

Abstract
Background
Lung cancer and tuberculosis cause significant morbidity and mortality worldwide. Tuberculosis may increase lung cancer risk through substantial and prolonged pulmonary inflammation. However, prospective data on tuberculosis and lung cancer risk are limited.
Methods
Our study included 29,133 Finnish male smokers followed prospectively in the Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study (1985–2005). Lung cancers were identified through linkage with the Finish Cancer Registry, and hospital-treated tuberculosis cases were ascertained from the National Hospital Discharge Register. We assessed the association between tuberculosis and lung cancer risk with proportional hazards regression models, adjusting for age and cigarette smoking.
Results
Forty-four lung cancer cases occurred among 273 men with tuberculosis (incidence rate=1,786 per 100,000 person-years). Tuberculosis was associated with a two-fold elevation in lung cancer risk (hazard ratio [HR]=1.97; 95% confidence interval [CI] 1.46–2.65) with significant associations observed for both incident (HR=2.05; 95% CI 1.42–2.96) and prevalent tuberculosis (HR=1.82; 95% CI 1.09–3.02). Lung cancer risk was greatest in the two-year window after tuberculosis diagnosis (HR=5.01; 95% CI 2.96–8.48), but remained elevated at longer latencies (HR=1.53; 95% CI 1.07–2.20). Though tuberculosis was associated with an increased risk of squamous cell carcinoma (HR=3.71), adenocarcinoma (HR=1.71), small cell carcinoma (HR=1.72), and lung cancer of other (HR=1.23) and unknown histologies (HR=1.35), only the association for squamous cell carcinoma was statistically significant.
Conclusions
Tuberculosis is associated with increased lung cancer risk in male smokers.
Impact statement
Our results add to the growing body of evidence implicating chronic inflammation and pulmonary scarring in the etiology of lung cancer.
INTRODUCTION
Lung cancer and tuberculosis are two major public health problems that cause significant morbidity and mortality worldwide. Internationally, lung cancer is the most common malignancy and causes the largest number of cancer-related deaths with an estimated 1.35 million cases diagnosed and 1.18 million deaths occurring annually (1). An estimated 90–95% of lung cancers among men in North America and Europe can be attributed to cigarette smoking (1). According to the World Health Organization, approximately 9.4 million incident cases of tuberculosis and 1.3 million deaths attributable to tuberculosis occurred in 2008 (2). Tuberculosis results from the reactivation of latent infection with Mycobacterium tuberculosis, which currently infects one-third of the world’s population (3).
Lung infections, including tuberculosis, have been implicated as potentially contributing to the etiology of lung cancer (4). Tuberculosis may increase the risk of lung cancer through substantial and prolonged pulmonary inflammation, leading to host tissue damage, fibrosis, scar formation, and genetic alterations (3–6). A recent meta-analysis reported tuberculosis to be associated with a 1.7-fold elevation in the risk of lung cancer (7). However, the majority of prior investigations have been case-control studies, and there are very limited prospective data regarding tuberculosis and lung cancer risk. As cigarette smoking is such a strong risk factor for lung cancer, it is possible that smoking and tuberculosis act synergistically to cause damage to the lungs and subsequently increase lung cancer risk.
In the current study, we assessed the association between tuberculosis and lung cancer risk in Finnish male smokers enrolled in the Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study and followed over a 20-year period. Further, we estimated the risk of lung cancer with varying latencies after tuberculosis diagnosis. Strengths of our study include the availability of detailed data on tobacco use, documentation of tuberculosis diagnoses using hospital records, and information on specific histological subtypes of lung cancer.
MATERIALS AND METHODS
Study population
Subjects in the present study were enrolled in the Alpha-Tocopherol, Beta-Carotene Cancer Prevention (ATBC) Study, a randomized, double-blind trial designed to assess whether supplementation with alpha-tocopherol and beta-carotene reduces the risk of lung cancer (8, 9). The ATBC Study enrolled 29,133 men living in southwestern Finland in 1985–1988. Men were 50 to 69 years old, smoked at least five cigarettes per day, and were randomized to receive either alpha-tocopherol supplements, beta-carotene supplements, both supplements, or a placebo. Participants completed questionnaires at randomization, providing information on demographics, diet, and medical, tobacco and occupational histories (9). The trial ended on April 30, 1993, but study participants continued to be followed for cancer outcomes and mortality through 2005.
