

Abstract
Background
Shoulder impingement syndrome is a common upper extremity pathology in manual wheelchair users. Central to impingement is the orientation of the scapula and humerus as they determine the available subacromial space. The purpose of this study was to examine the scapulothoracic and glenohumeral internal/external rotation kinematics during the time of peak shoulder loading of propulsion and weight relief lift conditions to assess possible risk of impingement.
Methods
Scapula, humerus and trunk kinematics were measured for twelve manual wheelchair users over three conditions: level propulsion, ramp propulsion, and a weight relief lift. Scapulothoracic and glenohumeral kinematic variables were characterized for the full cycle of each condition as well as at the period of peak loading.
Findings
Common to all activities was an externally rotated glenohumeral joint and an anteriorly tilted and internally rotated scapula. At peak loading, glenohumeral internal/external rotation showed a significant difference between conditions, and post hoc analysis revealed that the weight relief lift displayed significantly less external rotation at peak loading when compared to level and ramp propulsion.
Interpretation
All activities placed the scapula in a potentially dangerous orientation for development of shoulder impingement. The weight relief lift, with a decrease in glenohumeral external rotation and large superior forces at the shoulder, potentially places the shoulder of the manual wheelchair user at the greatest risk for impingement soft tissue injury. Preventative strength training and activity modification may provide measures to slow progression of impingement development and associated pain in the manual wheelchair user.
Keywords: wheelchair, scapula, kinematics, shoulder, impingement
INTRODUCTION
In the United States (US), approximately 12,000 people suffer from a spinal cord injury each year (National Spinal Cord Injury Statistical Center, 2010). Of the roughly 260,000 people living in the US with a spinal cord injury, many use manual wheelchairs. Manual wheelchair users (MWU) rely on their upper extremities (UE) for mobility, activities of daily living, and vocation performance. With the primary load bearing role shifting from the lower extremities to the smaller musculature of the UE (Requejo and Mulrouy, Spring, 2008), manual wheelchair users are at a high risk for UE pain and pathology limiting not only their ambulation but all areas of function (Bayley et al., 1987, Gellman et al., 1988a, Gellman et al., 1988b, Nichols et al., 1979, Pennes et al., 1983, Pentland and Twomey, 1991). Shoulder impingement syndrome has been reported as the most common UE pathology in MWU (Bayley et al., 1987, Lee and McMahon, 2002) and is described by Neer (Neer, 1972) as a compromise of the space between the humeral head and the acromial arch affecting the soft tissue contained within.
Central to the occurrence of impingement syndrome is the orientation of the scapula and humerus as they determine the available subacromial space. In the non-weight bearing shoulder, certain scapular and glenohumeral orientations have been identified to reduce the subacromial space; and thus, increase the risk of shoulder impingement. Scapular orientations of concern have been reported as an increase in anterior tilting (decrease in posterior tilt), an increase in internal rotation (decrease in external rotation), and a decrease of upward rotation (increase in downward rotation) (Ludewig and Cook, 2000, Lukasiewicz et al., 1999, Solem-Bertoft et al., 1993, Warner et al., 1992). Additionally, increased humeral internal rotation has been reported to contribute to greater deformation of the soft tissue within the subacromial space (Flatow et al., 1994).
Previous investigations into scapular orientation in MWU have been focused on transfers and weight relief lifts (Finley et al., 2005, Nawoczenski et al., 2003, Riek et al., 2008). Common to these studies was the characterization of scapula and humerus orientations during transfers and weight relief lifts that were associated with a decrease in the subacromial space. The rate at which these activities are performed in MWU places the shoulder at a high risk of developing an injury. Finley et al. (Finley et al., 2005) observed that MWU with and without impingement perform transfers with different scapular kinematics, and some of the differences could be attributed to compensatory changes in those with impingement to allow for a maintenance of subacromial space during the tested activity. Riek et al. (Riek et al., 2008) explored a larger variety of activities in MWU and concluded that the standing frame posture resulted in the most favorable scapular and humeral orientations when compared to a sitting rest posture, transfers, weight relief lifts, and standing depression lifts. While many activities have been characterized in terms of MWU shoulder health, propulsion tasks have not been investigated.
