

Abstract
Rationale
Attentional biases and executive control deficits may play a role in smoking cessation failure.
Objectives
The object of this study was to determine whether smokers' pre-quit reaction times on a computerized modified Simon task (which assesses attentional biases and executive control deficits) predict abstinence following a quit attempt.
Methods
Participants (N=365) in a larger smoking cessation clinical trial completed the modified Simon task twice (while 10-h nicotine-deprived vs. not deprived). In the task, two photographs (i.e., two digital slides) were displayed—one always neutral, the other positive, negative, smoking-relevant, or neutral. A probe (≪< or ≫>) then appeared to the left or right of center, and participants indicated the arrow's direction (left or right) which was either congruent or incongruent with the arrow's location on the screen. The incongruency effect, a measure of executive control, was calculated by subtracting the reaction time to congruent probes from the reaction time to incongruent probes.
Results
Greater impairment in executive control (i.e., greater probe incongruency effects) after viewing positive and smoking slides relative to negative slides predicted an inability to establish initial cessation and to maintain abstinence up to 8 weeks post-quit.
Conclusions
These effects may be because smokers who avoid/escape from processing negative affect are more likely to fail in a cessation attempt. Differences in relatively automatic responses to affective cues distinguish smokers who are successful and unsuccessful in their smoking cessation attempts, but effects were modest in size.
Keywords: Smoking cessation, Attention, Information processing, Nicotine withdrawal
Smoking cessation failure is common; even with state of the art treatment, only a minority of smokers will be abstinent 6 months after their quit date (Fiore et al. 2008; Piper et al. 2009). The prediction of smoking cessation failure may shed light on motivational factors involved in nicotine dependence and relapse. Self-report measures have often been used to understand the processes that lead to relapse (e.g., Bolt et al. 2009), but these have limitations, e.g., an inability to tap implicit or unconscious processing (Tiffany 1990), a tendency to reflect broad attitudes, and psychometric shortcomings. Therefore, measures such as reaction times on cognitive tasks have been used to gain insight into relapse processes (e.g., Waters et al. 2003b).
Identifying cognitive risk factors for relapse back to smoking is important for multiple reasons. Such risk factors may guide the design of new treatments that target the information processing mechanisms of addiction motivation, inform treatment selection and treatment adjustments for individual smokers, and provide endophenotypes or subphenotypes for research on the molecular genetics of nicotine dependence.
Studies of smokers' performance on information processing tasks have generally used either the modified Stroop task or the visual probe task. In the modified Stroop task, participants are asked to report the ink color of a smoking-related, neutral, or other type of word as quickly as possible. Slower reaction times on trials with smoking-related words versus other types of words (e.g., neutral words) are thought to reflect an attentional bias toward smoking words. In the visual probe task, two images are presented parallel to each other on a computer screen. One is the target image (i.e., an affectively valenced or smoking image) and one is neutral. The images disappear, a probe appears in the location of either the target or neutral image, and participants identify the type of probe (e.g., “..” versus “:”) as quickly as possible. Some studies exhibit a response pattern that has been attributed to “sticky attention” in which participants respond especially slowly to trials where the target slide location does not match the subsequent probe location. Sticky attention has been attributed to a difficulty on mismatched trials in disengaging and/or shifting attention away from the target slide location and toward the mismatched probe location. This difficulty is thought to be associated with affective or motivational state.
Studies using information processing tasks have generally found that smokers show an attention bias for smoking-relevant stimuli relative to neutral stimuli (Bradley et al. 2004; Cox et al. 2006; Waters et al. 2003a). A recent study (McCarthy et al. 2009), however, found that smokers did not show a bias for smoking-related words relative to pleasant (sex- and pleasure-related) words on the modified Stroop task. This study, instead, found a functional equivalence between classes of appetitive cues (i.e., smoking and pleasant words); both smokers and non-smokers showed an attentional bias for appetitive (smoking and pleasant) words versus unpleasant words. This suggests that contrasting smoking with other appetitive stimuli may remove important variance from smoking cue effects that may possess motivational significance.
Although multiple studies have assessed attentional biases in smokers, few have examined whether these biases predict real-world behavioral outcomes. Waters et al. (2003a) did examine whether attention bias (i.e., sticky attention) for smoking versus neutral stimuli on a visual probe task 2 weeks before the quit day predicted number of days to first lapse through 3 months following the quit day and found that it did not. Using the same sample but a different task (a modified Stroop task given on the quit day while participants were abstinent), however, Waters et al. (2003b) found that smokers' attentional bias for smoking versus neutral words marginally predicted both abstinence at 1 week and days to first lapse. These limited, mixed findings point to the need for additional research on the relation between information processing biases and smoking cessation outcome.