Lung cancers were identified through linkage with the Finnish Cancer Registry, which provides nearly 100% case ascertainment in Finland (10). For cases diagnosed through April 1999, medical records were reviewed centrally by 1 or 2 study physicians for diagnostic confirmation. Cases diagnosed after April 1999 had only the Finnish Cancer Registry data for information on site, histology, and date of diagnosis.
Information on cases of hospital-treated tuberculosis (ICD-9 codes 010-012) during 1976–1995 was available from the National Hospital Discharge Register, which includes inpatient visit information from all public and private hospitals. Hospital-treated tuberculosis diagnoses were available both prior to randomization (prevalent tuberculosis) and from randomization through 1995 (incident tuberculosis). Of the 330 hospital-treated cases of tuberculosis, 57 were extra-pulmonary cases, and were not included as tuberculosis cases in this analysis. Additionally, 114 men (20 men with registered cases of hospital-treated tuberculosis and 94 without hospital-treated tuberculosis) were diagnosed with late effects of tuberculosis, defined as sequelae due to old or inactive tuberculosis (i.e., ICD-9 code 137.0). We treated these hospital reports separately, as we did not know their tuberculosis diagnosis dates.
Statistical Analysis
First, proportional hazards regression models were used to assess associations between participant characteristics, vitamin intake and history of pulmonary disease with the risk of incident tuberculosis. For our main analysis, we examined the association between tuberculosis and lung cancer risk with proportional hazards regression models. Participants were followed from randomization to the first diagnosis of lung cancer, death or December 31, 2005. Age was used as the hazard time metric to fully control for confounding by age. Tuberculosis was treated as a time-varying covariate: men diagnosed with incident tuberculosis contributed unexposed person-time prior to tuberculosis diagnosis and exposed person-time after tuberculosis diagnosis; men diagnosed with prevalent tuberculosis at randomization contributed only exposed person-time; and men who never developed tuberculosis contributed only unexposed person-time. In a separate analysis, we added a variable to assess risk associated with tuberculosis sequelae.
Cigarette use was assessed at baseline, and all models were adjusted for cigarette smoking with logcig-years (log[cigarettes smoked per day + 1] * number of years smoked), which has previously been shown to better capture smoking information in relation to lung cancer risk than traditional smoking metrics (11). Additionally, we examined trial intervention arm, vitamin C intake (in a previous ATBC Study, vitamin C intake was protective against tuberculosis (12)), and baseline history of asthma, emphysema and chronic bronchitis as potential confounders. However, because these factors did not substantially alter the association between tuberculosis and lung cancer risk (data not shown), they were not included in the final models.
Additionally, we used proportional hazards regression models to examine whether the association between tuberculosis and lung cancer risk was modified by the duration of time after tuberculosis (i.e., latency, defined as 0–1.9 years, 2–9.9 years, and 10+ years after tuberculosis diagnosis). Further, we assessed the association between tuberculosis and specific lung cancer histological types (squamous cell carcinoma, adenocarcinoma, other histology and unknown histology), and evaluated lung cancer risk associated with incident and prevalent hospital-treated tuberculosis separately. We also tested for the presence of statistical interaction between tuberculosis and logcig-years, treating logcig-years as a continuous variable or a binary variable, dichotomized at the median. In a sensitivity analysis, we ended follow-up on December 31, 1995, limiting the analysis to the time period when participants were followed for tuberculosis diagnoses.
RESULTS
The median age of the 29,133 men included in this study was 57 years at the time of randomization. All participants were smokers. At randomization, the men smoked a median of 20 cigarettes/per day and had a cumulative tobacco use of 36 pack-years. According to the baseline questionnaire, 3.1% of participants had asthma, 6.5% had emphysema and 7.7% had chronic bronchitis (Table 1).