Another crucial variable in impingement risk beyond kinematics alone is the loading associated with an activity. The load of an activity performed by MWU can affect the musculature resulting in altered kinematics as well as contributing to a harmful migration of the humeral head into the subacromial space. The high loading and repetitive nature of manual wheelchair activities of daily living and mobility have been reported to result in an increase of scapular protraction on the thoracic wall from the fatigue of the scapular muscles. In protraction, the scapula is translated away from the midline and rotated to conform to the thoracic wall (Lee and McMahon, 2002). This altered scapular location and orientation results in an increase in scapula internal rotation and possible increase in scapula anterior tilting: leading to a decrease of the available subacromial space. While previous studies on scapular kinematics in MWU have focused on traditionally high load activities (transfers and weight relief lifts), loads occurring during the kinematic data collection were not reported. This piece is essential to not only being able to comment on global impingement risk, but specifically the risk in MWU who are utilizing their shoulders in a predominantly load-bearing state. Therefore, the purpose of this investigation was to characterize scapular kinematics during periods of high loading in a spectrum of wheelchair activities: level propulsion, ramp propulsion, and a weight relief lift. We hypothesized that the loading and kinematics associated with weight relief lifts would highlight its potential risk for impingement in comparison to level and ramp propulsion.
METHODS
Subjects
Twelve experienced manual wheelchair users were recruited for study participation (Table 1) (Morrow et al., 2009). Eleven participants were manual wheelchair users secondary to spinal cord injury; one secondary to spina bifida. All participants had normal functioning shoulder musculature. All participants were between 29 and 56 years old (Average age of 43 ± 6.4 years) and had a minimum of one year of experience as a manual wheelchair user (Average 18 ± 9.0 years of experience, range of 1–29 years). Prior to testing all subjects underwent a physical examination by a licensed physical therapist for evaluation of UE strength, pain, and joint stability. Individuals were excluded from study participation if they reported having any upper extremity pain or injury within the past 6 months, or their occupation involved repetitive overhead activities. Additional study exclusion criteria included findings of incomplete/painful upper extremity range of motion or muscle weakness as determined by the physical examination. The study protocol was approved by the Mayo Clinic Institutional Review Board and informed consent was obtained from all research participants before initiating test procedures.
Table 1.
Subject Demographics.
| Subject | Gender | Age (years) | Height (cm) | Weight (kg) | Arm Dominance | Physical Disability | SCI Level | Years as Wheelchair User |
|---|---|---|---|---|---|---|---|---|
| 1 | M | 45 | 178 | 79 | R | SCI | T11 | 24 |
| 2 | F | 42 | 163 | 61 | L | SCI | T12 | 14 |
| 3 | M | 44 | 183 | 86 | R | SCI | T10 | 11 |
| 4 | M | 42 | 175 | 67 | R | SCI | L1 | 16 |
| 5 | M | 45 | 180 | 61 | R | SCI | T10 | 18 |
| 6 | M | 45 | 170 | 80 | L | SCI | T4 | 22 |
| 7 | M | 56 | 170 | 82 | R | SCI | T12 | 22 |
| 8 | M | 46 | 180 | 94 | R | SCI | T5 | 29 |
| 9 | M | 29 | 152 | 61 | R | SB | NA | 29 |
| 10 | M | 42 | 175 | 75 | R | SCI | T10 | 5 |
| 11 | M | 35 | 185 | 136 | R | SCI | L1 | 1 |
| 12 | M | 45 | 183 | 114 | R | SCI | T10 | 26 |
Abbreviations:
M=Male
F=Female
R=Right
L=Left
SCI=Spinal Cord Injury
SB=Spina Bifida
Instrumentation
Kinematic data were recorded at 240 Hz using a 10 camera Real-time Eagle Motion Analysis System (Motion Analysis Corp., Santa Rosa, CA, USA) with a measured accuracy within 1mm and 1º using a standard motion system accuracy device (Piazza et al., 2007). Reflective markers were placed on 7 anatomical landmarks on the subject’s trunk and right humerus to define segment joint centers and segment coordinate systems (Table 2). The scapula anatomical system was defined using population data for three dimensional locations of the ISB recommended landmarks: angulus acromialis, trigonum scapulae, and the angulus inferior (Wu et al., 2005). The population-averaged digitized points were collected on twenty cadaveric scapulae using a Polhemus FASTTRACK system (Polhemus, Colchester, VT, USA) with a previously measured accuracy of digitization within 0.32±0.60 mm (Zhao et al., 2005). The digitized anatomical landmark locations were normalized to body height and referenced to surface markers present on both the cadaveric and in vivo subjects for conversion to a subject-specific anatomical coordinate system. Scapular kinematic tracking and technical coordinate system definition was captured with a custom built scapula tracker that has three reflective markers (Figure 1). The scapula tracker was made of thermo-plastic material that has been formed to rest on the skin overlying the posterior aspect of the scapula along the scapular spine. Two reflective markers were attached to the plastic frame on the medial end and one marker was attached to the lateral end of the tracker above a universal joint metal foot. The lateral foot was placed with double sided tape on the posterior aspect of the acromion, and the tracker body was attached with tape along the scapular spine. A similar scapula tracking device (jig that lies along the scapular spine) has been evaluated using a bone pin technique (Karduna et al., 2001). While the measurement systems differ between the studies, the scapula tracking device on the spine was determined to be accurate to within 3° for the functional range of motion experienced during wheelchair propulsion (Karduna et al., 2001). Marker position data were digitally filtered using a fourth-order, zero-phase, low-pass Butterworth filter with a 6-Hz cutoff frequency. A static, neutral position was collected for development of the local anatomical coordinate system prior to dynamic data collection. Expanded kinematic data and kinetic data were also collected and described previously in Morrow et al. (Morrow et al., 2009).