The present study tested whether smokers' pre-quit reaction times on a computerized task predicted their cessation success. The task was a modified version of the classic Simon task (Lu and Proctor 1995; Simon and Rudell 1967)—an information processing task designed to provide an index of executive control function during exposure to affective (positive and negative valence), neutral, and smoking images (see Fig. 1a for a schematic of the trial structure).
Fig. 1.
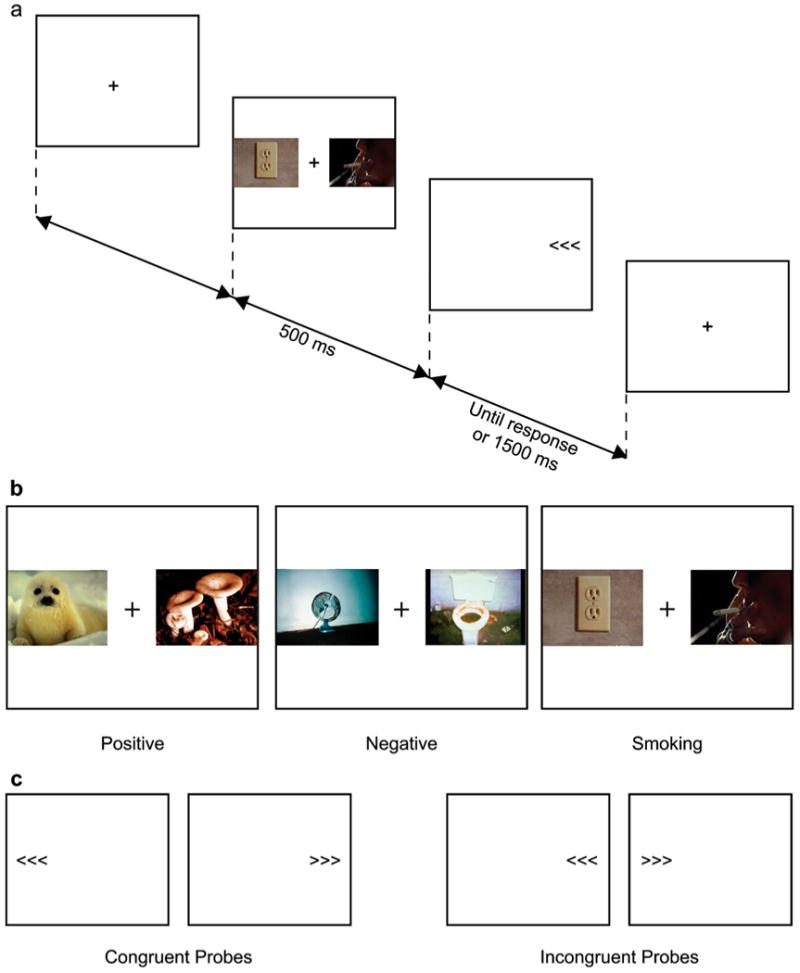
A schematic of the modified Simon task. a Presents the slide projection procedure starting with a fixation cross. In this example, the probe appears in the same location as the primary smoking slide (i.e., there is slide–probe match), and the probe is incongruent (a left-pointing arrow is to the right of fixation). b Presents three sample computer screens showing that the primary slide (either positive, negative, or smoking) was always accompanied by a neutral slide. c Presents the four possible probe computer screens. In the two screens on the left, the probes are congruent—the arrow's direction (left or right pointing) is congruent with the arrow's location on the screen (left of fixation or right of fixation). In the two screens on the right, the probes are incongruent—the arrow's direction is incongruent with the arrow's location on the screen
Participants completed 84 trials of the task twice: once while deprived of nicotine for ≥10 h and once while not deprived. In each trial—following a fixation cross in the center of the computer screen—two photographic images appeared for 500 ms oriented horizontally to the left and right of the fixation cross (see Fig. 1b). One slide was always neutral. The other was positive, negative, smoking-relevant, or neutral. Following the presentation of a pair of slides, a probe consisting of three arrows (≪< or ≫>) was displayed to the left or right of fixation until the participant responded or for up to 1,500 ms. The participants' task was to press one of two buttons (held in separate hands with their thumbs near the thumb-operated buttons) as quickly as possible to indicate the direction the arrows were pointing. The arrow's direction (left vs. right pointing) was either congruent or incongruent with the arrow's location on the screen (left of fixation vs. right of fixation; see Fig. 1c). There were an equal number of probe congruent (42) and incongruent (42) trials. As in the classic Simon task, the probe's location on the screen was irrelevant to determining the correct response. The Simon effect refers to the well-substantiated finding (Lu and Proctor 1995) that participants respond more quickly when the probe location is congruent with the correct response versus incongruent (e.g., a left-pointing arrow presented to the right of fixation). The effect of probe congruency on participants' reaction times can be seen as a measure of participants' executive control (i.e., their ability to inhibit a dominant response and give a non-dominant response quickly in the presence of response conflict).