Table 1.
Characteristics of 29,133 men in the ATBC Study at randomization and associations with tuberculosis.
| All Participants | Prevalent tuberculosis | Incident tuberculosis | ||
|---|---|---|---|---|
| N (%) | N (%) | N (%) | HR (95% CI) | |
| Total | 29,133 (100) | 88 (100) | 185 (100) | |
| Age at randomization, years | ||||
| 50–53 | 6,449 (22.1) | 16 (18.2) | 27 (14.6) | 1.0 |
| 53–57 | 7,863 (27.0) | 21 (23.9) | 42 (22.7) | 1.24 (0.77–2.02) |
| 57–61 | 6,936 (23.8) | 18 (20.5) | 41 (22.2) | 1.37 (0.84–2.23) |
| 61–69 | 7,885 (27.1) | 33 (37.5) | 75 (40.5) | 2.24 (1.44–3.48) p-trend=0.0001 |
| Cigarettes per day | ||||
| 5–14 | 5,934 (20.4) | 24 (27.3) | 22 (11.9) | 1.0 |
| 15–19 | 4,625 (15.9) | 14 (15.9) | 31 (16.8) | 1.62 (0.93–2.81) |
| 20–24 | 9,255 (31.8) | 22 (25.0) | 71 (38.4) | 1.98 (1.23–3.20) |
| 25+ | 9,319 (32.0) | 28 (31.8) | 61 (33.0) | 1.62 (0.99–2.64) P-trend=0.07 |
| Pack-years smoked | ||||
| 0–24 | 7,376 (25.3) | 25 (28.4) | 25 (13.5) | 1.0 |
| 25–35 | 7,329 (25.1) | 16 (18.2) | 44 (23.8) | 1.69 (1.03–2.78) |
| 36–46 | 7,260 (24.9) | 21 (23.9) | 59 (31.9) | 2.24 (1.40–3.58) |
| 47+ | 7,177 (24.6) | 26 (29.6) | 57 (30.8) | 2.27 (1.41–3.64) P-trend=0.0004 |
| Alpha-tocopherol arm | ||||
| No | 14,569 (50.0) | 45 (51.1) | 86 (46.5) | 1.0 |
| Yes | 14,564 (50.0) | 43 (48.9) | 99 (53.5) | 1.10 (0.82–1.47) |
| Beta-carotene arm | ||||
| No | 14,573 (50.0) | 49 (55.7) | 91 (49.2) | 1.0 |
| Yes | 14,560 (50.0) | 39 (44.3) | 94 (50.8) | 1.08 (0.81–1.45) |
| Baseline vitamin C intake (mg/day) | ||||
| <92.5 | 13,565 (50.0) | 36 (47.4) | 107 (63.7) | 1.0 |
| 92.5+ | 13,546 (50.0) | 40 (52.6) | 61 (36.3) | 0.57 (0.41–0.78) |
| Missing | 2,022 | 12 | 17 | |
| History of asthma | ||||
| No | 28,232 (96.9) | 82 (93.2) | 167 (90.3) | 1.0 |
| Yes | 901 (3.1) | 6 (6.8) | 18 (9.7) | 3.97 (2.43–6.48) |
| History of emphysema | ||||
| No | 27,234 (93.5) | 73 (83.0) | 145 (78.4) | 1.0 |
| Yes | 1,899 (6.5) | 15 (17.1) | 40 (21.6) | 3.75 (2.62–5.36) |
| History of chronic bronchitis | ||||
| No | 26,888 (92.3) | 71 (80.7) | 148 (85.4) | 1.0 |
| Yes | 2,245 (7.7) | 17 (19.3) | 27 (14.6) | 2.27 (1.51–3.42) |
Eighty-eight cases of hospital-treated tuberculosis were identified prior to randomization (i.e., prevalent cases), and 185 incident cases of tuberculosis occurred during follow-up through December 31, 1995 (incidence rate=135 per 100,000 person-years). As shown in Table 1, the risk of incident tuberculosis increased with age (p-trend<0.0001) and with pack-years smoked (p-trend=0.0004). A history of asthma, emphysema or chronic bronchitis was also associated with increased risk of incident tuberculosis, while baseline intake of vitamin C was inversely associated. Among the hospital-treated prevalent cases of tuberculosis, the median time from diagnosis to randomization was 1.7 years, and ranged up to 10.5 years.
