealed that the best treatment effect was in the youngest group and the differences between this group and the other two groups were statistically significant (Table 1). The mean VAS score reduction in male patients was 31.3% and in female patients was 43.6%, but this difference was not statisti-cally significant (p = 0.23), but when we compared the treatment effect in two sexes, according to their age categories by means of univariate analysis, the difference between male and female patients was significant in the third group (p < 0.0001) (Figure 1).
Table 1.
The comparison of treatment effect in different age categories
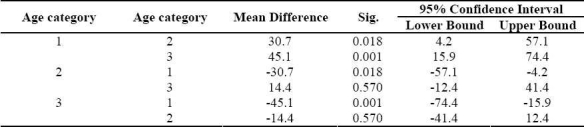
Figure 1.
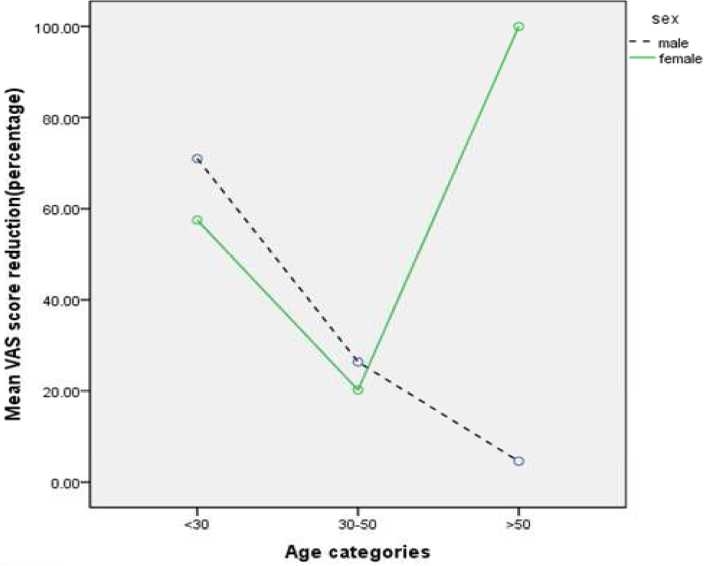
Mean VAS score reduction in three age categories accordcing to sex
We calculated the treatment outcome according to the noise level in patient's work-places (Figure 2). The difference was not statistically significant in women (p = 0.693), but it was significant in men (p = 0.029).
Figure 2.
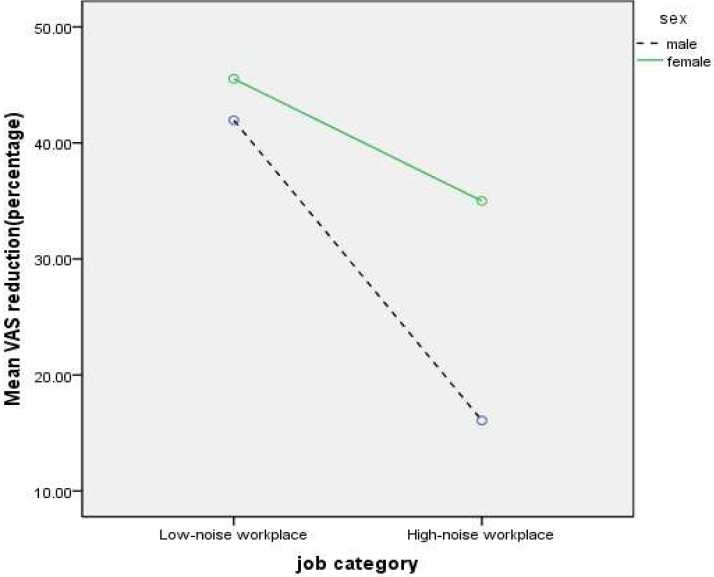
Mean VAS score reduction in two job categories according to sex
Discussion
Low-level laser therapy (LLLT) as a therapeutic morality in cochlear dysfunction such as chronic cochlear tinnitus or sensorineural hearing loss is still controversial. Low-intensity laser irradiation is a new and effective method for the treatment of peripheral and central nervous system injuries and disorders.11 In addition to different pathophysiological mechanisms of inner ear diseases and diverse theories on the nature of tinnitus, the methodical differences in study design, treatment schedules and irradiation parameters could cause wide range of outcomes.11
The present study for treatment of tinnitus resulted in subjectively mentioned tinnitus reduction in 30 (49.1%) patients, tinnitus disappearance in eleven (18%), and without change in twenty (32.7%) patients two weeks after completion of therapy. The mean reduction of tinnitus intensity was 35.9%. Generally these results are in concordance with therapeutic outcomes of the previous studies that have shown the range of tinnitus relief between 37% and 58%.11–13 In contrast, some of previous trials failed to show clear benefits of low-level laser for patients suffering from chronic tinnitus.12,14,15
In general, the present study shows the best treatment outcome in younger patients and it may be because of higher prevalence of some conditions like presbycusis or chochlear dysfunction in older age groups. This finding was not similar in men and women and it is probably because of small sample size in some sub-groups. In addition, our trial suggests that noise level in workplace can affect the treatment outcome too, but further investigations are needed to confirm this finding.
Current study evaluated the tinnitus intensity only by means of VAS and it was measured once two weeks after laser therapy. We did not follow patients to assess if the treatment effect remains changeless.
Because tinnitus sensation is a subjective phenomenon, it seems that the study design is acceptable. However, self-controlled clinical trials such as the present one have some limitations. Part of observed treatment effect may be due to the phenomenon of “regression toward the mean” and also there is some degree of “Hawthorne effect” in uncontrolled trials. These problems can be solved only by performing a comparative study, while the use of a randomized control group is the best method for distinguishing between any real reduction in tinnitus intensity and the effect of those biases.