Probe location relative to the primary (non-neutral) slide was balanced (i.e., half the probes were presented in the same location as the primary slide). This design permitted us to investigate the effect of slide–probe match (i.e., the effect of sticky attention—the tendency to respond more quickly when the probe is in the same vs. in the opposite location as the primary slide).1 We selected the modified Simon task, in part, because it permits tests of multiple factors and their interactions within the same paradigm, i.e., whether there were main effects or interaction effects on participants' reaction times for Probe Congruency (congruent vs. incongruent probes—a measure of executive control), Slide–Probe Match (whether the probe location matched vs. mismatched the primary slide location—a measure of sticky attention), Slide Type (negative, positive, or smoking slides), and Nicotine Deprivation (deprived vs. nondeprived), and whether any of these effects predicted cessation outcome. We examined the effects of Slide Type with two planned orthogonal Helmert contrasts that mapped onto effects of interest. As McCarthy et al. (2009) did, the Slide Type factor (negative vs. positive vs. smoking) was decomposed into two orthogonal contrasts: (a) negative vs. positive+smoking slides (i.e., negative vs. appetitive) and (b) positive vs. smoking slides. The sparse literature reviewed earlier on cognitive performance in relation to smoking cessation outcome and a lack of strong guiding theory suggested three general hypotheses regarding the relations of reaction time to cessation outcome.
Hypothesis 1 (sticky attention)
Research on sticky attention in smokers is limited. Evidence of sticky attention for smoking versus control slides has been reported in visual probe tasks (Bradley et al. 2004; Field et al. 2004), but this bias was not related to cessation outcome in the single study analyzing this effect (Waters et al. 2003a). In the sticky attention hypothesis, we predicted that smokers would have worse cessation outcomes if they showed slower responses to slide–probe mismatch than match trials in the presence of appetitive (positive and smoking) target slides versus negative target slides. In other words, we hypothesized that the interaction of Slide–Probe Match× Slide Type (negative versus positive+smoking slides) would predict cessation outcome. We based this prediction in part on the McCarthy et al. (2009) findings suggesting that smokers may have a bias for appetitive cues rather than a unique bias for smoking cues. Because sticky attention was not related to withdrawal in the Field et al. (2004) study, we did not predict that participants' sticky attention would be affected by withdrawal status.
Hypothesis 2 (executive control)
We hypothesized that smokers' general impairment in executive control on the task (i.e., their degree of probe congruency effects regardless of slide type) would predict poor cessation outcomes. That is, relapse should be related to a relative inability to engage in non-dominant response options such as choosing not to smoke in the face of an urge or smoking cue (Curtin et al. 2006). This hypothesis was based on findings that difficulties with executive control are associated prospectively with a range of negative outcomes, including externalizing behaviors (Olson et al. 1999), difficulties showing self-control in frustrating situations in adolescents (Shoda et al. 1990), and drug use (Ayduk et al. 2000).
Hypothesis 3 (contextually impaired executive control)
Our third hypothesis predicted that the degree to which nicotine-deprived (vs. nondeprived) participants showed greater impairment in executive control when resolving incongruent versus congruent probes following appetitive (positive and smoking) versus negative cues would predict worse cessation outcomes. In other words, we predicted that the interaction of Smoking Deprivation×Probe Congruency× Slide Type (negative versus positive+smoking slides) would predict cessation outcome. This interaction hypothesis comprised a test of whether probe congruency and slide type would exert different effects as a function of deprivation, i.e., whether executive control impairment is most apparent when smokers are nicotine-deprived versus not deprived (see Dawkins et al. 2007) and processing demands are increased by provocative cues. We note that the predicted interaction of Smoking Deprivation×Probe Congruency×Slide Type (negative versus positive+ smoking slides) contrasts with hypothesis 2 and with other appraisals of executive control (e.g., Thush et al. 2008) that do not examine contextual influences.