During 1985-2005, 3,102 cases of lung cancer occurred for an incidence rate of 744 cases per 100,000 person-years. The most common lung cancer histologies were squamous cell carcinoma (n=788, 25.4%), small cell carcinoma (n=427, 14.0%), and adenocarcinoma (n=257, 8.3%). There were 461 (14.9%) lung cancers of other histological types and 1,169 (37.7%) cases with an unknown histology. Forty-four men who developed lung cancer had a prior diagnosis of either incident or prevalent tuberculosis.
Tuberculosis (incidence and prevalent tuberculosis cases combined) was associated with a two-fold elevation in risk of lung cancer (HR=1.97; 95% confidence interval [CI] 1.46–2.65; Table 2). Lung cancer risk was greatest in the two year window after tuberculosis diagnosis (HR=5.01; 95% CI 2.96–8.48) but continued to be elevated at longer latencies (Figure 1), with a 50% increased risk of lung cancer in the overall period two or more years after tuberculosis diagnosis (HR=1.53; 95% CI 1.07–2.20). When men diagnosed with tuberculosis sequelae were included in the model, the lung cancer HR for tuberculosis was 1.88 (95% CI 1.39–2.54) and the lung cancer HR for tuberculosis sequelae was 2.00 (95% CI 1.23–3.23). No interaction was observed between tuberculosis and logcig-years treated as a continuous (p=0.36) or a dichotomous variable (p=0.84). When follow-up time was censored in 1995, the association between tuberculosis and lung cancer was somewhat stronger (HR=2.38; 95% CI 1.57–3.59, based on 1,320 lung cancer cases).
Table 2.
Tuberculosis and lung cancer risk by histology among men in the ATBC Study, 1985–2005.
| Lung Cancer Cases | Incidence Rate, per 100,000 person-years | Hazard Ratio* | 95% CI | |
|---|---|---|---|---|
| All lung cancers | ||||
| No tuberculosis | 3058 | 737 | 1.0 | |
| Tuberculosis | 44 | 1,786 | 1.97 | 1.46–2.65 |
| Squamous cell carcinoma | ||||
| No tuberculosis | 767 | 197 | 1.0 | |
| Tuberculosis | 21 | 917 | 3.71 | 2.40–5.72 |
| Adenocarcinoma | ||||
| No tuberculosis | 254 | 66 | 1.0 | |
| Tuberculosis | 3 | 136 | 1.71 | 0.55–5.35 |
| Small cell carcinoma | ||||
| No tuberculosis | 422 | 109 | 1.0 | |
| Tuberculosis | 5 | 226 | 1.72 | 0.71–4.15 |
| Other cancer histology | ||||
| No tuberculosis | 457 | 118 | 1.0 | |
| Tuberculosis | 4 | 180 | 1.23 | 0.46–3.28 |
| Unknown cancer histology | ||||
| No tuberculosis | 1158 | 288 | 1.0 | |
| Tuberculosis | 11 | 469 | 1.35 | 0.75–2.45 |
All hazard ratios were adjusted for age and baseline tobacco use using the logcig-years metric (see Methods).
Figure 1. Risk of lung cancer according to duration of time since tuberculosis.
