

Abstract
A 55-year-old woman with human T-cell lymphotropic virus type-1 (HTLV-1)-associated adult T-cell leukemia (ATL) and a history of previously treated Strongyloides stercoralis infection received anti-CD52 monoclonal antibody therapy with alemtuzumab on a clinical trial. After an initial response, she developed ocular involvement by ATL. Alemtuzumab was stopped and high-dose corticosteroid therapy was started to palliate her ocular symptoms. Ten days later, the patient developed diarrhea, vomiting, fever, cough, skin rash, and a deteriorating mental status. She was diagnosed with disseminated S. stercoralis. Corticosteroids were discontinued and the patient received anthelmintic therapy with ivermectin and albendazole with complete clinical recovery.
Key Words: Adult T-cell leukemia, Alemtuzumab, Corticosteroid, Disseminated Strongyloides, HTLV-1, Human T-cell lymphotropic virus type-1
Introduction
Infection with human T-cell lymphotropic virus type-1 (HTLV-1) is associated with development of adult T-cell leukemia (ATL) [1]. HTLV-1 also predisposes patients to recurrent and severe infection with the nematode parasite Strongyloides stercoralis [2]. Patients with chronic Strongyloides infection are susceptible to the life-threatening complication of disseminated strongyloidiasis (DS) if treated with immunosuppressive therapy, in particular corticosteroids. We present here a case of this unusual but serious condition as a complication of therapy of ATL.
Case Report
A 55-year-old woman from Barbados diagnosed with HTLV-1-associated ATL was enrolled in a phase II trial of alemtuzumab (Campath™ anti-CD52) for ATL. Her past medical history was significant for S. stercoralis infection that had been diagnosed 6 years earlier by endoscopy after a 5-month history of vomiting and diarrhea. She had been treated with ivermectin. A serologic diagnosis of HTLV-1 infection was made at that time; however, there was no evidence of ATL. Four months later, she underwent a jejunal resection and a gastrojejunostomy for a partial small bowel obstruction. Six years later, she was empirically treated in Barbados with ivermectin for presumed strongyloidiasis after another bout of prolonged vomiting and diarrhea. No stool test was performed at that time. She responded clinically to the therapy. Later this same year, she was diagnosed with chronic ATL and enrolled in a clinical trial using daclizumab (humanized anti-CD25); however, her disease progressed.
She subsequently enrolled in another clinical trial and was treated with intravenous alemtuzumab. She received 30 mg three times weekly. Her circulating leukemic cell count promptly declined. However, after 10 weeks of treatment she developed decreased vision in her right eye. Ophthalmologic examination revealed a vitreous infiltrate. Vitreous biopsy and immunophenotyping of the vitreous infiltrate by flow cytometry revealed an aberrant T-cell population consistent with ATL. This was considered disease progression, and therefore the alemtuzumab was stopped and she was taken off the study. Daily oral dexamethasone 20 mg and prednisolone acetate 1% ophthalmic suspension were started as palliative treatment.
At a follow-up visit 10 days later, the patient complained of new onset watery diarrhea of up to 10 stools per day, and vomiting. She was found to have had a 2.7-kg weight loss and experienced an episode of near-syncope requiring hospital admission. She also complained of a pruritic rash on her abdomen and flank. On review of systems, the patient complained of a mild, dry cough, but no shortness of breath. She was afebrile, but tachycardic at 121 beats/min and had orthostatic hypotension. Pulse oximetry showed 96% saturation on room air. Pulmonary examination was notable for bibasilar rales. Her abdomen was soft and non-tender, without hepatosplenomegaly. An extensive petechial purpuric rash was noted on both flanks, extending to the mid-to-lower abdomen and thighs (fig. 1). Laboratory values showed a serum sodium of 125 mmol/l (reference range 135–145), potassium of 2.8 mmol/l (reference range 3.5–5.2), and a normal peripheral blood leukocyte count without eosinophilia. On direct smear of stool and sputum, numerous S. stercoralis larvae were seen. Computed tomographic (CT) scan of the chest showed patchy, ‘ground-glass’ infiltrates that had not been present 1 month previously. Blood cultures were negative for bacterial growth. A biopsy of the rash demonstrated Strongyloides larvae (fig. 2). Oral ivermectin 200 μg/kg once daily was initiated for DS.