In theory, appetitive cues would particularly attract attentional processing and disrupt executive control in smokers prone to relapse. In other words, smokers drawn to these appetitive cues would take longer following such cues to exert executive control and enact a non-dominant response. This possible mechanism may be influenced by the high attentional salience of drug cues and other signals of reward as they are inflated by dopaminergic mechanisms (Berridge 2007). In addition, appetitive cues such as drug cues could elicit craving and thereby occupy executive control resources and slow reaction times that depend upon having executive control resources available (Franken 2003). These effects on attentional processing might be further inflated by nicotine deprivation which appears to increase the allocation of executive control resources to drug cues (Gloria et al. 2009). Presumably, disruption of executive control by reward signals (such as drug cues) would reduce a person's ability to cope with temptation in an adaptive manner and not smoke when trying to abstain (Curtin et al. 2006; Franken 2003).
Negative affect might also account for a discrepancy between reaction times following appetitive versus aversive cues (cues that elicit negative affect). There is a great deal of evidence that negative affect is associated with relapse vulnerability (e.g., Baker et al. 2004; Kenford et al. 2002; Piper et al. 2008). Smokers who are high in negative affect and/or tend to engage in experiential avoidance (i.e., trying to avoid aversive feelings) may be at greater risk of relapse back to smoking, and they may also be primed to process negative cues quickly. That is, relative to other smokers, they may process negative cues more automatically, or they may disengage their attention from negative cues more quickly. This idea is based, in part, on strong evidence that people with depression display a processing bias for mood-congruent stimuli (for a review see Elliott et al. 2002). For example, unmedicated people with depression processed sad words more quickly than happy words on the Affective Go/No-Go Task, while healthy controls processed happy words more quickly than sad ones (Erickson et al. 2005). Of course, there is also seemingly contradictory evidence from the emotional Stroop task that people with depression process sad words more slowly than neutral words (Williams et al. 1996). These different findings may be related to the specific task and the time course of the processing involved. In the modified Simon task, we believed that smokers with future poor cessation outcomes would process the negative, aversive photographs faster than the appetitive photographs because such smokers may be more likely to engage in experiential avoidance and the aversive aspects of the negative stimuli may lead to disengagement. Thus, as part of our third hypothesis, we predicted that smokers with poor cessation outcomes would show less disruption in executive control following exposure to negative affect cues than following exposure to appetitive cues. Moreover, this model suggests that withdrawal should further decrease disruption of executive processing by negative cues because withdrawal increases negative affect and therefore should further speed processing of negative cues (cf. Leventhal et al. 2008).
We have described two mechanisms that could render appetitive cues more effective than negative cues in disrupting executive control in smokers with subsequent poor cessation outcomes: smokers with poor versus good outcomes may (a) respond more slowly after appetitive/smoking cues and thus produce slower reaction times or (b) tend to be high in negative affect or experiential avoidance and therefore process negative cues faster (e.g., negative cues may be more highly primed in such smokers). Either or both of these two mechanisms may be involved, and both can be theoretically linked to relapse vulnerability.
Method
Participants
Participants were 365 smokers (57% female, 90% White; see Table 1) from Southeastern Wisconsin enrolled in a randomized placebo-controlled efficacy trial comparing five smoking cessation pharmacotherapy conditions (see Piper et al. 2009). All participants who entered the trial after a certain date completed the current study's computerized information processing task. Inclusion criteria included heavy smoking (>10 cigarettes/day) and being motivated to quit smoking. Exclusion criteria included medical contraindications to study medications, heavy alcohol consumption (≥6 drinks 6–7 days a week), or self-reported history of seizure, schizophrenia, psychosis, an eating disorder, or bipolar disorder. All participants gave written informed consent, and the University of Wisconsin Health Sciences Institutional Review Board approved the study.