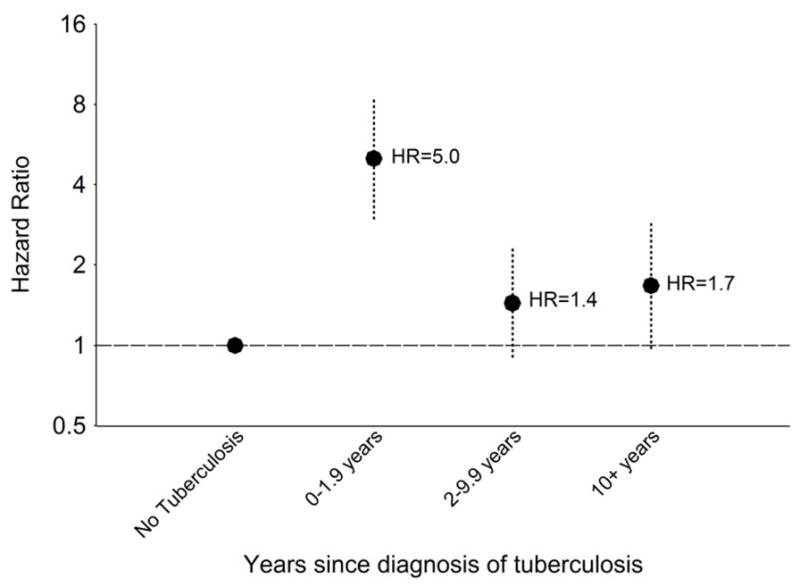
Figure 1 shows the risk of lung cancer 0–1.9 years, 2–9.9 years and 10+ years after tuberculosis diagnosis. Points indicate hazard ratios (HRs) and vertical dotted lines indicate 95% confidence intervals (CIs). The horizontal dashed lines shows the reference value correspond to HR=1. Although not shown in the Figure, in the overall period 2+ years after tuberculosis diagnosis, the HR for lung cancer was 1.53 (95% CI 1.07–2.20). All estimates were adjusted for age and baseline tobacco use using the logcig-years metric (see Methods).
When associations with tuberculosis were examined for separate lung cancer histologies (Table 2), we found a 3.7-fold elevated risk of squamous cell carcinoma; risks of adenocarcinoma, small cell carcinoma, and lung cancers of other and unknown histologies also appeared increased, though these estimates were not statistically significant. We also separately evaluated associations with incident and prevalent tuberculosis and found lung cancer risk was elevated following both (HR=2.05, 95% CI 1.42–2.96 and HR=1.82, 95% CI 1.09–3.02, respectively).
DISCUSSION
Among a population of Finnish male smokers, we found the risk of lung cancer to be doubled in men with tuberculosis. Lung cancer risk was greatest in the two-year period following tuberculosis diagnosis, but elevated risk persisted with longer follow-up. Further, the association between tuberculosis and lung cancer was not explained by cigarette smoking, as all men in ATBC were smokers and our analyses adjusted for intensity and duration of tobacco use.
Tuberculosis is thought to increase lung cancer risk through chronic pulmonary inflammation and fibrosis (4). Tuberculosis infection causes a profound and extended host immune response, with inflammatory cells in the lung producing extensive cytokine signaling cascades, reactive nitrogen and oxygen species, prostaglandins, and tissue-destructive proteases (5). Even tuberculosis patients who receive treatment may have prolonged pulmonary inflammation, because tuberculosis symptoms occur months before diagnosis, and the treatment for tuberculosis requires a drug regimen administered over an extended period of time (3). In turn, prolonged pulmonary inflammation may cause tissue damage and genomic alterations. Further, repair of tissue damage caused by tuberculosis can lead to pulmonary fibrosis and scarring (5), which is also linked to increased lung cancer risk (6). Of note, we found that men diagnosed with tuberculosis sequelae also had an elevated risk of lung cancer. This diagnosis likely captures men who had suffered severe lung damage due to tuberculosis infection, and our observation thus supports the importance of fibrosis in promoting carcinogenesis.