Fig. 1.

Skin rash of disseminated Strongyloides.
Fig. 2.
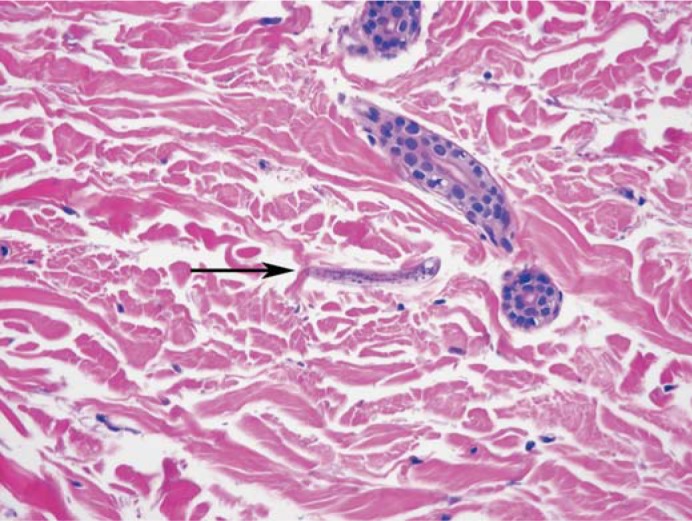
Strongyloides larva in skin.
One week later, the patient became acutely obtunded with a temperature of 39°C. She was hemodynamically stable with no focal neurological signs. Ivermectin was increased from 200 to 300 μg/kg/day and albendazole 400 mg twice daily via nasogastric tube was added, along with intravenous meropenem, vancomycin, ampicillin and acyclovir. CT scan of the brain was normal. Lumbar puncture and cerebrospinal fluid (CSF) analysis showed a total leukocyte count of 6,095 × 109/l cells with 98% neutrophils, with a protein concentration of 430 mg/dl (reference range 15–45) and glucose of 82 mg/dl (reference range 40–70) with a serum glucose of 236 mg/dl. Gram stain and bacterial culture, agar plate culture and a concentrated smear of CSF for Strongyloides larvae were all negative. CSF polymerase chain reaction for herpes simplex virus and human herpes virus-6, and a cryptococcal antigen test by EIA were negative. Repeat blood cultures showed no growth. Within 24 h, the patient became afebrile and her mental status improved. Repeat CSF analysis 2 days after the initial test showed the total leukocyte count decreased to 0.378 × 109/l cells with 93% neutrophils. Broad-spectrum antimicrobials were continued for 2 weeks and the patient's dexamethasone was tapered and discontinued. She remained on ivermectin and albendazole for 14 days after her stool examination was negative for Strongyloides for 5 consecutive days. This resulted in a total of 33 days of anthelmintic treatment.
At a follow-up visit 3 months later, the patient was well and without complaints, with normal stool and CSF studies. Ophthalmologic examination showed improvement in the vitreous infiltrate. Flow cytometry continued to demonstrate an aberrant T-cell population in the peripheral blood suspicious for ATL, but her total white count remained normal. Six months after discharge, the patient reported an episode of watery diarrhea, abdominal discomfort and mild dizziness that resolved after she was treated with ivermectin (200 μg/kg/day) by her local physician in Barbados. No stool studies were done at the time of the acute illness. Stool studies at the time of her follow-up visit were negative for larvae and other infectious causes of diarrhea. One year later, the patient was well with no intercurrent symptoms and her stool examination for Strongyloides was negative.
