

Abstract
Objective
The purpose of this case report is to describe the chiropractic management of a patient with Ménière disease.
Clinical Features
A 40-year-old woman presented with a diagnosis of Ménière disease including a 2-month history of vertigo and a 16-month history of left-sided tinnitus, low-frequency hearing loss, and aural fullness. The patient's other symptoms included left-sided neck pain, temporomandibular joint pain, and headaches. Examination revealed left-sided upper cervical joint dysfunction along with myofascial trigger points in the middle and upper trapezius muscle.
Intervention and Outcome
Treatment included primarily high-velocity, low-amplitude spinal manipulation to the upper cervical and thoracic spine, along with soft-tissue trigger-point therapy, and stretching exercises. Within 2 weeks of treatment, the patient's tinnitus had resolved; and all other symptoms (including vertigo) were improved. The patient's headaches, neck pain, and vertigo were subsequently resolved within 3 months of treatment. The patient experienced only 2 minor episodes of self-resolving “light-headedness” over that time. After 2½ years of follow-up, any occasional episodes of mild aural fullness and/or light-headedness are either self-resolving or relieved with cervical spinal manipulation and soft-tissue treatment.
Conclusion
This case report suggests that chiropractic care, including upper cervical spinal manipulation and soft-tissue therapy, may be beneficial in treating some patients with Ménière disease.
Key indexing terms: Ménière disease, Vertigo, Temporomandibular joint, Chiropractic, Spinal manipulation
Introduction
Prosper Ménière1 first described Ménière disease (MD) in 1861 as a syndrome characterized by hearing loss, tinnitus, and episodic vertigo. In 1938, endolymphatic hydrops—thought to be the principal underlying pathology of MD—was described by Hallpike and Cairns2; however, the precise etiology still remains controversial.3-5 The prevalence of MD is estimated to be 100 cases per 100 000, as studied in the United Kingdom.6 MD primarily affects white people, both sexes equally, and has a peak onset between 20 and 50 years of age.6
MD is typically diagnosed clinically from the classic triad of symptoms including recurrent and spontaneous vertigo, hearing loss, and tinnitus/sensation of aural fullness.7 The vertigo attacks vary in severity, last from several minutes to several hours, and are often accompanied by nausea.8 Patients with MD typically experience remissions and exacerbations.9 The disease can also stabilize, where the vertigo attacks disappear, or at least diminish over time. However, patients with MD can still have severe symptoms of dizziness even after a 20-year disease history.10
Medical treatment of MD has historically been empirical,3 and the evidence base for its management is limited.11 In a review by Saeed,3 he states, “As yet, no treatment has prospectively modified the clinical course of the condition and thereby prevented the progressive hearing loss.” The traditional medical management of MD has primarily been directed at controlling the vertigo attacks.12 Interestingly, several chiropractic studies have shown improvement in patients with vertigo symptoms when treated for upper cervical spine and temporomandibular joint (TMJ) dysfunction.13-17 There may be a relationship between MD and cervicogenic vertigo (CV), a condition chiropractors often diagnose and treat. The purpose of this case report is to describe the chiropractic management of a patient with MD.
Case report
A 40-year-old white female presented with a 2-month history of vertigo, along with left-sided hearing loss and tinnitus of 16 months' duration. The tinnitus was described as a loud “ringing tone” mixed with a sensation of “swooshing” or fullness in the left ear. The patient's symptoms also included chronic, left-sided neck and TMJ pain, along with intermittent headaches. The pain severity for each was graded as a 6.5 on a numeric rating scale of 10 and was typically worse toward the end of the day. Use of a dental bite splint over the past 3 years provided only mild relief of the headaches and TMJ pain. The vertigo attacks occurred monthly and would each last for approximately 3 hours. The vertigo was described as if the room was spinning in a slow, clockwise motion, while the patient's eyes involuntarily moved repeatedly back and forth (ie, nystagmus). During a vertigo attack, rotating the neck to either side aggravated the neck and TMJ pain, headache, vertigo, and nausea symptoms. Sitting down with the head flexed between the knees was the only palliative position.