Two previous cohort studies and a number of case-control studies have examined the association between tuberculosis and lung cancer with mixed results. Our results are consistent with one previous prospective study that found a six-fold increase in lung cancer risk with tuberculosis (3); however, another cohort study found no association (13). Some case-control studies have reported associations between tuberculosis and lung cancer with odds ratios ranging from 1.6–4.2 (14–16), while others observed no association (17–19). As the strength of the association between tuberculosis and lung cancer appears to attenuate at longer latencies, it is possible that studies ascertaining tuberculosis history at one time point may have been primarily identifying cases occurring many years or even decades earlier. This, along with poor exposure assessment and limited power to detect differences, may account for some of the null results in previously published studies.
When we stratified lung cancer cases by histology, we observed tuberculosis to be significantly associated with squamous cell carcinoma. Though the results for adenocarcinoma, small cell carcinoma, and other and unknown histologies were not statistically significant, HRs for these endpoints were in the direction of increased risk, and were based on a small number of lung cancer cases with tuberculosis. Previous studies have found tuberculosis to be associated with both squamous cell carcinoma and adenocarcinoma of the lung (7, 14, 15).
Cigarette smoking remains the single most important risk factor for lung cancer, increasing risk 15- to 30-fold (20). Tuberculosis may work in conjunction with tobacco to produce chronic inflammation, causing damage to lung tissues (4). In the current study, we did not detect a synergistic effect between the amount of tobacco used and tuberculosis. Previous case-control studies have found associations between tuberculosis and lung cancer in never smokers (7), but we were not able to assess this population because the ATBC Study only included smokers.
We also considered the possibility that confounding by cigarette smoking might have biased our results. Tobacco use has been previously shown to be associated with tuberculosis (21, 22), and in our analysis higher cumulative smoking was associated with an increased risk of incident tuberculosis (Table 1). Though we cannot rule out that confounding may have influenced our results, the potential for bias in our study may be less than in others. As noted, the ATBC Study only included smokers, and we utilized the available smoking data to control for smoking behaviors. Also, when we compared HRs before and after adjusting for logcig-years, we observed only a modest attenuation of the association between tuberculosis and lung cancer from 2.2 to 2.0. This relatively small change further indicates that the inclusion criteria of the study, restricting the cohort to a fairly homogeneous population of smokers, already partially controlled for confounding by cigarette smoking.
Studies of tuberculosis and lung cancer may be limited by additional biases. First, surveillance bias may occur if people with tuberculosis are more apt to receive medical care and testing that may lead to lung cancer diagnosis. In particular, people with tuberculosis are evaluated with chest x-rays, resulting in a greater likelihood of diagnosing asymptomatic lung cancer. This bias is unlikely in our study, as all the men in the ATBC Study received chest x-rays at baseline, at 2.3 and 4.6 years after randomization and at the end of active follow-up (9). Another potential bias arises due to reverse causality, in that an occult lung cancer may weaken the immune system and result in the reactivation of latent M. tuberculosis infection (5). Thus, tuberculosis may become clinically apparent prior to the lung cancer, even though lung cancer preceded tuberculosis reactivation. Indeed, in our study the risk of lung cancer was greatest in the two-year window after hospital-treated tuberculosis. However, reverse causality is less likely to drive the association between tuberculosis and lung cancer as the latency period between tuberculosis and lung cancer increases. In our study, we observed a 50% increase in the risk of lung cancer two or more years after tuberculosis, suggesting a persistent association when tuberculosis temporally preceded lung cancer. Further, as participants received chest x-rays during the course of the study, some occult lung cancers would have been detected prior to becoming clinically evident, reducing the likelihood of reverse causation. Finally, follow-up for tuberculosis diagnoses ended in 1995, while follow-up for lung cancer diagnoses extended through 2005. Thus, cases of tuberculosis occurring during 1996–2005 could have been missed in our analysis, potentially attenuating the association with lung cancer. When the analysis was restricted to 1985–1995, the association between tuberculosis and lung cancer was somewhat stronger.