Discussion
S. stercoralis is an intestinal nematode endemic to the tropics and subtopics with worldwide estimates of prevalence varying from 30 to 100 million people. In developed countries such as the United States, there is growing recognition of Strongyloides as a parasite of significance among immigrants, travelers and refugees [3,4]. Chronic infection with S. stercoralis is frequently asymptomatic, although patients may complain of gastrointestinal symptoms such as diarrhea, abdominal pain, constipation and bloating, or have dermatologic findings, such as chronic urticaria or larva currens, a serpiginous rash located along the lower trunk, thighs or buttocks. Unusual manifestations include arthritis, nephrotic syndrome, chronic malabsorption, duodenal obstruction, focal hepatic lesions and asthma [5]. Hyperinfection syndrome (HIS) occurs when chronically infected individuals are administered corticosteroids, resulting in increased numbers of larvae and exacerbation of gastrointestinal and pulmonary symptoms [5]. DS occurs when large numbers of larvae migrate beyond from the gastrointestinal tract and lungs to ectopic sites such as the skin, as occurred in our patient [6]. The mortality associated with HIS or disseminated disease approaches 100% if untreated [5]. Death in patients with DS can result from Gram-negative or aseptic meningitis, bacteremia, or massive larval dissemination and hypovolemic shock [2].
Epidemiologic studies have shown that, in endemic areas, persons who are HTLV-1 seropositive have a significantly higher prevalence of S. stercoralis infection detected by stool examination compared to seronegative persons [2]. HTLV-1 coinfection plays a critical role in the development of HIS/DS by interfering with the immune response to S. stercoralis, most notably by decreasing the production of IL-4, IL-5, IL-13 and IgE in response to parasite antigens, resulting in an increase in autoinfection and decreased parasite killing [2]. Regulatory T-cell populations are also expanded in HTLV-1 and S. stercoralis coinfected individuals compared to persons infected with S. stercoralis alone suggesting another potential mechanism for decreased T-cell immunity to the parasite [7]. Consequently, HTLV-1 coinfected individuals are predisposed to more severe and recurrent strongyloidiasis. Decreased treatment efficacy is noted in these patients [2]. It is likely that our patient had persistent Strongyloides infection despite several treatments over a 6-year period, and that the episode of DS was a complication of this chronic infection.
Our patient was diagnosed with ATL many years after she developed the Strongyloides infection. Some studies have suggested that S. stercoralis infection promotes development of ATL in HTLV-1 infected individuals [8,9,10], but this hypothesis has been disputed on the grounds that ATL patients infected with Strongyloides have improved responses to chemotherapy [11], and HTVL-1 carriers coinfected with Strongyloides have a lower proviral loads than those with HTVL-1 alone [12].
Another major risk factor for the development of HIS/DS is the use of corticosteroids. Even a single dose of dexamethasone has been followed by the development of disseminated disease [13]. Other immunosuppressive drugs, including monoclonal antibodies such as alemtuzumab, have been implicated in the development of DS/HIS [14], although concurrent steroid use was associated with the majority of these cases, including our own.
The parasitological diagnosis of HIS/DS is usually straightforward because of the greatly increased parasite number, as larvae are easily found in stool or sputum, and have been incidentally found in blood smears, ascitic fluid, and bronchoalveolar lavage specimens [15]. Diagnosis of the chronically infected, asymptomatic individual, however, can be challenging, as adult parasites may produce only 10–15 eggs per day [16]. The sensitivity of a single, fresh stool specimen has been estimated to be as low as 30% [17]. Multiple stool specimens can increase the sensitivity [18]. Agar plate culture improves parasite detection considerably [19]. Aspiration of duodenal fluid for microscopic examination has been shown to be more sensitive (76%) than wet mount analysis of stool samples [20]. Serology by enzyme-linked immunosorbent assay (ELISA) based on crude larval antigen can be useful in excluding strongyloidiasis as part of the differential diagnosis. The sensitivity of this test has been determined to be ∼95% [21], although this is reduced in patients with hematologic malignancies [22]. Serology utilizing a recombinant Strongyloides antigen has the advantage of eliminating cross-reactivity with filarial infections [23].