Table 1. Baseline sample characteristics (N=365).
| % Female | 57.3% |
| Race | |
| % White | 90.4% |
| % African American | 6.6% |
| % Other race | 3% |
| % With a high school education or greater | 97% |
| % Married or living with a partner | 60.2% |
| Mean age (SD) | 43.81 (11.51) |
| Mean number of cigarettes per day (SD) | 21.32 (8.64) |
| Mean number of years smoked (SD) | 25.47 (11.72) |
| Mean score on the Fagerström Test for Nicotine Dependence (SD) | 5.24 (2.15) |
| Mean baseline CO in parts per million (SD) | 24.67 (11.25) |
Participants completed the information processing task in two different counterbalanced sessions: once while deprived of nicotine overnight and once while not deprived. Both sessions occurred prior to the participants' quit attempt and use of any cessation medication. Participants were included in the current study if they: (a) completed the task during two different sessions, (b) reported not smoking for at least 10 h for the “deprived” session and smoking in the last 2 h before the “nondeprived” session, (c) had sufficiently low error and no response rates on the task during both sessions (the maximum allowable number of errors or no responses per a session was 17, i.e., 20% of trials), and (d) provided cessation outcome data.
Measures
Smoking status
Seven-day point-prevalence abstinence was biochemically confirmed by an expired carbon monoxide (CO) rating of less than 10 parts per million. The study included four smoking outcome indices: (a) initial cessation (remaining abstinent for at least 1 day in the first week post-quit), (b) biochemically confirmed 7-day point-prevalence abstinence 1 week post-quit, (c) number of days smoked in the first 7 days post-quit, and (d) biochemically confirmed 7-day point-prevalence abstinence at 8 weeks post-quit (i.e., the end of treatment except for those receiving the nicotine lozenge). (Please note that the terms “pre-quit” and “post-quit” mean, respectively, the time period before and after a participant's target quit day.) The use of multiple diverse outcome indices permitted tests of the robustness of the task performance–outcome relations. We focused on relatively short-term outcomes because we believed distal outcomes would be less sensitive to the information processing characteristics reflected by task performance and would be more sensitive to fortuitous events such as exposure to stressors and temptation events.
Demographics and smoking history
Participants reported their age, race, other demographic characteristics, and their smoking behavior (e.g., cigarettes smoked per day).
Fagerström Test of Nicotine Dependence (FTND)
The FTND (Heatherton et al. 1991) comprises six items. Scores range from 0 to 10; higher numbers indicate greater dependence.
Wisconsin Smoking Withdrawal Scale (WSWS)
The WSWS (Welsch et al. 1999) is a 28-item measure of nicotine withdrawal. Immediately prior to the information processing task, participants completed a ten-item WSWS that assessed the following scales: anger, anxiety, sadness, hunger, and concentration. This abbreviated form consisted of the two strongest loading questions for each scale in the scale derivation factor analysis (Welsch et al. 1999).
Modified Simon task
In each trial of the task, two digital slides (each sized to 461×346 pixels) appeared oriented horizontally to the left and right of the fixation cross (see Fig. 1b). One of the slides was always neutral (e.g., a person with a neutral facial expression, a clock). The other was either positive (e.g., people white water rafting, a bare-chested father embracing his naked baby, an attractive elderly couple smiling at each other), negative (e.g., a child crying, a woman with bruises on her face, a dead animal), smoking-relevant (e.g., a person lighting up a cigarette, a close-up of a person's mouth exhaling smoke while holding a cigarette, three friends having cocktails and smoking), or neutral. The positive, negative, and neutral slides were from the International Affective Picture System (Lang et al. 1999). The positive slides did not include the sexual images. The smoking-relevant slides were generated in our laboratory, rated by smokers, and found to create the expected effects (Shi 1998). The mean arousal ratings—on a scale from 1 (calm) to 10 (excited)—were 5.4, 5.4, and 4.7 for the positive, negative, and smoking slides, respectively.2 Thus, the positive slides were approximately matched on arousal with the negative and smoking slides. The mean valence ratings—on a scale from 1 (sad) to 10 (happy)—were 7.9, 2.1, and 4.8 for the positive, negative, and smoking slides, respectively. Thus, the positive and negative slides were matched on valence intensity.