Conclusions
In conclusion, low-level laser therapy can offer significant benefit in treatment of tinnitus. In addition, we assessed the treatment effect in different gender, job, and age categories. Further experimental studies specially randomized controlled trials are needed to assess the effect of these factors on the treatment efficacy.
Conflict of Interests
Authors have no conflict of interests.
Authors’ Contributions
HA, NB, AO and HO carried out the design and coordinated the study, participated in most of the experiments and prepared some parts of the manuscript. AM provided assistance in the design and analysis of the study, and participated in manuscript preparation. All authors have read and approved the content of the manuscript.
Acknowledgments
We are grateful to the Isfahan University of Medical Sciences for financial support (Grant No. 388469). We also express our gratitude to Mr. Ali Hosseini for his help with the laser therapy of patients.
References
- 1.Malouff JM, Noble W, Schutte NS, Bhullar N. The effectiveness of bibliotherapy in alleviating tinnitus-related distress. J Psychosom Res. 2010;68(3):245–51. doi: 10.1016/j.jpsychores.2009.07.023. [DOI] [PubMed] [Google Scholar]
- 2.Enrico P, Sirca D, Mereu M. Antioxidants, minerals, vitamins, and herbal remedies in tinnitus therapy. In: Moller A, Langguth B, Hajak G, Kleinjung T, Cacace A, editors. Tinnitus: pathophysiology and treatment. Amsterdam: Elsevier; 2007. pp. 323–30. (Progress in brain research; vol 166) [DOI] [PubMed] [Google Scholar]
- 3.Jalali MM, Kousha A, Naghavi SE, Soleimani R, Banan R. The effects of alprazolam on tinnitus: a cross-over randomized clinical trial. Med Sci Monit. 2009 Nov 15;15(11):PI55–60. [PubMed] [Google Scholar]
- 4.Savastano M, Brescia G, Marioni G. Antioxidant therapy in idiopathic tinnitus: preliminary outcomes. Arch Med Res. 2007;38(4):456–9. doi: 10.1016/j.arcmed.2006.12.004. [DOI] [PubMed] [Google Scholar]
- 5.Kapkin O, Satar B, Yetiser S. Transcutaneous electrical stimulation of subjective tinnitus.A placebo-controlled, randomized and comparative analysis. ORL J Otorhinolaryngol Relat Spec. 2008;70(3):156–61. doi: 10.1159/000124288. [DOI] [PubMed] [Google Scholar]
- 6.Brehmer D, Overhoff HM. The initial results of the effectiveness of outpatient tinnitus retraining therapy--a multi-centric study. Int Congr Ser. 2003;1240:221–3. [Google Scholar]
- 7.Langguth B, Kleinjung T, Landgrebe M, de Ridder D, Hajak G. rTMS for the treatment of tinnitus: the role of neu-ronavigation for coil positioning. Neurophysiol Clin. 2010;40(1):45–58. doi: 10.1016/j.neucli.2009.03.001. [DOI] [PubMed] [Google Scholar]
- 8.Jastreboff MM. Sound therapies for tinnitus management. In: Moller A, Langguth B, Hajak G, Kleinjung T, Cacace A, editors. Tinnitus: pathophysiology and treatment. Amsterdam: Elsevier; 2007. pp. 435–40. Progress in brain research; vol 166. [Google Scholar]
- 9.Andersson G. Psychological aspects of tinnitus and the application of cognitive-behavioral therapy. Clin Psychol Rev. 2002;22(7):977–90. doi: 10.1016/s0272-7358(01)00124-6. [DOI] [PubMed] [Google Scholar]
- 10.Siedentopf CM, Ischebeck A, Haala IA, Mottaghy FM, Schikora D, Verius M, et al. Neural correlates of transmeatal cochlear laser (TCL) stimulation in healthy human subjects. Neurosci Lett. 2007;411(3):189–93. doi: 10.1016/j.neulet.2006.08.049. [DOI] [PubMed] [Google Scholar]
- 11.Tauber S, Schorn K, Beyer W, Baumgartner R. Transmeatal cochlear laser (TCL) treatment of cochlear dysfunction: a feasibility study for chronic tinnitus. Lasers Med Sci. 2003;18(3):154–61. doi: 10.1007/s10103-003-0274-6. [DOI] [PubMed] [Google Scholar]
- 12.Nakashima T, Ueda H, Misawa H, Suzuki T, Tominaga M, Ito A, et al. Transmeatal low-power laser irradiation for tinnitus. Oto Neurotol. 2002;23(3):296–300. doi: 10.1097/00129492-200205000-00011. [DOI] [PubMed] [Google Scholar]
- 13.Shiomi Y, Takahashi H, Honjo I, Kojima H, Naito Y, Fujiki N. Efficacy of transmeatal low power laser irradiation on tinnitus: a preliminary report. Auris Nasus Larynx. 1997;24(1):39–42. doi: 10.1016/S0385-8146(96)00003-X. [DOI] [PubMed] [Google Scholar]
- 14.Partheniadis-Stumpf M, Maurer J, Mann W. Soft laser therapy in combination with tebonin i.v. in tinnitus. Laryngorhinootologie. 1993;72(1):28–31. doi: 10.1055/s-2007-997848. (German) [DOI] [PubMed] [Google Scholar]
- 15.Teggi R, Bellini C, Piccioni L, Palonta F, Bussi M. Transmeatal low-level laser therapy for chronic tinnitus with cochlear dysfunction. Audiol Neurotol. 2009;14(2):115–20. doi: 10.1159/000161235. [DOI] [PubMed] [Google Scholar]