The patient had originally presented to her family physician for evaluation of the left-sided aural fullness, tinnitus, and hearing loss. A referral was made to a hearing clinic for audiometric testing, which revealed a mild, low-frequency hearing loss and difficulty with speech discrimination on the left. A few months later, the patient experienced her first vertigo attack, which prompted a return to her family physician. The patient was diagnosed with MD and prescribed a vestibular suppressant for the vertigo. Instead of filling the prescription, the patient visited a naturopath for treatment. After another bout of vertigo and nonresolution of the MD symptoms, the patient presented for chiropractic assessment.
Examination including DeKlyn Test (ie, neck held in extension and rotation for 30 seconds) did not produce nystagmus or dizziness. Blood pressure was normal at 106/62. Postural examination revealed a high left shoulder and forward head carriage. Motion palpation of the spine revealed joint restriction at C2-3 in right rotation, T1-2 in left rotation, and T5-6 in extension. Static palpation of the neck revealed localized tenderness of the left C2-3 joint and a large myofascial trigger point within the left middle trapezius muscle. Cervical spine range of motion (ROM) was restricted and mildly painful in extension. Depression of the left shoulder while holding the neck in flexion and right rotation (ie, Shoulder Depression Test) produced some left upper trapezius pain. Upper extremity neurologic examination was unremarkable for motor, reflex, and sensory testing. Cranial nerve examination was normal. Cervical spine radiographs revealed mild-to-moderate discogenic spondylosis at C5-6. The patient was diagnosed with left-sided cervicogenic headache and vertigo, with underlying degenerative disk disease at C5-6. This diagnosis was secondary to the patient's primary diagnosis of MD.
The patient underwent a course of chiropractic treatment consisting of spinal manipulative therapy (SMT) to the cervical (Fig 1A) and thoracic spine, soft-tissue trigger-point therapy to the left middle and upper trapezius muscle (Fig 1B), home ice therapy (as needed), and cervical spine rehabilitation exercises (Figs 2 and 3). The initial treatment frequency was 3 times per week for 2 weeks. Outcome measures used were numeric rating scale for pain; the number and severity of acute vertigo attacks and headaches; and subjective changes in hearing, tinnitus, and perception of aural fullness. Objective measures used were visual estimation for ROM and orthopedic examination.
Fig 1.
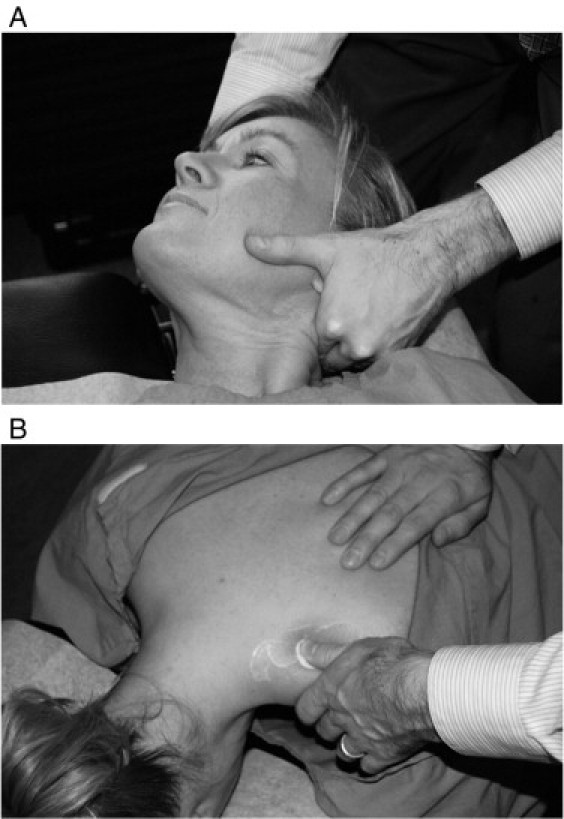
Cervical SMT (A). Soft-tissue trigger-point therapy (B).
Fig 2.