Each slide was presented only once. There were four blocks of trials: (a) 24 trials pairing a positive and neutral slide, (b) 24 trials pairing a negative and neutral slide, (c) 24 trials pairing a smoking and neutral slide, and (d) 12 trials pairing two different neutral slides. The slides were presented in blocks by slide type (rather than interleaved) because we believed the effect would be stronger if blocked, and we were concerned about carryover if different slide types were interleaved. Within each of the four blocks, individual slides were randomly presented. The order of the four blocks and the location (left vs. right of fixation) for the positive, negative, and smoking slides were crossed and counterbalanced across participants. Participants were randomized to one of four different task orders, and participants completed the same task order in both sessions
Procedure
Potential participants who passed the phone screen were invited to a group information session where they provided written, informed consent. Next, participants completed an individual orientation session where they underwent screening for exclusion criteria and completed demographic, smoking history, and tobacco dependence questionnaires. Qualified participants then completed three baseline visits. The baseline visits did not have a set time frame in relation to the quit day, except the last visit, where medication was dispensed, which took place between 8 and 15 days pre-quit. All participants completed the information processing task during baseline visit two (between 8 am and noon) after being deprived overnight of nicotine and caffeine, and they also completed the task while not deprived at either baseline visit one or three (counterbalanced). The number of days between the two times participants completed the task ranged from 0 to 47 with a mean of 10.11 days (SD=7.90).
At the end of baseline visit three, qualified participants were randomized in a double-blind fashion to one of six treatment conditions: (1) bupropion SR (150 mg, twice daily for 9 weeks total—1 week prior to the quit day plus 8 weeks starting on the quit day); (2) nicotine lozenge (2 or 4 mg based on dependence level for 12 weeks starting on the quit day); (3) nicotine patch (21, 14, and 7 mg; titrated down over the 8 weeks following the quit day); (4) nicotine patch+nicotine lozenge; (5) bupropion SR+nicotine lozenge; or (6) one of five placebo conditions matched to the five active conditions. All participants received six brief (10–20 min) individual counseling sessions (see Piper et al. 2009 for details).
Participants completed the information processing task in a darkened room looking at the 14-in screen (refresh rate 60 Hz) with 1,024 by 768 resolution of either an IBM G40 ThinkPad laptop (IBM Corporation, Armonk, NY) or a Dell Latitude D600 laptop (Dell Inc., Round Rock, TX). The task was delivered using DMDX software (Forster and Forster 2003). Before beginning the task, participants typed into the computer when they last smoked and their responses to the WSWS questionnaire. Participants then read the task instructions on the computer screen, including: “Please try to perform this task as quickly and accurately as possible.” Participants completed eight practice trials and then received feedback on the computer screen tallying their errors. While participants completed the task, the research assistant stood behind them and observed unobtrusively to ensure they complied with instructions. The computer gave participants three 30-s breaks during the task. Total task time was approximately 20 min.
Results
Data preparation
Reaction times shorter than 200 ms were considered invalid and discarded, as were incorrect responses. To protect against violations of the assumption of sphericity, reported p-values are based on Huynh–Feldt estimates of sphericity to correct the degrees of freedom.
Preliminary analyses
Manipulation check of nicotine deprivation versus no deprivation conditions
Participants completed the WSWS measure of withdrawal symptoms immediately prior to the task. Participants' scores on both the individual items of the scale and on the five subscales (anger, anxiety, sadness, hunger, and difficulty with concentration) were higher when nicotine-deprived vs. nondeprived (all p's≤0.009).
Control variables
We assessed whether any socio-demographic variables (age, sex, race, marital status, education, or income) were correlated with participants' overall reaction times on the task. With a Bonferroni-corrected p-value of 0.008 to control for the six correlations tested (0.05/6=0.008), only age was correlated with performance. As prior research has found (e.g., Fozard et al. 1994), older age was associated with slower overall reaction time, r(363)=0.33, p<0.001. We therefore included age as a control variable in subsequent analyses.
Preliminary analyses of the modified Simon task effects
Main effects of slide type, probe congruency, slide–probe match, and nicotine deprivation on participants' reaction times were analyzed in a General Linear Model (GLM) with four repeated-measures factors: (a) Slide Type (negative, positive, or smoking slides); (b) Probe Congruency (congruent vs. incongruent); (c) Slide–Probe Match (match vs. mismatch); and (d) Nicotine Deprivation (deprived vs. nondeprived). Age (converted to a z-score) was included as a control variable. Partial η2 was used as the measure of effect size with 0.02, 0.15, and 0.35 considered small, medium, and large effects, respectively (Cohen 1992). We examined the effects of Slide Type on reaction time with two planned orthogonal Helmert contrasts that mapped onto effects of interest: (a) negative vs. positive+smoking slides (i.e., negative vs. appetitive slides) and (b) positive vs. smoking slides. These contrasts revealed that participants' mean response to probes following negative slides (M= 583 ms, SE=5.3) was slower than the average of their responses to probes following positive (M=562 ms, SE= 5.1) and smoking slides (M=570 ms, SE=5.2), F(1, 363)= 57.09, p<0.001, ηp2=.14. Participants' response to probes following smoking slides was also slower than their response following positive slides, F(1, 363)=14.30, p< 0.001, ηp2=.04.