For chronic strongyloidiasis, oral ivermectin 200 μg/kg/day for 1–2 days is the drug of choice based on its efficacy and tolerability [24]. Groups in whom empiric ivermectin would be relatively contraindicated include: pregnant or lactating women, children <1 year of age, or persons weighing <15 kg [5]. Alternatives include oral albendazole, 400 mg twice daily for 2–7 days, although albendazole has been associated with lower efficacy compared to ivermectin [25]. A few caveats for the presumptive treatment of Strongyloides exist. Ivermectin should not be used empirically in patients from Western and Central Africa at risk for Loa loa microfilaremia because of the potential for life-threatening encephalopathy in patients with blood microfilaria levels >5,000 microfilariae/ml [26]. The use of albendazole must similarly be weighed against the risk of exacerbating inflammatory reactions in patients with known neurocysticercosis, or in patients from neurocysticercosis-endemic regions with a seizure history of unknown etiology.
Regardless of treatment regimen, certain patients, such as those with HTLV-1 coinfection or hypogammaglobulinemia, have lower cure rates [2]. For this reason, these patients should be closely followed, as they remain at risk for the development of HIS/DS even after treatment. Currently, there is no test of cure for strongyloidiasis. Follow-up of patients after treatment with anthelmintics should routinely include multiple stool examinations to check for continued shedding of larvae. Resolution of peripheral eosinophilia has been observed in 90% of patients following treatment [24]. Although antibody levels typically persist after treatment, a decline in antibody levels has been noted in some patients 6 months after therapy [27,28].
Once HIS/DS develops, it is generally advisable to continue therapy for at least 2 weeks after three or more negative stool studies, or longer if the patient remains immunosuppressed [5]. In critically ill patients with hypoalbuminemia or paralytic ileus, it can be difficult to achieve adequate serum levels of ivermectin. Parenteral ivermectin has been administered under an Investigational New Drug exemption with demonstrated improvement in serum ivermectin concentrations, although its use has not been systematically studied [29]. Off-label rectal administration has been useful in some patients with severe diarrhea [30]. Combination therapy with albendazole and ivermectin has not been well studied.
Several questions remain unanswered in the management of Strongyloides infection. A critical issue relevant to oncologists is whether secondary prophylaxis prior to the initiation of immunosuppressive therapy can prevent development of HIS/DS in chronically infected individuals. Cases of HIS/DS have occurred even after treatment and documented clearance of Strongyloides larvae in stools of chronically infected individuals undergoing solid organ transplantation [31]. For this reason, extended or intermittent courses of anthelmintics have been advocated by some, although a prophylactic regimen has yet to be defined [32,33]. Screening of persons from endemic areas with serologic tests or repeated stool tests should occur prior to the initiation of immunosuppressive therapy. Infected individuals should be treated and monitored with serial stool examination and eosinophil counts post-treatment. HTLV-1 coinfected individuals should be considered at continued risk for HIS/DS despite anthelmintic treatment.
Conclusions
HTLV-1 infection, in addition to playing a causal role in the development of ATL, is a major risk factor for chronic S. stercoralis infection, and for the complications of hyperinfection and dissemination. Additional immunosuppressive therapy given to patients with HTLV-1 and S. stercoralis coinfection may trigger potentially fatal dissemination. Careful consideration should be given to these risks before administering steroids or other immunosuppressive therapy to such patients.
Acknowledgements
The authors gratefully acknowledge the assistance of Dr. Maria Turner, Dr. Rachel Bishop, and the clinical study staff (Melissa Law, Amara Pabon, Eunice Fox) at the National Institutes of Health for their help in caring for this patient. We additionally thank Dr. Thomas B. Nutman for his review of the manuscript.
This study was supported in part by the Intramural Research Program of the Center for Cancer Research, National Cancer Institute, and the National Institute of Allergy and Infectious Diseases, National Institutes of Health.