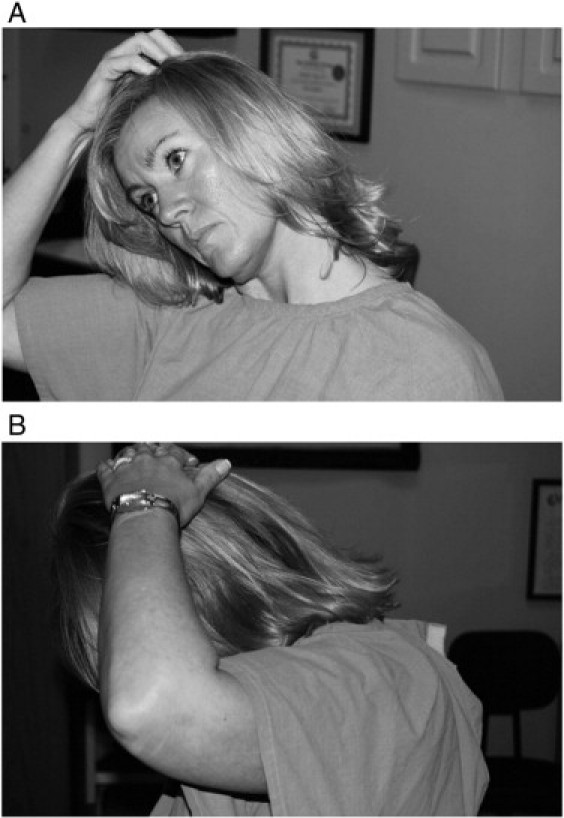
Cervical spine scalene (A) and paraspinal stretches (B) (each held for 15 seconds); 2 repetitions, 1 to 2 sets per day.
Fig 3.
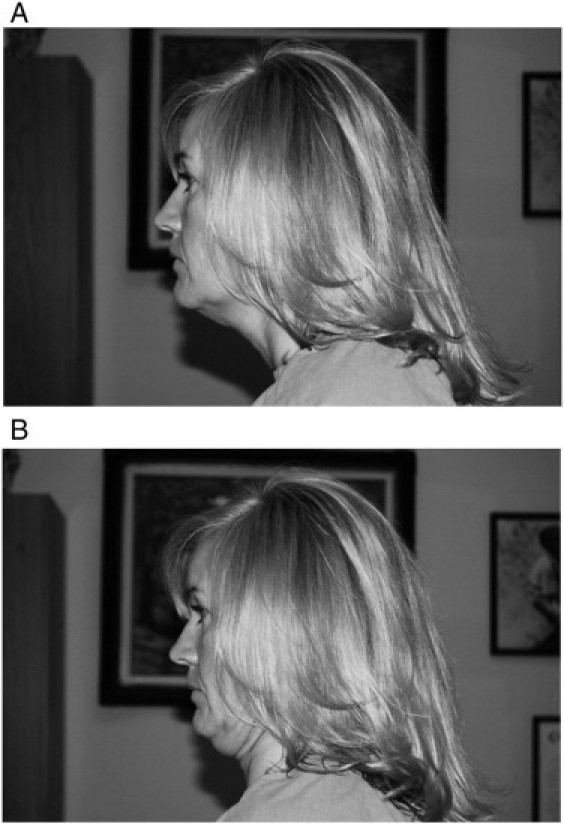
Cervical spine retraction exercise showing protraction (A) and retraction (B) (held for 6 seconds); 3 repetitions, 1 to 2 sets per day.
After 2 weeks of treatment, the patient's TMJ pain and clicking, headache frequency and intensity, and vertiginous symptoms had improved; and the tinnitus had resolved. The neck pain and TMJ pain were each reduced to 2 out of 10. Objectively, cervical ROM was within normal limits; and the result of the Shoulder Depression Test was negative. Based on these improvements, the treatment frequency progressively decreased to once every 3 weeks. At 3-month follow-up and after a total of 12 treatments, the left-sided neck pain, headaches, and vertigo were resolved. Only 2 minor episodes of “light-headedness” (ie, not vertigo and lasting only a few minutes) were reported.
After 2½ years, the patient continues to experience occasional symptoms of aural fullness or mild light-headedness (without vertigo) about 2 to 3 times per year. She also experiences intermittent neck and shoulder pain, likely as a result of postural strain from sitting at work at a computer. These symptoms are all typically mild and are either self-resolving or relieved with manipulation and soft-tissue trigger-point therapy. In addition, the patient continues to report that she has not used any prescription or over-the-counter medications during the entire course of treatment. The patient has given written consent to having her personal health information, including photographs of her likeness, published.