Table 2.
Segment and Coordinate System (CS) Definitions.
| Segment | Anatomical Landmarks | Tracking Landmarks | Anatomical CS ORIGIN | CS Sign Convention |
|---|---|---|---|---|
| Trunk | Sternum Xiphoid C7 T10 |
Sternum Xiphoid C7 T10 |
Geometric Center between Xiphoid and T10 | Anterior (+X), posterior (-X) Medial (+Y), lateral (-Y) Superior (+Z), inferior (-Z) |
| Upperarm | Acromion process Medial epicondyle Lateral epicondyle |
Acromion process Medial epicondyle Lateral epicondyle |
Shoulder center defined by regression equation by de Leva (1996). | |
| Scapula | Angulus acromialis Trigonum scapulae Angulus inferior |
Lateral tracker marker Superior tracker marker Inferior tracker marker |
Angulus acromialis |
DE LEVA, P. (1996) Joint center longitudinal positions computed from a selected subset of Chandler's data. J Biomech, 29, 1231–3.
Figure 1.
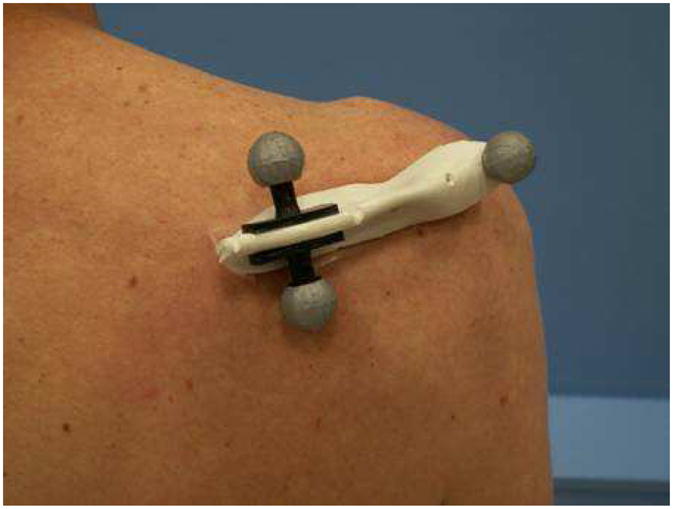
Scapula tracker placement on subject.
Experimental Procedure
Three dynamic conditions were evaluated in the following order: level propulsion, ramp propulsion up a 1:12 incline, and during a weight relief maneuver. The level and ramp propulsion conditions were performed over a distance of 10 m at a self-selected speed. For the weight relief, subjects began at rest, then lifted the weight of their body with their hands on the handrim at a self-selected speed, held the position for 3 seconds, and returned to initial rest position at a self selected speed. Five trials were performed for each condition, and subjects were allowed to rest between trials as needed.
Data Analysis
A three-dimensional model of the right upper extremity was developed using Visual3D (C-Motion Inc., Germantown, MD, USA). The model consisted of three rigid body segments: trunk, right scapula, and right upper arm. Local anatomical coordinate systems, following the right hand rule, were defined for each segment based on the UE marker set (Table 2). Euler angles were used to describe the joint kinematics of the distal segment relative to the proximal segment. Scapula orientation relative to the thorax (Z, X’, Y”) was described as internal and external rotation (about the Zs axis), downward and upward rotation (about the Xs’ axis), and posterior and anterior tilting (about the Ys” axis) in the thorax coordinate system (Nawoczenski et al., 2003). Humeral orientation relative to the scapula (X, Y’, Z”) was described as adduction and abduction (about the Xh axis), flexion and extension (about the Yh’ axis), and internal and external rotation (about the Zh” axis) in the scapula coordinate system (Nawoczenski et al., 2003).