References
- 1.Tsukasaki K, Hermine O, Bazarbachi A, Ratner L, Ramos JC, Harrington W, Jr, O'Mahony D, Janik JE, Bittencourt AL, Taylor GP, Yamaguchi K, Utsunomiya A, Tobinai K, Watanabe T. Definition, prognostic factors, treatment, and response criteria of adult T-cell leukemia-lymphoma: a proposal from an international consensus meeting. J Clin Oncol. 2009;27:453–459. doi: 10.1200/JCO.2008.18.2428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Carvalho EM, Da Fonseca Porto A. Epidemiological and clinical interaction between HTLV-1 and Strongyloides stercoralis. Parasite Immunol. 2004;26:487–497. doi: 10.1111/j.0141-9838.2004.00726.x. [DOI] [PubMed] [Google Scholar]
- 3.Brodine SK, Thomas A, Huang R, Harbertson J, Mehta S, Leake J, Nutman T, Moser K, Wolf J, Ramanathan R, Burbelo P, Nou J, Wilkins P, Reed SL. Community-based parasitic screening and treatment of Sudanese refugees: application and assessment of Centers for Disease Control guidelines. Am J Trop Med Hyg. 2009;80:425–430. [PubMed] [Google Scholar]
- 4.Dawson-Hahn EE, Greenberg SL, Domachowske JB, Olson BG. Eosinophilia and the seroprevalence of schistosomiasis and strongyloidiasis in newly arrived pediatric refugees: an examination of Centers for Disease Control and Prevention screening guidelines. J Pediatr. 2010;156:1016–1018. doi: 10.1016/j.jpeds.2010.02.043. [DOI] [PubMed] [Google Scholar]
- 5.Ramanathan R, Nutman T. Strongyloides stercoralis infection in the immunocompromised host. Curr Infect Dis Rep. 2008;10:105–110. doi: 10.1007/s11908-008-0019-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Salluh JI, Bozza FA, Pinto TS, Toscano L, Weller PF, Soares M. Cutaneous periumbilical purpura in disseminated strongyloidiasis in cancer patients: a pathognomonic feature of potentially lethal disease? Braz J Infect Dis. 2005;9:419–424. doi: 10.1590/s1413-86702005000500010. [DOI] [PubMed] [Google Scholar]
- 7.Montes M, Sanchez C, Verdonck K, Lake JE, Gonzalez E, Lopez G, Terashima A, Nolan T, Lewis DE, Gotuzzo E, White AC., Jr Regulatory T-cell expansion in HTLV-1 and strongyloidiasis co-infection is associated with reduced IL-5 responses to Strongyloides stercoralis antigen. PLoS Negl Trop Dis. 2009;3:e456. doi: 10.1371/journal.pntd.0000456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nakada K, Yamaguchi K, Furugen S, Nakasone T, Nakasone K, Oshiro Y, Kohakura M, Hinuma Y, Seiki M, Yoshida M, Matutes E, Catovsky D, Ishii T, Takatsuki K. Monoclonal integration of HTLV-1 proviral DNA in patients with strongyloidiasis. Int J Cancer. 1987;40:145–148. doi: 10.1002/ijc.2910400203. [DOI] [PubMed] [Google Scholar]
- 9.Satoh M, Toma H, Sugahara K, Etoh K, Shiroma Y, Kiyuna S, Takara M, Matsuoka M, Yamaguchi K, Nakada K, Fujita K, Kojima S, Hori E, Tanaka Y, Kamihira S, Sato Y, Watanabe T. Involvement of IL-2/IL-2R system activation by parasite antigen in polyclonal expansion of CD4+25+ HTLV-1-infected T cells in human carriers of both HTLV-1 and S. stercoralis. Oncogene. 2002;21:2466–2475. doi: 10.1038/sj.onc.1205329. [DOI] [PubMed] [Google Scholar]