Discussion
The central medical hypothesis for the etiology of MD is bound to endolymphatic hydrops—thought to be responsible for the classic symptoms of MD (ie, episodic vertigo, tinnitus/aural fullness, and sensorineural hearing loss). Endolymphatic hydrops is caused by impaired filtration and excretion of endolymph within the inner ear leading to a buildup of fluid. This endolymphatic buildup results in distension of the endolymphatic compartment, thereby leading to vestibulocochlear dysfunction.2,18
Conventional medical treatment
The traditional medical management of MD is primarily designed to lower endolymphatic pressure. A low-salt diet (ie, less than 1 to 2 g of salt per day) and diuretics (ie, most commonly the combination of hydrochlorothiazide and triamterene) are commonly prescribed.19,20 However, in a recent Cochrane review,11 the authors concluded that “there is no good evidence for or against the use of diuretics in [MD] or syndrome” and recommended further research. For patients who do not respond to diet and diuretic treatment, oral steroid or intratympanic steroid injection can be attempted.21 In patients with intractable vertigo, transtympanic perfusion with gentamicin can be used. Gentamicin, an aminoglycoside, directly destroys the epithelial cells in the cochlea and the labyrinth.21 This treatment provides good control of patients' vertigo; and when administered in lower doses, the risk of hearing loss can be reduced.22,23 Other surgical procedures such as endolymphatic sac surgery, vestibular nerve section, or labyrinthectomy are usually reserved for the most severe, unresponsive cases of MD.3,12
Nonconventional treatment
In contrast to the traditional medical approach, Bjorne et al24-26 have studied the association between patients with MD, and concomitant TMJ and cervical spine disorders. In successive studies,24,25 they found a much higher prevalence of signs and symptoms of craniomandibular and cervical spine disorders, respectively, in patients diagnosed with MD compared with controls.
The MD patients from the 2 aforementioned studies participated in a 3-year longitudinal study involving “coordinated treatment” of their TMJ and cervical spine disorders.26 The treatment consisted of a range of therapies including education; stress, relaxation, and postural training; stretching exercises; periodontal grinding; custom bite splints; lidocaine injections; and physiotherapy. The study results showed significant, simultaneous improvements (throughout the 3-year follow-up) for all MD symptoms, as well as neck/shoulder, jaw, and headache pain. The researchers concluded that MD has a clear association with TMJ and cervical spine disorders. However, this study was not a randomized, controlled trial; therefore, more research is warranted to provide further evidence of this association.
A recent review by Long et al27 investigated the evidence for acupuncture as a treatment of MD. The overall conclusion by the authors was that there is “potential benefit” of acupuncture for patients with MD. However, further research is needed, particularly in a Western health care context.
Chiropractic care
Research involving chiropractic treatment of MD is extremely scarce. Only 2 studies, both involving “upper cervical specific” treatment, were found in PubMed and Index to Chiropractic Literature relating chiropractic care and MD.28,29 Kessinger and Boneva28 reported on a chiropractic patient treated for symptoms “consistent with [MD].” Their patient had a longstanding history of vertigo, tinnitus, and hearing loss, which had progressively worsened 5 weeks before presenting for care. The patient's vertigo symptoms were alleviated within the first few weeks, and her hearing improved (as measured by audiometric testing) after 13 weeks of care. The patient was treated on each office visit with an upper cervical, toggle-type SMT. In a case series, Burcon29 treated 10 patients diagnosed with MD (9 of whom had a history of neck trauma). All 10 patients also responded favorably to upper cervical, toggle SMT (reportedly within the first few treatment visits). However, this study lacks rigorous outcome measures; therefore, the results need to be interpreted judiciously.