The main strength of our study was the use of prospectively collected data. The ATBC Study has a relatively large number of tuberculosis cases and extended follow-up for lung cancer diagnoses. In our analysis, the incidence rate of hospital-treated tuberculosis was 135 per 100,000 person-years. Though this rate seems high compared to other European countries, it is thought that many of the men, who were 50-70 years old in the 1980s, were infected at a young age when tuberculosis was highly endemic in Finland (12). Unlike the majority of prior studies (3, 13-19), the ATBC Study did not rely on self-report to ascertain tuberculosis diagnoses. Systematically collected information on hospital-treated tuberculosis reduced the risk of misclassification of exposure. Additionally, most of the ATBC Study clinics were part of an earlier population-based tuberculosis diagnosis and treatment system, further enhancing the likelihood of complete and accurate diagnoses.
In conclusion, our results add to the growing body of evidence implicating chronic inflammation and pulmonary scarring in the etiology of lung cancer (4, 6, 23). Though we observed the increased risk of lung cancer among men with tuberculosis to be independent of cigarette smoking, it is important to note the particularly harmful effects of cigarette smoking among those infected with tuberculosis. Not only is cigarette smoking the strongest risk factor for lung cancer, it is also associated with an elevated risk of developing tuberculosis, as well as subsequent tuberculosis recurrence and mortality (21, 22). Given the high risk of lung cancer in tuberculosis patients, future public health efforts should focus on encouraging smoking cessation. Evaluation of screening programs to detect early lung cancers should also be considered.
Acknowledgments
This study was supported by the Intramural Research Program of the National Cancer Institute. The ATBC Study was supported by the Intramural Research Program of the National Cancer Institute, NIH, and U.S. Public Health Service contracts N01-CN-45165, N01-RC-45035, N01-RC-37004, and HHSN261201000006C from the National Cancer Institute, Department of Health and Human Services.
Reference List
- 1.Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. doi: 10.3322/canjclin.55.2.74. [DOI] [PubMed] [Google Scholar]
- 2.World Health Organization. Tuberculosis. 104. 2010. [Google Scholar]
- 3.Engels EA, Shen M, Chapman RS, et al. Tuberculosis and subsequent risk of lung cancer in Xuanwei, China. Int J Cancer. 2009;124:1183–7. doi: 10.1002/ijc.24042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Engels EA. Inflammation in the development of lung cancer: epidemiological evidence. Expert review of anticancer therapy. 2008;8:605–15. doi: 10.1586/14737140.8.4.605. [DOI] [PubMed] [Google Scholar]
- 5.Nalbandian A, Yan BS, Pichugin A, Bronson RT, Kramnik I. Lung carcinogenesis induced by chronic tuberculosis infection: the experimental model and genetic control. Oncogene. 2009;28:1928–38. doi: 10.1038/onc.2009.32. [DOI] [PubMed] [Google Scholar]
- 6.Yu YY, Pinsky PF, Caporaso NE, et al. Lung cancer risk following detection of pulmonary scarring by chest radiography in the prostate, lung, colorectal, and ovarian cancer screening trial. Arch Intern Med. 2008;168:2326–32. doi: 10.1001/archinte.168.21.2326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Liang HY, Li XL, Yu XS, et al. Facts and fiction of the relationship between preexisting tuberculosis and lung cancer risk: a systematic review. Int J Cancer. 2009;125:2936–44. doi: 10.1002/ijc.24636. [DOI] [PubMed] [Google Scholar]
