

Cardiovascular disease remains the leading cause of death in women. Both obesity and diabetes mellitus are important independent risk factors for the development of cardiovascular disease. Obesity is the leading risk factor for type 2 diabetes. The Centers for Disease Control and Prevention report that 32% of white and 53% of black women are obese. Women with a body mass index (BMI) of 30 kg/m2 have a 28 times greater risk of developing diabetes than do women of normal weight. The risk of diabetes is 93 times greater if the BMI is 35 kg/m2.1 The presence of diabetes can increase a woman's risk of heart disease 2-fold. In addition, the presence of diabetes overshadows the protective effects of the premenopausal state. In 2007, 11.5 million of all women over the age of 20 (10.2%) had diabetes, and rates were slightly higher in ethnic minority groups: 10.4% in Hispanic women and 11.8% in non-Hispanic black women.2 The national prevalence rates of diabetes have increased in parallel with the rates of obesity (Fig. 1).
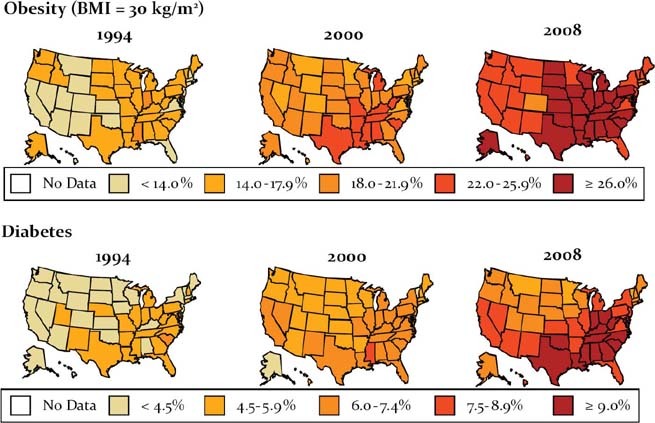
Fig. 1 Age-adjusted percentage of U.S. adults who were obese or who had a diagnosis of diabetes mellitus.
BMI = body mass index
Screening
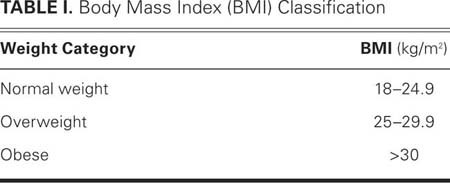
Screening for obesity and diabetes is the 1st step to treatment and often reveals individuals who are at risk for but do not yet have overt disease. The United States Preventive Services Task Force (USPSTF) recommends that all adults be screened for obesity. Obesity signifies excess adipose tissue. The most widely used method for screening is determination of the BMI. The BMI is weight in kilograms divided by height in meters squared (BMI = kg/m2) (Table I). Most electronic medical records automatically calculate BMI if height and weight are entered. There are also many smart-phone applications and online calculators that can calculate BMI (for example, http://www.nhlbisupport.com/bmi). Other screening tools include waist circumference and the waist-to-hip ratio. In women, a waist circumference >35 in (88 cm) or a waist-to-hip ratio >0.7 indicates excess visceral fat and increased risk for disease.