- 10.Ratner L, Grant C, Zimmerman B, Fritz J, Weil G, Denes A, Suresh R, Campbell N, Jacobson S, Lairmore M. Effect of treatment of Strongyloides infection on HTLV-1 expression in a patient with adult T-cell leukemia. Am J Hematol. 2007;82:929–931. doi: 10.1002/ajh.20929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Agape P, Copin MC, Cavrois M, Panelatti G, Plumelle Y, Ossondo-Landeau M, Quist D, Grossat N, Gosselin B, Fenaux P, Wattel E. Implication of HTLV-I infection, strongyloidiasis, and P53 overexpression in the development, response to treatment, and evolution of non-Hodgkin's lymphomas in an endemic area (Martinique, French West Indies) J Acquir Immune Defic Syndr Hum Retrovirol. 1999;20:394–402. doi: 10.1097/00042560-199904010-00011. [DOI] [PubMed] [Google Scholar]
- 12.Porto AF, Santos SB, Muniz AL, Basilio V, Rodrigues W, Jr, Neva FA, Dutra WO, Gollob KJ, Jacobson S, Carvalho EM. Helminthic infection down-regulates type 1 immune responses in human T-cell lymphotropic virus type 1 (HTLV-1) carriers and is more prevalent in HTLV-1 carriers than in patients with HTLV-1-associated myelopathy/tropical spastic paraparesis. J Infect Dis. 2005;191:612–618. doi: 10.1086/427560. [DOI] [PubMed] [Google Scholar]
- 13.Thomas MC, Costello SA. Disseminated strongyloidiasis arising from a single dose of dexamethasone before stereotactic radiosurgery. Int J Clin Pract. 1998;52:520–521. [PubMed] [Google Scholar]
- 14.Qazilbash MH, Ueno NT, Hosing C, De Lima M, Cortes J, Massaro A, Rivera Z, Deavers M, Adachi JA, Champlin RE. Strongyloidiasis after unrelated nonmyeloablative allogeneic stem cell transplantation. Bone Marrow Transplant. 2006;38:393–394. doi: 10.1038/sj.bmt.1705448. [DOI] [PubMed] [Google Scholar]
- 15.Keiser PB, Nutman TB. Strongyloides stercoralis in the immunocompromised population. Clin Microbiol Rev. 2004;17:208–217. doi: 10.1128/CMR.17.1.208-217.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Genta RM. Dysregulation of strongyloidiasis: a new hypothesis. Clin Microbiol Rev. 1992;5:345–355. doi: 10.1128/cmr.5.4.345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Siddiqui AA, Berk SL. Diagnosis of Strongyloides stercoralis infection. Clin Infect Dis. 2001;33:1040–1047. doi: 10.1086/322707. [DOI] [PubMed] [Google Scholar]
- 18.Pelletier LL., Jr Chronic strongyloidiasis in World War II Far East ex-prisoners of war. Am J Trop Med Hyg. 1984;33:55–61. doi: 10.4269/ajtmh.1984.33.55. [DOI] [PubMed] [Google Scholar]
- 19.Hirata T, Nakamura H, Kinjo N, Hokama A, Kinjo F, Yamane N, Fujita J. Increased detection rate of Strongyloides stercoralis by repeated stool examinations using the agar plate culture method. Am J Trop Med Hyg. 2007;77:683–684. [PubMed] [Google Scholar]
- 20.Goka AK, Rolston DD, Mathan VI, Farthing MJ. Diagnosis of Strongyloides and hookworm infections: comparison of faecal and duodenal fluid microscopy. Trans R Soc Trop Med Hyg. 1990;84:829–831. doi: 10.1016/0035-9203(90)90098-y. [DOI] [PubMed] [Google Scholar]
- 21.Loutfy MR, Wilson M, Keystone JS, Kain KC. Serology and eosinophil count in the diagnosis and management of strongyloidiasis in a non-endemic area. Am J Trop Med Hyg. 2002;66:749–752. doi: 10.4269/ajtmh.2002.66.749. [DOI] [PubMed] [Google Scholar]