There was a main effect of Probe Congruency, F(1.00, 363.00)=953.51, p<0.001, ηp2=0.72, as participants were slower on probe incongruent (M=599.7 ms, SE=5.2) than congruent trials (M=543 ms, SE=4.96). There was, however, no main effect of Slide–Probe Match (p=0.53); overall participants responded similarly when the probe appeared on the opposite side of the screen from where the primary slide had been (slide–probe mismatch; M=572 ms, SE=5.1) as when the probe appeared on the same side of the screen as the primary slide (slide–probe match; M= 571 ms, SE=5.02).3 Finally, there was a main effect of Nicotine Deprivation, F(1.00, 363.00)=47.60, p<0.001, ηp2=0.12; participants responded more slowly when nicotine-deprived (M=587 ms, SE=5.5) than when not deprived (M=556 ms, SE=5.5). There were no significant, substantive interaction effects, and we did not examine interaction effects with age.
Main analyses of the modified Simon task effects
We assessed whether reaction times on the task predicted four cessation outcomes: (a) initial cessation (which 87.1% attained), (b) point-prevalence abstinence 1 week post-quit (41.1% abstinent), (c) number of days smoked in the first 7 days post-quit (median=1 day), and (d) point-prevalence abstinence at 8 weeks post-quit (51.5% abstinent).4 Recent research has shown that such diverse outcome indices are not equivalent and may share different relations with treatment condition and other sorts of variables (Shiffman et al. 2006). Correlations among these cessation outcome indices ranged from moderate in size (i.e., r=.31: the correlation between initial cessation and abstinence at 8 weeks post-quit) to high (i.e., r=−0.80: the correlation between initial cessation and the number of days smoked in the first 7 days post-quit).
We analyzed participants' reaction time in a GLM with four repeated-measures factors: (a) Slide Type (negative, positive, or smoking slides); (b) Probe Congruency (congruent vs. incongruent); (c) Slide–Probe Match (match vs. mismatch); and (d) Nicotine Deprivation (deprived vs. nondeprived), with age, treatment type (active versus placebo), and cessation outcome as control variables. We included cessation outcome as a control variable to assess the relationship between task performance and this outcome. Age was converted to a z-score, and treatment type and cessation outcome were mean-centered to simplify interpretation of interactions (Cohen et al. 2003).
We conducted the analysis four separate times—once for each cessation outcome. Within the GLM, the only effects interpreted involved substantive outcomes. We therefore focused on main effects (described under Preliminary Analyses—results did not change when treatment and cessation outcome were included as control variables) and interaction effects and did not examine interactions with age and treatment. For interaction effects involving Slide Type, we conducted two planned orthogonal Helmert contrasts that mapped onto effects of interest: (a) negative versus positive+smoking slides and (b) positive versus smoking slides.
Hypothesis testing: hypothesis 1
The first Helmert contrast found no significant interaction of Slide Type (negative versus positive+smoking slides)×Slide–Probe Match×Cessation Outcome Measure for any of the four cessation outcomes. Thus, contrary to our prediction, smokers were not more likely to have poor cessation outcomes if they showed sticky attention (i.e., showed slower responses to slide–probe mismatch than match trials) in response to appetitive versus negative target slides.
Hypothesis testing: hypothesis 2
The interaction of Probe Congruency×Cessation Outcome Measure was not significant for any of the four cessation outcomes. Thus, contrary to our prediction, smokers' general degree of executive control impairment on the task (i.e., the degree of probe congruency effects), as indexed across all three slide types, did not predict poor cessation outcomes.
Hypothesis testing: hypothesis 3
The first Helmert contrast found—across all four cessation outcomes—a significant interaction of Slide Type (negative versus positive+smoking slides)×Probe Congruency×Cessation Outcome Measure (see Table 2).5 This interaction provided partial support for our third hypothesis. Thus, across all four cessation outcomes, poorer cessation outcomes were related to greater impairment in executive control (i.e., greater slowing/larger incongruency effects) after viewing appetitive (positive and smoking) slides than after viewing negative slides (see Fig. 2). In fact, participants with poor cessation outcomes did not show particularly strong incongruency effects after viewing negative slides, but they tended to show larger incongruency effects following positive and smoking slides, i.e., they responded faster to congruent than to incongruent probes following positive and smoking slides. In contrast, participants who achieved abstinence tended to show smaller incongruency effects after viewing positive and smoking slides and somewhat larger incongruency effects after viewing negative slides.