Scapulothoracic and glenohumeral kinematics were calculated for all trials, and the first and last trials for all conditions were disregarded. For the remaining three trials, a starting and ending event was defined for each condition to extract the data of interest. For the level and ramp propulsion conditions, one propulsion cycle was chosen from each trial for analysis. The start and end of the propulsion cycle were defined based on the detection of an applied propulsion moment to the handrim and the removal of that applied moment (Kwarciak et al., 2007). The starting event of the weight relief maneuver occurred at detection of an applied inferior force on the handrim, and the ending event occurred when the handrim force returned to zero (subjects returned to rest and removed their hands from the rim). The data chosen from each trial were normalized to 101 points and averaged to obtain a mean cycle for each subject and each condition. The shoulder intersegmental kinetics for the subjects and conditions reported in this study were previously reported (Morrow et al., 2009). The scapulothoracic and glenohumeral kinematics occurring at peak intersegmental superior joint loading (Morrow et al., 2009) were identified for each subject using an algorithm implemented in MATLAB (Mathworks Inc., Natick, MA, USA) (Morrow et al., 2009). The kinematics were averaged for all subjects.
Statistical Analysis
The variables of interest were the mean scapulothoracic and glenohumeral kinematics during level propulsion, ramp propulsion, and weight relief lift at the point of peak loading as reported by Morrow et al. (Morrow et al., 2009). A one-way ANOVA with three repeated measures (level, ramp, and weight relief) was performed for each variable of interest (α =.05). Separate analyses were performed for each rotation. When significant main effects were observed, post hoc Tukey pairwise comparisons (α = .05) were performed to compare the means of each kinematic variable between each condition. The Tukey test was chosen for its conservative analysis and control over Type 1 errors. All statistical analyses were performed in SAS (SAS Institute, Cary, NC, USA).
RESULTS
Group mean, time series scapulothoracic and glenohumeral kinematics are presented in Figures 2 and 3. For all conditions, the scapula remained internally rotated throughout the activity (Figure 2A). During level and ramp propulsion the scapula began at a minimum internal rotation (app. 33º and 37 º, respectively) which increased to a peak (app. 40º and 44 º, respectively) at the point the hand leaves the rim. Less internal rotation occurred during the weight relief task with a minimum (app. 24º) occurring at the onset of the lift and a maximum (app. 36º) at the onset of the hold. The scapula exhibited slight upward rotation throughout the activity for all conditions (Figure 2B), except for during level propulsion at the point when the hand leaves the rim (app. 1º). The maximum levels for upward rotation occurred mid-way through the push phase for the level and ramp propulsion conditions (app. −9º and 13º, respectively). During the weight relief, the maximum upward rotation (app. −10º) occurred just after the onset of the lift and the scapula was nearly neutral near the onset of the hold phase. Anterior tilt was maintained throughout all conditions (Figure 2C). The anterior tilt was roughly 53º for the entire weight relief task. The level and ramp propulsion exhibited a modest increase in anterior tilt excursion over weight relief with a minimum occurring during the push phase (app. 50º and 47º, respectively) and a maximum (app. 56º and 57º, respectively) at the end of the recovery phase. The glenohumeral joint remained in external rotation throughout all conditions (Figure 3). Both the level and ramp propulsion conditions have a minimum (app. 12º and 13º, respectively) external rotation at the onset of propulsion and a maximum (app. 39º and 38º, respectively) immediately after the hands left the rim. In the weight relief, the humerus maintains an external rotation of approximately 10º, with a slight decrease during the lift and decent phases.
Figure 2.
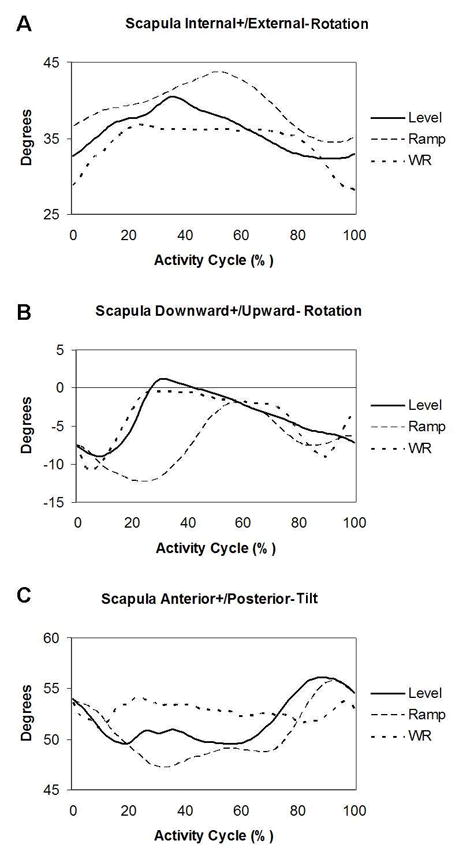
Group mean scapulothoracic kinematics during level propulsion, ramp propulsion, and a weight relief lift.
Figure 3.