- 22.Schaffel R, Nucci M, Carvalho E, Braga M, Almeida L, Portugal R, Pulcheri W. The value of an immunoenzymatic test (enzyme-linked immunosorbent assay) for the diagnosis of strongyloidiasis in patients immunosuppressed by hematologic malignancies. Am J Trop Med Hyg. 2001;65:346–350. doi: 10.4269/ajtmh.2001.65.346. [DOI] [PubMed] [Google Scholar]
- 23.Ramanathan R, Burbelo PD, Groot S, Iadarola MJ, Neva FA, Nutman TB. A luciferase immunoprecipitation systems assay enhances the sensitivity and specificity of diagnosis of Strongyloides stercoralis infection. J Infect Dis. 2008;198:444–451. doi: 10.1086/589718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Gann PH, Neva FA, Gam AA. A randomized trial of single- and two-dose ivermectin versus thiabendazole for treatment of strongyloidiasis. J Infect Dis. 1994;169:1076–1079. doi: 10.1093/infdis/169.5.1076. [DOI] [PubMed] [Google Scholar]
- 25.Marti H, Haji HJ, Savioli L, Chwaya HM, Mgeni AF, Ameir JS, Hatz C. A comparative trial of a single-dose ivermectin versus three days of albendazole for treatment of Strongyloides stercoralis and other soil-transmitted helminth infections in children. Am J Trop Med Hyg. 1996;55:477–481. doi: 10.4269/ajtmh.1996.55.477. [DOI] [PubMed] [Google Scholar]
- 26.Twum-Danso NA. Loa loa encephalopathy temporally related to ivermectin administration reported from onchocerciasis mass treatment programs from 1989 to 2001: implications for the future. Filaria J. 2003;2(suppl 1):S7. doi: 10.1186/1475-2883-2-S1-S7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Karunajeewa H, Kelly H, Leslie D, Leydon J, Saykao P, Biggs BA. Parasite-specific IgG response and peripheral blood eosinophil count following albendazole treatment for presumed chronic strongyloidiasis. J Travel Med. 2006;13:84–91. doi: 10.1111/j.1708-8305.2006.00004.x. [DOI] [PubMed] [Google Scholar]
- 28.Page WA, Dempsey K, McCarthy JS. Utility of serological follow-up of chronic strongyloidiasis after anthelminthic chemotherapy. Trans R Soc Trop Med Hyg. 2006;100:1056–1062. doi: 10.1016/j.trstmh.2005.12.006. [DOI] [PubMed] [Google Scholar]
- 29.Turner SA, Maclean JD, Fleckenstein L, Greenaway C. Parenteral administration of ivermectin in a patient with disseminated strongyloidiasis. Am J Trop Med Hyg. 2005;73:911–914. [PubMed] [Google Scholar]
- 30.Boken DJ, Leoni PA, Preheim LC. Treatment of Strongyloides stercoralis hyperinfection syndrome with thiabendazole administered per rectum. Clin Infect Dis. 1993;16:123–126. doi: 10.1093/clinids/16.1.123. [DOI] [PubMed] [Google Scholar]
- 31.Roxby AC, Gottlieb GS, Limaye AP. Strongyloidiasis in transplant patients. Clin Infect Dis. 2009;49:1411–1423. doi: 10.1086/630201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Santiago M, Leitao B. Prevention of Strongyloides hyperinfection syndrome: a rheumatological point of view. Eur J Intern Med. 2009;20:744–748. doi: 10.1016/j.ejim.2009.09.001. [DOI] [PubMed] [Google Scholar]
- 33.Peters L, McCarthy AE, Faught C. Secondary Strongyloides stercoralis prophylaxis in patients with human T-cell lymphotropic virus type 1 infection: report of two cases. Int J Infect Dis. 2009;13:e501–e503. doi: 10.1016/j.ijid.2009.02.009. [DOI] [PubMed] [Google Scholar]