Other studies have investigated the effectiveness of chiropractic treatment for patients with CV.13-17 In a review by Hawk et al,14 they conclude that there is evidence from both controlled studies and usual practice that is adequate to support the “total package” of chiropractic care, including SMT and other procedures, as providing benefit to patients with CV (among other conditions). Fitz-Ritson17 explains that cervical spine trauma (eg, whiplash) can damage the proprioceptors of the neck muscles, joints, and tendons. This damage changes the afferent input into the spinal cord and brainstem nuclei, which may result in CV. Therefore, treatment of the neck and TMJ (ie, SMT and soft-tissue therapy) can restore the normal afferent input from the neck proprioceptors, thereby decreasing vertigo symptoms.
TMJ and cervical spine
Disease symptoms involving the TMJ and cervical spine often overlap.30,31 In a series of articles written by a dental physicist,32-34 he found that the functional center of rotation of the mandible and TMJ exists at a point between the atlas and axis. According to this theorem, mandibular dysfunction (eg, abnormal dental occlusion) can result in mechanical stress to not only the TMJ, but the upper cervical spine as well. Fink et al30 showed that imbalanced dental occlusion in healthy subjects resulted in upper cervical (C0-C3) joint dysfunction/hypomobility. They also found the same relationship between dental occlusion and the sacroiliac joint.
In some cases, treatment of the TMJ results in improvement of the cervical spine, and vice versa. In a retrospective study, Steigerwald et al31 investigated a group of 43 patients who had undergone arthroscopic surgery for arthrogenous TMJ dysfunction. Ninety-five percent of respondents reported statistically significant levels of symptom reduction for neck pain, shoulder pain, and headaches, as well as symptoms of tinnitus and dizziness. Alcantara et al35 reported on a 41-year-old patient who experienced complete remission of her TMJ symptoms after 9 SMT treatments to the upper cervical spine. Interestingly, this patient also experienced improvement with other symptoms including tinnitus, vertigo, hearing difficulty, and headaches. Blum36 reported on a patient with tinnitus who also improved with chiropractic care.
Therefore, the scientific literature supports a functional relationship between disorders of the cervical spine and TMJ. The literature also supports the use of nonconventional therapy (including upper cervical SMT) in the treatment of TMJ pain, as well as other MD symptoms such as tinnitus, vertigo, and/or dizziness.
Limitations
Single case studies do not provide conclusive evidence for treatment effectiveness. The natural course of MD often includes remissions and exacerbations. Therefore, the patient in this case may have improved without treatment. In addition, rigorous outcome measures (eg, Dizziness Handicap Inventory, Neck Disability Index, and Headache Disability Index) were lacking in this study. Subjective changes in hearing, tinnitus, and aural fullness were also used rather than audiometric reevaluation. Any future studies of chiropractic treatment of MD should include more rigorous outcome measures.
Conclusion
Presented here was a patient with MD that responded very favorably to chiropractic care. In light of the paucity of research in the chiropractic literature reporting on the treatment of MD, more studies are needed to determine whether chiropractic care, including cervical SMT, is an effective alternative treatment for patients with MD. Chiropractic physicians may have a significant role to play in treating MD symptoms, such as vertigo and tinnitus, due primarily to the success reported in the literature on treating patients with CV and TMJ disorders. Again, however, more research is necessary to determine the link, if any, between these conditions and MD.
Funding sources and conflicts of interest
No funding sources or conflicts of interest were reported for this study.
Acknowledgment
The author thanks Carolyn Simolo and the staff at the New York Chiropractic College Library for their assistance in retrieving reference articles for this paper.