- 8.The effect of vitamin E and beta carotene on the incidence of lung cancer and other cancers in male smokers. The Alpha-Tocopherol, Beta Carotene Cancer Prevention Study Group. N Engl J Med. 1994;330:1029–35. doi: 10.1056/NEJM199404143301501. [DOI] [PubMed] [Google Scholar]
- 9.The alpha-tocopherol, beta-carotene lung cancer prevention study: design, methods, participant characteristics, and compliance. The ATBC Cancer Prevention Study Group. Ann Epidemiol. 1994;4:1–10. doi: 10.1016/1047-2797(94)90036-1. [DOI] [PubMed] [Google Scholar]
- 10.Korhonen P, Malila N, Pukkala E, et al. The Finnish Cancer Registry as follow-up source of a large trial cohort--accuracy and delay. Acta Oncol. 2002;41:381–8. doi: 10.1080/028418602760169442. [DOI] [PubMed] [Google Scholar]
- 11.Thurston SW, Liu G, Miller DP, Christiani DC. Modeling lung cancer risk in case-control studies using a new dose metric of smoking. Cancer Epidemiol Biomarkers Prev. 2005;14:2296–302. doi: 10.1158/1055-9965.EPI-04-0393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hemila H, Kaprio J, Pietinen P, Albanes D, Heinonen OP. Vitamin C and other compounds in vitamin C rich food in relation to risk of tuberculosis in male smokers. Am J Epidemiol. 1999;150:632–41. doi: 10.1093/oxfordjournals.aje.a010062. [DOI] [PubMed] [Google Scholar]
- 13.Littman AJ, Thornquist MD, White E, et al. Prior lung disease and risk of lung cancer in a large prospective study. Cancer Causes Control. 2004;15:819–27. doi: 10.1023/B:CACO.0000043432.71626.45. [DOI] [PubMed] [Google Scholar]
- 14.Park SK, Cho LY, Yang JJ, et al. Lung cancer risk and cigarette smoking, lung tuberculosis according to histologic type and gender in a population based case-control study. Lung cancer (Amsterdam, Netherlands) 2010;68:20–6. doi: 10.1016/j.lungcan.2009.05.017. [DOI] [PubMed] [Google Scholar]
- 15.Wang XR, Yu IT, Chiu YL, et al. Previous pulmonary disease and family cancer history increase the risk of lung cancer among Hong Kong women. Cancer Causes Control. 2009;20:757–63. doi: 10.1007/s10552-008-9289-4. [DOI] [PubMed] [Google Scholar]
- 16.Lan Q, Chapman RS, Schreinemachers DM, Tian L, He X. Household stove improvement and risk of lung cancer in Xuanwei, China. J Natl Cancer Inst. 2002;94:826–35. doi: 10.1093/jnci/94.11.826. [DOI] [PubMed] [Google Scholar]
- 17.Brownson RC, Alavanja MC. Previous lung disease and lung cancer risk among women (United States) Cancer Causes Control. 2000;11:853–8. doi: 10.1023/a:1008999202040. [DOI] [PubMed] [Google Scholar]
- 18.Koshiol J, Rotunno M, Consonni D, et al. Lower risk of lung cancer after multiple pneumonia diagnoses. Cancer Epidemiol Biomarkers Prev. 2010;19:716–21. doi: 10.1158/1055-9965.EPI-09-0873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mayne ST, Buenconsejo J, Janerich DT. Previous lung disease and risk of lung cancer among men and women nonsmokers. Am J Epidemiol. 1999;149:13–20. doi: 10.1093/oxfordjournals.aje.a009722. [DOI] [PubMed] [Google Scholar]
- 20.Sasco AJ, Secretan MB, Straif K. Tobacco smoking and cancer: a brief review of recent epidemiological evidence. Lung cancer (Amsterdam, Netherlands) 2004;45 (Suppl 2):S3–S9. doi: 10.1016/j.lungcan.2004.07.998. [DOI] [PubMed] [Google Scholar]
- 21.World Health Organization. A WHO/The Union monograph on TB and tobacco control: joining efforts to control two related global epidemics. Geneva, Switzerland: WHO Press; 2007. [Google Scholar]
- 22.Bates MN, Khalakdina A, Pai M, et al. Risk of tuberculosis from exposure to tobacco smoke: a systematic review and meta-analysis. Arch Intern Med. 2007;167:335–42. doi: 10.1001/archinte.167.4.335. [DOI] [PubMed] [Google Scholar]
- 23.Ballaz S, Mulshine JL. The potential contributions of chronic inflammation to lung carcinogenesis. Clin Lung Cancer. 2003;5:46–62. doi: 10.3816/CLC.2003.n.021. [DOI] [PubMed] [Google Scholar]