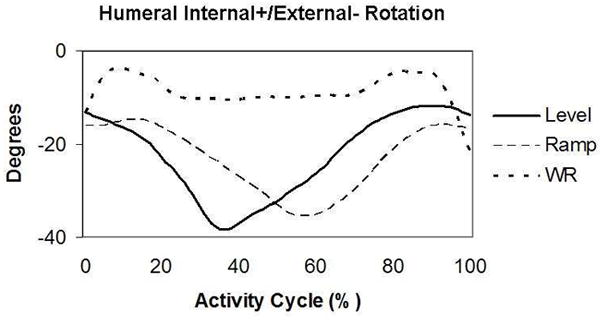
Group mean transverse glenohumeral kinematics during level propulsion, ramp propulsion, and a weight relief lift.
During level and ramp propulsion, peak superior intersegmental loading occurred immediately before the end of the push phase prior to the hand leaving the rim (Morrow et al., 2009). This was approximately between 25–30% of the level propulsion cycle and between 45–55% of the ramp propulsion cycle. The peak superior intersegmental loading for the weight relief occurred during the hold phase of the lift between 25–75% of the cycle. Glenohumeral internal/external rotation showed a significant difference between conditions (p=.03) and post hoc analysis revealed that the weight relief lift displayed significantly less external rotation at peak loading when compared to level and ramp propulsion (Figure 4). There were no significant differences for the scapulothoracic kinematics between conditions at the occurrence of peak loading (Figure 4). At peak loading, the scapula for all conditions was anteriorly tilted and internally rotated. The scapula was additionally either slightly upwardly or downwardly rotated.
Figure 4.
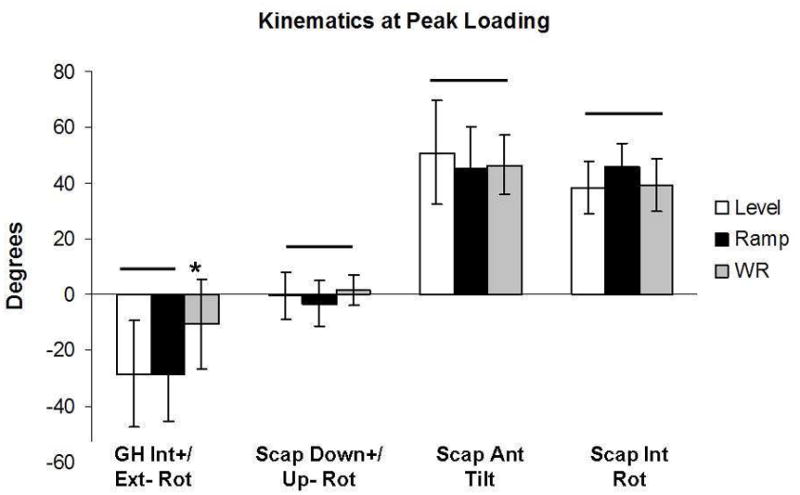
Kinematics at peak shoulder loading (mean ± SD). GH=glenohumeral; Scap=scapulothoracic; Int=internal; Ext=external; Down=downward; Up=upward; and Ant=anterior. * indicates a statistically significant difference.
DISCUSSION
Specific scapula kinematic patterns have been identified as leading contributors to the development of shoulder impingement syndrome in the non-weight bearing shoulder. As impingement is the most common UE pathology experienced by manual wheelchair users, it is logical that these potentially harmful orientations are also commonly observed in tasks associated with manual wheelchair propulsion. The repetitive nature of manual wheelchair activities places the manual wheelchair user at an increased risk for impingement development when compared to the typical non-weight bearing shoulder. Previous work has described the scapular orientation associated with transfers, weight relief lifts, standing depression lifts, and standing frame posture (Finley et al., 2005, Nawoczenski et al., 2003, Riek et al., 2008). The work presented here expands upon the previous observations to include propulsion activities and weight relief lifts in conjunction with shoulder joint intersegmental loading.
Common to all conditions explored in this study was an externally rotated glenohumeral joint and an anterior tilted and internally rotated scapula. Also similar is the small degree of upward scapula rotation for the complete activity. As the propulsion condition is the same between level ground and up a ramp, it was of no surprise that the scapulothoracic and glenohumeral kinematic profiles presented here were similar between the two. As a larger percentage of the propulsion cycle is spent in the push phase of ramp propulsion, the relative peaks and minimums of the kinematics are simply shifted for the increased push phase and decreased recovery phase. Not represented in the data shown here are the glenohumeral abduction and flexion angles, wherein the differences in kinematics are observed between level and ramp propulsion. The weight relief was associated with similar kinematic magnitudes to the propulsion conditions, but with an expected differing pattern.