References
- 1.Ménière P. Pathologie auriculaeire: mémoires sur des lésions de l'oreille interne donnant lieu à des symptoms des congestion cérébrale apoplectiforme. Gaz Med Paris. 1861;16:597–601. [Google Scholar]
- 2.Hallpike C.S., Cairns H. Observations on the pathology of Ménière's syndrome. J Laryngol Otol. 1938;53:625–655. doi: 10.1177/003591573803101112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Saeed S.R. Fortnightly review. Diagnosis and treatment of Ménière's disease. BMJ. 1998;316:368–372. doi: 10.1136/bmj.316.7128.368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mancini F., Catalini M., Carru M., Monti B. History of Ménière's disease and its clinical presentation. Otolaryngol Clin North Am. 2002;35:565–580. doi: 10.1016/s0030-6665(02)00017-8. [DOI] [PubMed] [Google Scholar]
- 5.Merchant S.N., Adams J.C., Nadol J.B., Jr Pathophysiology of Ménière's syndrome: are symptoms caused by endolymphatic hydrops? Otol Neurotol. 2005;26:74–81. doi: 10.1097/00129492-200501000-00013. [DOI] [PubMed] [Google Scholar]
- 6.Morrison A.W. Anticipation in Ménière's disease. J Laryngol Otol. 1995;109:499–502. doi: 10.1017/s0022215100130567. [DOI] [PubMed] [Google Scholar]
- 7.Monsell E.M., Balkany T.A., Gates G.A., Goldenberg R.A., Meyerhoff W.L., House J.W. Committee on Hearing and Equilibrium guidelines for the diagnosis and evaluation of therapy in Ménière's disease. American Academy of Otolaryngology Head and Neck Foundation, Inc. Otolaryngol Head Neck Surg. 1995;113:181–185. doi: 10.1016/S0194-5998(95)70102-8. [DOI] [PubMed] [Google Scholar]
- 8.Pearson B.W., Brackmann D.E. Committee on Hearing and Equilibrium guidelines for reporting treatment results in Ménière's disease. Otolaryngol Head Neck Surg. 1985;93:579–581. doi: 10.1177/019459988509300501. [DOI] [PubMed] [Google Scholar]
- 9.Green J.D., Jr, Blum D.J., Harner S.G. Longitudinal follow-up of patients with Ménière's disease. Otolaryngol Head Neck Surg. 1991;104:783–788. doi: 10.1177/019459989110400603. [DOI] [PubMed] [Google Scholar]
- 10.Havia M., Kentala E. Progression of symptoms of dizziness in Ménière's disease. Arch Otolaryngol Head Neck Surg. 2004;130:431–435. doi: 10.1001/archotol.130.4.431. [DOI] [PubMed] [Google Scholar]
- 11.Thirlwall A., Kundu S. Diuretics for Ménière's disease or syndrome. Cochrane Database Syst Rev. 2006;(3) doi: 10.1002/14651858.CD003599.pub2. Art. No.:CD003599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Swartz R., Longwell P. Treatment of vertigo. Am Fam Physician. 2005;71:1115–1122. [PubMed] [Google Scholar]
- 13.Côté P., Mior S.A., Fitz-Ritson D. Cervicogenic vertigo: a report of three cases. J Can Chiropr Assoc. 1991;35:89–94. [Google Scholar]
- 14.Hawk C., Khorsan R., Lisi A.J., Ferrance R.J., Evans M.W. Chiropractic care for nonmusculoskeletal conditions: a systematic review with implications for whole systems research. J Altern Complement Med. 2007;13:491–512. doi: 10.1089/acm.2007.7088. [DOI] [PubMed] [Google Scholar]
- 15.Bracher E.S., Almeida C.I., Almeida R.R., Duprat A.C., Bracher C.B. A combined approach for the treatment of cervical vertigo. J Manipulative Physiol Ther. 2000;23:96–100. [PubMed] [Google Scholar]
- 16.Collins M.E., Misukanis T.M. Chiropractic management of a patient with post traumatic vertigo of complex origin. J Chiropr Med. 2005;4:32–38. doi: 10.1016/S0899-3467(07)60110-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Fitz-Ritson D. Assessment of cervicogenic vertigo. J Manipulative Physiol Ther. 1991;14:193–198. [PubMed] [Google Scholar]
- 18.Paparella M.M. Pathogenesis and pathophysiology of Ménière's disease. Acta Otolaryngol Suppl. 1991;485:26–35. doi: 10.3109/00016489109128041. [DOI] [PubMed] [Google Scholar]