TABLE I. Body Mass Index (BMI) Classification
Recommendations for screening for diabetes vary by guideline author. The USPSTF recommends screening asymptomatic patients who have blood pressures >135/80 mmHg. The American Diabetes Association (ADA) recommends that individuals who are ≥18 years of age and have a BMI ≥25 kg/m2 and 1 additional risk factor for diabetes should be screened annually (Table II).3 Individuals over the age of 45 without risk factors should be screened every 3 years. In January 2010, the ADA released new recommendations for the use of hemoglobin A1C as a screening tool. An A1C greater than 6.5% indicates diabetes. In addition, the results of screening tests for diabetes can identify individuals with “prediabetes” who have a markedly increased risk of developing overt disease.3
TABLE II. American Diabetes Association Recommendations on Screening for Type 2 Diabetes3

Non-Pharmaceutical Treatment
Lifestyle-treatment options for diabetes mellitus and excess weight are similar, and 2 recent studies4,5 have demonstrated the critical components for treating pre-diabetes and diabetes through weight loss, using caloric restriction and physical activity. The 1st study was the Diabetes Prevention Program.4 The purpose of the study was to identify individuals who were at risk for developing diabetes because of elevated fasting plasma glucose or impaired glucose tolerance levels that were not yet in the diagnostic range, in order to determine if metformin or an intensive lifestyle intervention could delay or prevent the onset of diabetes. More than 3,000 individuals with prediabetes were randomized to receive placebo, metformin, or a 16-session lifestyle-modification program. The intensive lifestyle program set a goal of 7% weight loss and 150 min/wk of moderate physical activity. Fifty percent of the lifestyle-intervention group lost 7% of their body weight. The 3-year incidence of diabetes in the metformin group was 31% lower than that in the placebo group. The incidence was 58% lower in the lifestyle group than in the placebo group.4 The clinical implications of this study are that we should 1) identify individuals with pre-diabetes and 2) recommend lifestyle modifications that result in a 7% weight loss and include 150 min/wk of moderate physical activity.
The 2nd study that examined lifestyle treatment of diabetes and obesity is the Look AHEAD Trial. The purpose of the study was to determine the effect of intentional weight loss on cardiovascular risk factors in individuals with diabetes. Approximately 5,100 individuals with type 2 diabetes and an elevated BMI were randomized. Study conditions specified a 36-session intensive lifestyle intervention with the option of using partial meal replacements for caloric restriction or 4 sessions of standard diabetes support and education (DSE). At 1 year, 55% of the intensive-lifestyle-intervention group achieved 7% weight loss. Hemoglobin A1C, systolic and diastolic blood pressure, and lipids improved significantly more in the intensive-lifestyle group than in the DSE group.5 The clinical implication of this study is that intentional weight loss of at least 7% can improve the cardiovascular risk profile of patients with type 2 diabetes.
Conclusions
Excess weight affects two thirds of the U.S. adult population and increases risk for cardiovascular disease and diabetes. All patients should be screened for obesity and most should be screened for pre-diabetes and diabetes. The best treatment for diabetes is prevention. Prevention of diabetes can be accomplished through a 7% weight loss through intensive lifestyle interventions that include caloric reduction and approximately 30 min of daily moderate physical activity. Practitioners will have access to these evidence-based programs soon. The Centers for Disease Control and Prevention are promoting community-based diabetes prevention programs throughout the country.
Footnotes
Address for reprints: Ann Smith Barnes, MD, MPH, Department of Medicine, Baylor College of Medicine, One Baylor Plaza, MS 285, Houston, TX 77030. E-mail: smith@bcm.edu
Presented at the Risk, Diagnosis and Treatment of Cardiovascular Disease in Women symposium; Denton A. Cooley Auditorium, Texas Heart Institute, Houston; 11 September 2010.
References
- 1.Colditz GA, Willett WC, Rotnitzky A, Manson JE. Weight gain as a risk factor for clinical diabetes mellitus in women. Ann Intern Med 1995;122(7):481–6. [DOI] [PubMed]
- 2.U.S. Department of Health and Human Services Centers for Disease Control and Prevention. National diabetes fact sheet, 2007 [2010 Mar 12; cited 2011 Feb 1]. Available from: http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2007.pdf.
- 3.American Diabetes Association. Standards of medical care in diabetes–2010. Diabetes Care 2010;33 Suppl 1:S11–61. [DOI] [PMC free article] [PubMed]
- 4.Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002;346(6):393–403. [DOI] [PMC free article] [PubMed]
- 5.Look AHEAD Research Group, Pi-Sunyer X, Blackburn G, Brancati FL, Bray GA, Bright R, et al. Reduction in weight and cardiovascular disease risk factors in individuals with type 2 diabetes: one-year results of the look AHEAD trial. Diabetes Care 2007;30(6):1374–83. [DOI] [PMC free article] [PubMed]