

Abstract
Focal myositis is a commonly referenced, infrequently reported and poorly documented benign inflammatory pseudotumour, which may be misdiagnosed as a malignant tumour. We report the clinicopathologic features in a case of focal myositis in the thigh of a 15-year-old boy.
Background
Focal myositis is a rare, benign, inflammatory pseudotumour of the skeletal muscle. Although it usually involves the extremities, it may occur in any skeletal muscle. Its clinical presentation and appearance may mimic a malignant neoplasm of soft tissue; it is important that physicians be aware of this benign entity. We report a case of focal myositis of the thigh muscle. The clinical features were compatible with a rhabdomyosarcoma, requiring investigation to correctly identify its benign aetiology.
Case presentation
A 15-year-old Iranian boy presented with a left-sided thigh mass and pain. The patient had noticed the mass approximately 1 week before presentation, and it had subsequently increased in size. There was pain in the affected region that was intermittent and sharp. There was no history of trauma to the affected thigh. On examination, the mass was firm and fixed. The remainder of the physical examination was normal. Laboratory investigations revealed an elevated creatinine kinase level (550 U/l) and erythrocyte sedimentation rate (20 mm/h). The C reactive protein and white cell count were normal. An MRI showed ill-defined large edematous mass-like lesion in vastus lateralis muscle in middle third of left thigh showing marked surrounded edema. Signal intensity of the mentioned lesion was non-homogeneous and multiple small hyposignal components were seen. The lesion extended to the outer cortex of femur, but no invasion or periosteal elevation was detected. Size of lesion was 10×3×3 cm and irregular non-homogeneous enhancement in mentioned mass was detected (figures 1 and 2). The clinical impression was rhabdomyosarcoma. Finally, an open biopsy was performed under general anaesthesia. Microscopic examination showed skeletal muscle infiltrated by aggregates of lymphocytes and plasma cells with occasional eosinophils and macrophages. The inflammation was associated with exuberant fibrocollagenous scar tissue, entrapping muscle bundles as well as focally extending between individual muscle fibres. Myofibres in the most affected areas showed evidence of degeneration, with variability in diameter and internal placement of the nuclei. Granulomas were not identified (figure 3). Biopsy results led to a diagnosis of focal myositis.
Figure 1.

MRI revealed well-defined lobulated isosignal mass lesion.
Figure 2.

Lobulated isosignal mass lesion seen in the magnetic resonance image of a cross section of left thigh.
Figure 3.
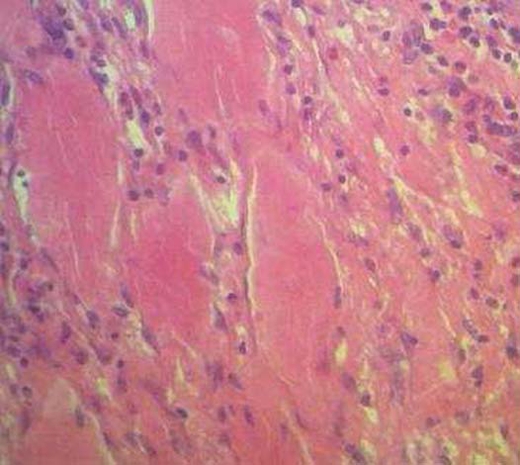
Section shows skeletal muscle fibres infiltrated by inflammatory cells.
Differential diagnosis
The diagnosis of focal myositis is one of exclusion and muscle biopsy is necessary to assess the presence of histopathologic features of inflammatory muscle disease and rule out neoplastic and ischaemic diseases.
Treatment
The patient received corticosteroids at a dose of 60 mg a day for 1 week, followed by tapering over an additional 1 month until discontinued.
Outcome and follow-up
The patient is in good condition after 5 months of follow-up.
Discussion
Focal myositis was first described in 1977 by Heffiner et al1 as a rare and heterogeneous disease diagnosed on clinical and pathological findings. It remains a diagnosis of exclusion. There is no age or sex prevalence.2 3 The cause is unknown, but some case have been related to inset bite,4 infection caused by Campylobacter species5 and immunisation.6 Focal myositis has not been associated with paraneoplastic phenomena, but foci of muscular inflammation around metastasis have been recently reported.7 It is reported to occur rarely in association with some inflammatory and connective tissue diseases.8 As in our patient, focal myositis most frequently affects the lower limbs, but any localisation can occur, and involvement of the arms, thorax, abdomen, neck and even tongue has been described.1 2 It may present as an enlarged and painful and sometimes symmetric mass of the skeletal muscle.1 It may affect one or more group of muscles, but rarely appears multifocal.9 The diagnosis of focal myositis is one of exclusion and muscle biopsy is necessary to assess the presence of histopathologic features of inflammatory muscle disease and rule out neoplastic and ischaemic diseases.3 10 Laboratory tests are of little intrinsic value because results usually are normal whether the disease is focal or multifocal. However, they will be useful to exclude other diseases. MRI provides a sensitive means to diagnose muscle inflammatory disorders, define the extension and assess disease activity.
Learning points.
-
▶
Focal myositis is a rare and heterogeneous disease.
-
▶
It is a diagnosis of exclusion.
-
▶
Muscle biopsy is necessary to assess the presence of histopathologic features of inflammatory muscle disease and rule out neoplasm and ischaemic disease.
Footnotes
Competing interests None.
Patient consent Obtained.
References
- 1.Heffiner RR, Jr, Armbrustmacher VW, Earle KM. Focal myositis. Cancer 1977;40:301–6 [DOI] [PubMed] [Google Scholar]
- 2.Flaisler F, Blin D, Asencio G, et al. Focal myositis: a localized form of polymyositis? J Rheumatol 1993;20:1414–16 [PubMed] [Google Scholar]
- 3.Smith AG, Urbanits S, Blaivas M, et al. Clinical and pathologic features of focal myositis. Muscle Nerve 2000;23:1569–75 [DOI] [PubMed] [Google Scholar]
- 4.Vatan R, Coquet M, Heraud A, et al. Biceps crural myositis after an insect bite. Rev Med Interne 2002;23:939–42 [DOI] [PubMed] [Google Scholar]
- 5.Dawson JK, Davidson JE. Focal myositis due to Campylobacter infection. Rheumatology (Oxford) 2001;40:704–6 [DOI] [PubMed] [Google Scholar]
- 6.Manganelli S, De Stefano R, Malandrini A, et al. Bilateral recurrent focal myositis of gastrocnemius muscles after BCG vaccination. Rheumatology (Oxford) 2002;41:1074–6 [DOI] [PubMed] [Google Scholar]
- 7.Uppal SS, Salopal TK, Singh H. Left gluteal focal myositis in a patient with signet ring adenocarcinoma of the stomach: not a paraneoplastic phenomenon. Rheumatol Int 2004;24:365–7 [DOI] [PubMed] [Google Scholar]
- 8.Alzagatiti BI, Bertorini TE, Horner LH, et al. Focal myositis presenting with radial nerve palsy. Muscle Nerve 1999;22:956–9 [DOI] [PubMed] [Google Scholar]
- 9.Revaz S, Theumann N, Lobrinus JA, et al. Leg pain due to bilateral focal recurrent myositis in a hemodialysis patient. Am J Kidney Dis 2005;45:E7–E11 [DOI] [PubMed] [Google Scholar]
- 10.Marie I, Hatron PY, Hachulla E, et al. Pulmonary involvement in polymyositis and in dermatomyositis. J Rheumatol 1998;25:1336–43 [PubMed] [Google Scholar]