At the point of peak superior intersegmental loading, the scapulothoracic kinematics for all activities were typical of an orientation that decreases the subacromial space: high degree of anterior tilt and internal rotation (Ludewig and Cook, 2000, Lukasiewicz et al., 1999, Solem-Bertoft et al., 1993, Warner et al., 1992). An upward rotated scapula may allow for a larger subacromial space (Babyar, 1996), but at peak loading, the scapula was maintained in a relatively neutral downward/upward rotation for all activities. The only significant difference between kinematics was observed in the decreased level of external rotation of the glenohumeral joint during the weight relief activity. This decreased external rotation of the humerus may increase the deformation of the soft tissues in the subacromial space (Flatow et al., 1994). For all activities, the kinematics are of concern in terms of compromising the subacromial space, but in conjunction with the level of loading at the joint (Morrow et al., 2009), the weight relief task has the highest relative risk of associated impingement. The loading of the humerus in the superior direction in a weight relief lift is at least twice the loading experienced during ramp or level propulsion. This superior force acts to translate the humeral head into the structures of the subacromial space (Van Drongelen et al., 2005). This force can potentially lead to soft tissue impingement.
Two previous studies investigated scapular and humeral kinematics a weight relief lift (Nawoczenski et al., 2003, Riek et al., 2008) (Table 3). The current study used the event of shoulder peak superior intersegmental loading for data reporting of weight relief kinematics while Riek et al. (2008) used an assumed point of peak loading and Nawoczenski et al. (2003) reported data at the beginning of the hold phase. The scapulothoracic upward rotation in the current study was lower than in previous investigations and the anterior tilt was higher. The scapular internal rotation was comparable to both studies and the magnitude of humeral transverse rotation was comparable to Nawoczenski et al (2003). There were many methodological differences between the current and previous investigations, beyond the event at which data was reported, that can possibly explain the variation in kinematics. Riek et al. (2008) and Nawoczenski et al. (2003), used an electromagnetic tracking sensor on the acromion to follow scapular motion. The current study used population data for anatomical landmarks while the previous studies used subject-specific landmarks. The humeral differences between the studies at the point of peak loading may be due to the placement of the hands during the maneuver. The subjects in this study performed the lift on the instrumented rim while in the previous study, the subjects were instructed to place their hands wherever they felt comfortable (rim, wheel, or armrest). The differences in anterior tilt may be related to possible offsets caused by placement of the scapula tracker on the scapular spine. No comparisons can be made with the scapular kinematics of level and ramp propulsion as these have never been described.
Table 3.
Comparison of scapular and humeral kinematics at peak loading during a weight relief lift
| Study | Scapular Upward Rotation | Scapula Anterior Tilt | Scapular Internal Rotation | Humeral I/E Rotation |
|---|---|---|---|---|
| Current Study | 1º±5º | 46º±10º | 40º±10º | 10º±16º E |
| Riek et al (2008) | 20º±5º | 11º±5º | 47º±3º | 15º±5º I |
| Nawoczenski et al (2003) | 20º±5º | 19º±11º | 60º±12º | 4º±15º E |
Values are mean ± SD
Abbreviations: I=Internal, E=External
In addition to load and kinematic considerations, frequency of activity performance factors into the risk of development of shoulder impingement syndrome. All activities demonstrated potentially injurious scapular orientations, and unfortunately, the activities described here are frequent components of daily life for a manual wheelchair user. It is recommended that weight relief lifts are performed every 15 minutes to prevent ulcer development and maintain tissue health (1992), and propulsion, whether level or ramp, is essential for daily mobility and independence. These observations place the shoulder complex of a manual wheelchair user in disadvantageous positions for the majority of the time spent in a wheelchair.
The subject cohort in this study was composed, generally, of people with paraplegia (injuries at or below T4, spina bifida in one subject). In persons with paraplegia (at or below T1 injury) general function of the shoulder and scapular stabilizers are maintained with varied control of the trunk musculature. As muscle control will differ depending on injury level, the kinematics from this study are not representative of persons with tetraplegia. In a tetraplegic population, scapular stabilizers and other shoulder musculature will begin to be affected at levels as low as T8, which will alter the ability of the scapula and humerus to function as expected during upper extremity motions (Kendall and McCreary, 1983). As injury levels move up the cervical level, the ability to propel a manual wheelchair and perform weight reliefs diminish.