- 19.Van Deelen G.W., Huizing E.H. Use of a diuretic (Dyazide) in the treatment of Ménière's disease. A double-blind cross-over placebo-controlled study. ORL J Otorhinolayngol Relat Spec. 1986;48:287–292. doi: 10.1159/000275884. [DOI] [PubMed] [Google Scholar]
- 20.Santos P.M., Hall R.A., Snyder J.M., Hughes L.F., Dobie R.A. Diuretic and diet effect on Ménière's disease evaluated by the 1985 Committee on Hearing and Equilibrium guidelines. Otolaryngol Head Neck Surg. 1993;109:680–689. doi: 10.1177/019459989310900408. [DOI] [PubMed] [Google Scholar]
- 21.Sajjadi H., Paparella M.M. Ménière's disease. Lancet. 2008;372:406–414. doi: 10.1016/S0140-6736(08)61161-7. [DOI] [PubMed] [Google Scholar]
- 22.Nedzelski J.M., Bryce G.E., Pfleiderer A.G. Treatment of Ménière's disease with topical gentamicin: a preliminary report. J Otolaryngol. 1992;21:95–101. [PubMed] [Google Scholar]
- 23.Driscoll C.L., Kasperbauer J.L., Facer G.W., Harner S.G., Beatty C.W. Low-dose intratympanic gentamicin and the treatment of Ménière's disease: preliminary results. Laryngoscope. 1997;107:83–89. doi: 10.1097/00005537-199701000-00017. [DOI] [PubMed] [Google Scholar]
- 24.Bjorne A., Agerberg G. Craniomandibular disorders in patients with Ménière's disease: a controlled study. J Orofac Pain. 1996;10:28–37. [PubMed] [Google Scholar]
- 25.Bjorne A., Berven A., Agerberg G. Cervical signs and symptoms in patients with Ménière's disease: a controlled study. Cranio. 1998;16:194–202. doi: 10.1080/08869634.1998.11746057. [DOI] [PubMed] [Google Scholar]
- 26.Bjorne A., Agerberg G. Symptom relief after treatment of temporomandibular and cervical spine disorders in patients with Ménière's disease: a three-year follow-up. Cranio. 2003;21:50–60. doi: 10.1080/08869634.2003.11746232. [DOI] [PubMed] [Google Scholar]
- 27.Long A.F., Xing M., Morgan K., Brettle A. Exploring the evidence base for acupuncture in the treatment of Ménière's syndrome—a systematic review. Evid Based Complement Alternat Med. 2009 doi: 10.1093/ecam/nep047. [Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kessinger R.C., Boneva D.V. Vertigo, tinnitus, and hearing loss in the geriatric patient. J Manipulative Physiol Ther. 2000;23:352–362. [PubMed] [Google Scholar]
- 29.Burcon M. Upper cervical protocol to reduce vertebral subluxation in ten subjects with Ménières: a case series. J Vertebral Subluxation Res. 2008;2:1–8. [Google Scholar]
- 30.Fink M., Wähling K., Stiesch-Scholz M., Tschernitschek H. The functional relationship between the craniomandibular system, cervical spine, and the sacroiliac joint: a preliminary investigation. Cranio. 2003;21:202–208. doi: 10.1080/08869634.2003.11746252. [DOI] [PubMed] [Google Scholar]
- 31.Steigerwald D.P., Verne S.V., Young D. A retrospective evaluation of the impact of temporomandibular joint arthroscopy on the symptoms of headache, neck pain, shoulder pain, dizziness, and tinnitus. Cranio. 1996;14:46–54. doi: 10.1080/08869634.1996.11745949. [DOI] [PubMed] [Google Scholar]
- 32.Guzay C.M. Introduction to the quadrant theorem. Basal Facts. 1976;1:153–160. [PubMed] [Google Scholar]
- 33.Guzay C.M. Quadrant theorem—part two. Basal Facts. 1977;2:19–33. [PubMed] [Google Scholar]
- 34.Guzay C.M. Quadrant theorem. Part III. Basal Facts. 1977-1978;2:171–183. [PubMed] [Google Scholar]
- 35.Alcantara J., Plaugher G., Klemp D.D., Salem C. Chiropractic care of a patient with temporomandibular disorder and atlas subluxation. J Manipulative Physiol Ther. 2002;25:63–70. doi: 10.1067/mmt.2002.120415. [DOI] [PubMed] [Google Scholar]
- 36.Blum C.L. Spinal/cranial manipulative therapy and tinnitus: a case history. Chiropr Tech. 1998;10:163–168. [Google Scholar]