This study had limitations. First, anatomical landmark locations were not collected for each subject. Alternatively, population data were used from cadaveric scapulae. This aspect of the methodology assumes that the cadaveric samples represented a range of anatomical variability that would encompass our subjects’ specific anthropometrics. This method limits the ability to directly compare our results with previous studies, and should not be a standard of practice in moving forward. Second, while subjects were able to use their own chair frame, they were instructed to perform all propulsion and lift activities using only the instrumented rim and not the tire. This may contribute to over or underestimation in the kinematics presented here. Third, the propulsion activities were performed in a laboratory setting and not in the user’s usual environment. To mimic the activities to the best of our ability, subjects were not constrained to an ergometer and subjects were instructed to propel at a comfortable speed. Fourth, an independent accuracy study on the scapula tracker used in this study was not performed. The accuracy was assumed to be equivalent to results presented on a similar scapula tracking methods that lays atop the scapular spine (Karduna et al., 2001). Finally, this study did not address the effects potential activity modifications or rehabilitation could have on advantageously altering the scapular kinematics. Further investigation is necessary to address what biomechanical and behavioral changes could be enacted through strengthening and retraining to reorient the scapula during these common manual wheelchair activities.
In conclusion, all the investigated activities placed the scapula in a potentially dangerous position for development of shoulder impingement syndrome. The weight relief lift, with a decrease in glenohumeral external rotation and large superior forces at the shoulder in addition to a detrimental scapula orientation, potentially places the shoulder of the manual wheelchair user at the greatest risk for impingement soft tissue injury. Preventative strength training and activity modification in the form weight relief shifts and leans as opposed to body lifts may provide measures to slow progression of impingement development and associated pain in the manual wheelchair user.
Acknowledgments
The authors acknowledge Kathie Bernhardt and Diana Hansen for their assistance with subject testing and data processing. All aspects of this study were funded by a grant from the National Institutes of Health (R01HD48781).
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Agency for Health Care Policy and Research. Pressure ulcers in adults: prediction and prevention. Clin Pract Guidel Quick Ref Guide Clin. 1992:1–15. [PubMed] [Google Scholar]
- BABYAR SR. Excessive scapular motion in individuals recovering from painful and stiff shoulders: causes and treatment strategies. Phys Ther. 1996;76:226–38. doi: 10.1093/ptj/76.3.226. discussion 239–47. [DOI] [PubMed] [Google Scholar]
- BAYLEY JC, COCHRAN TP, SLEDGE CB. The weight-bearing shoulder. The impingement syndrome in paraplegics. Journal of Bone & Joint Surgery. 1987;69:676–8. [PubMed] [Google Scholar]
- FINLEY MA, MCQUADE KJ, RODGERS MM. Scapular kinematics during transfers in manual wheelchair users with and without shoulder impingement. Clin Biomech (Bristol, Avon) 2005;20:32–40. doi: 10.1016/j.clinbiomech.2004.06.011. [DOI] [PubMed] [Google Scholar]
- FLATOW EL, SOSLOWSKY LJ, TICKER JB, PAWLUK RJ, HEPLER M, ARK J, MOW VC, BIGLIANI LU. Excursion of the rotator cuff under the acromion. Patterns of subacromial contact. Am J Sports Med. 1994;22:779–88. doi: 10.1177/036354659402200609. [DOI] [PubMed] [Google Scholar]
- GELLMAN H, CHANDLER DR, PETRASEK J, SIE I, ADKINS R, WATERS RL. Carpal tunnel syndrome in paraplegic patients. Journal of Bone & Joint Surgery. 1988a;70:517–9. [PubMed] [Google Scholar]
- GELLMAN H, SIE I, WATERS RL. Late complications of the weight-bearing upper extremity in the paraplegic patient. Clinical Orthopaedics & Related Research. 1988b:132–5. [PubMed] [Google Scholar]
- KARDUNA AR, MCCLURE PW, MICHENER LA, SENNETT B. Dynamic measurements of three-dimensional scapular kinematics: a validation study. J Biomech Eng. 2001;123:184–90. doi: 10.1115/1.1351892. [DOI] [PubMed] [Google Scholar]
- KENDALL FP, MCCREARY EK. Muscles: Testing and Function. Baltimore, MD: Williams and Wilkins; 1983. [Google Scholar]
- KWARCIAK AM, SISTO SA, YAROSSI BS. Gait and clinical movement analysis society. Springfield; MA, USA: 2007. Proposal to standardize and redefine the phases of manual wheelchair propulsion. [Google Scholar]
- LEE TQ, MCMAHON PJ. Shoulder biomechanics and muscle plasticity: implications in spinal cord injury. Clin Orthop Relat Res. 2002:S26–36. doi: 10.1097/00003086-200210001-00004. [DOI] [PubMed] [Google Scholar]
- LUDEWIG PM, COOK TM. Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Phys Ther. 2000;80:276–91. [PubMed] [Google Scholar]
- LUKASIEWICZ AC, MCCLURE P, MICHENER L, PRATT N, SENNETT B. Comparison of 3-dimensional scapular position and orientation between subjects with and without shoulder impingement. J Orthop Sports Phys Ther. 1999;29:574–83. doi: 10.2519/jospt.1999.29.10.574. discussion 584–6. [DOI] [PubMed] [Google Scholar]
- MORROW MM, HURD WJ, KAUFMAN KR, AN KN. Shoulder demands in manual wheelchair users across a spectrum of activities. J Electromyogr Kinesiol. 2009 doi: 10.1016/j.jelekin.2009.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- NATIONAL SPINAL CORD INJURY STATISTICAL CENTER, N. Spinal cord injury facts and figures at a glance. 2010. [PubMed] [Google Scholar]
- NAWOCZENSKI DA, CLOBES SM, GORE SL, NEU JL, OLSEN JE, BORSTAD JD, LUDEWIG PM. Three-dimensional shoulder kinematics during a pressure relief technique and wheelchair transfer. Arch Phys Med Rehabil. 2003;84:1293–300. doi: 10.1016/s0003-9993(03)00260-0. [DOI] [PubMed] [Google Scholar]
- NEER CS., 2ND Anterior acromioplasty for the chronic impingement syndrome in the shoulder: a preliminary report. J Bone Joint Surg Am. 1972;54:41–50. [PubMed] [Google Scholar]
- NICHOLS PJ, NORMAN PA, ENNIS JR. Wheelchair user's shoulder? Shoulder pain in patients with spinal cord lesions. Scandinavian Journal of Rehabilitation Medicine. 1979;11:29–32. [PubMed] [Google Scholar]
- PENNES DR, SHIRAZI KK, MARTEL W. Bilateral palmar flexion instability: a complication of wheelchair use. AJR American Journal of Roentgenology. 1983;141:1327–8. doi: 10.2214/ajr.141.6.1327. [DOI] [PubMed] [Google Scholar]
- PENTLAND WE, TWOMEY LT. The weight-bearing upper extremity in women with long term paraplegia. Paraplegia. 1991;29:521–30. doi: 10.1038/sc.1991.75. [DOI] [PubMed] [Google Scholar]
- PIAZZA SJ, CHOU L-S, DENNISTON NL, MCMULKIN ML, QUIGLEY EJ, RICHARDS JG, SCHWARTZ MH. Gait and Clinical Movement Analysis Society. Springfield; MA: 2007. A proposed standard of assessing the marker-location accuracy of video-based motion analysis systems. [Google Scholar]
- REQUEJO PS, MULROUY SJ. Evidence-Based Strategies to Preserve Shoulder Function in Manual Wheelchair Users with Spinal Cord Injury. Topics in Spinal Cord Injury Rehabilitation. 2008 Spring;13:86–119. [Google Scholar]
- RIEK LM, LUDEWIG PM, NAWOCZENSKI DA. Comparative shoulder kinematics during free standing, standing depression lifts and daily functional activities in persons with paraplegia: considerations for shoulder health. Spinal Cord. 2008;46:335–43. doi: 10.1038/sj.sc.3102140. [DOI] [PubMed] [Google Scholar]
- SOLEM-BERTOFT E, THUOMAS KA, WESTERBERG CE. The influence of scapular retraction and protraction on the width of the subacromial space. An MRI study. Clin Orthop Relat Res. 1993:99–103. [PubMed] [Google Scholar]
- VAN DRONGELEN S, VAN DER WOUDE LH, JANSSEN TW, ANGENOT EL, CHADWICK EK, VEEGER DH. Mechanical load on the upper extremity during wheelchair activities. Archives of Physical Medicine & Rehabilitation. 2005;86:1214–20. doi: 10.1016/j.apmr.2004.09.023. [DOI] [PubMed] [Google Scholar]
- WARNER JJ, MICHELI LJ, ARSLANIAN LE, KENNEDY J, KENNEDY R. Scapulothoracic motion in normal shoulders and shoulders with glenohumeral instability and impingement syndrome. A study using Moire topographic analysis. Clin Orthop Relat Res. 1992:191–9. [PubMed] [Google Scholar]
- WU G, VAN DER HELM FC, VEEGER HE, MAKHSOUS M, VAN ROY P, ANGLIN C, NAGELS J, KARDUNA AR, MCQUADE K, WANG X, WERNER FW, BUCHHOLZ B. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion--Part II: shoulder, elbow, wrist and hand. J Biomech. 2005;38:981–992. doi: 10.1016/j.jbiomech.2004.05.042. [DOI] [PubMed] [Google Scholar]
- ZHAO K, YANG C, ZHAO C, AN KN. Assessment of non-invasive intervertebral motion measurements in the lumbar spine. J Biomech. 2005;38:1943–6. doi: 10.1016/j.jbiomech.2004.07.029. [DOI] [PubMed] [Google Scholar]