Table 2. Helmert contrasts showing—across all four cessation outcome measures—a significant interaction of Slide Type (negative versus positive+ smoking slides)×Probe Congruency×Cessation Outcome Measure.
| Cessation outcome measure | Helmert contrast |
|---|---|
| Initial cessation (not smoking at least 1 day in the first week post-quit) | F(1, 361)=9.41, p=.002, ηp2=0.03 |
| Abstinence at 1 week post-quit | F(1, 361)=7.92, p=.005, ηp2=0.02 |
| Days smoked in the first week post-quit | F(1, 361)=6.68, p=.01, ηp2=0.02 |
| Abstinence at 8 weeks post-quit | F(1, 361)=4.65, p=.03, ηp2=0.01 |
Fig. 2.
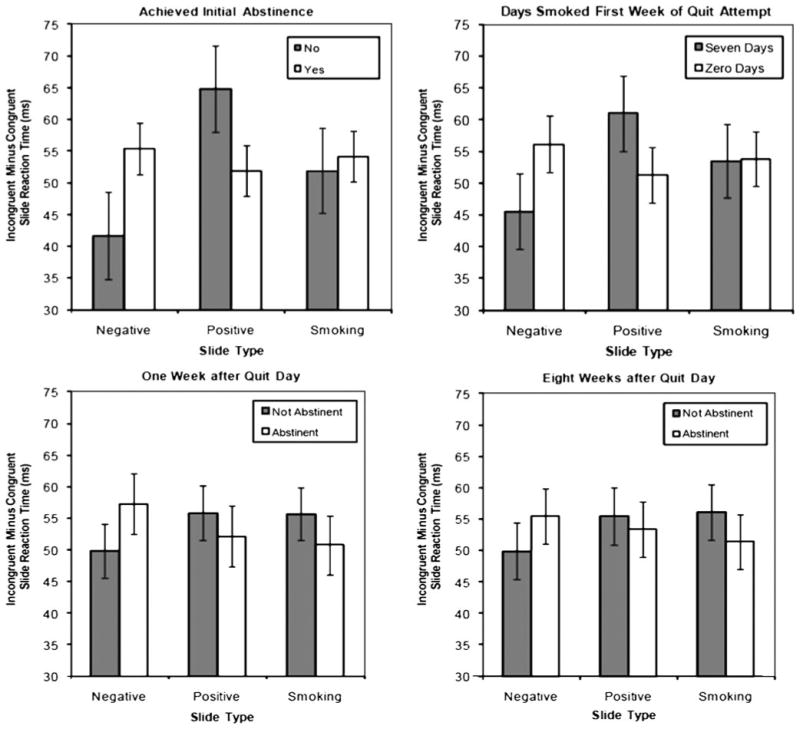
Incongruent probe reaction times minus congruent probe reaction times across three slide types (negative, positive, and smoking) for participants who had good or poor abstinence outcomes at four different time points. Figures are point estimates from the model (±SE). For the outcome days smoked in the first week, we chose to graph only endpoints (i.e., smoking all 7 days or not smoking at all in the first week) because the endpoints showed the full range of the effect and because there were more participants at the endpoints making estimates more precise at those time points
For the cessation outcome of abstinence at 1 week, however, the interaction just described of Slide Type (negative versus positive+smoking slides)×Probe Congruency×Cessation Outcome at 1 week was subsumed by a significant Helmert contrast for Slide Type (negative versus positive+smoking slides)×Probe Congruency×Smoking Deprivation×Cessation Outcome at 1 week, F(1, 361)= 4.25, p=0.04, ηp2=0.01. This interaction involving smoking deprivation was what we predicted in our third hypothesis. As Fig. 3 shows, participants not abstinent at 1 week tended to show relatively weak incongruency effects after viewing negative slides while nicotine-deprived but not after recent smoking, i.e., participants not abstinent at 1 week tended to respond while in withdrawal almost as quickly to incongruent probes following negative slides as they did to congruent probes following negative slides.
Fig. 3.
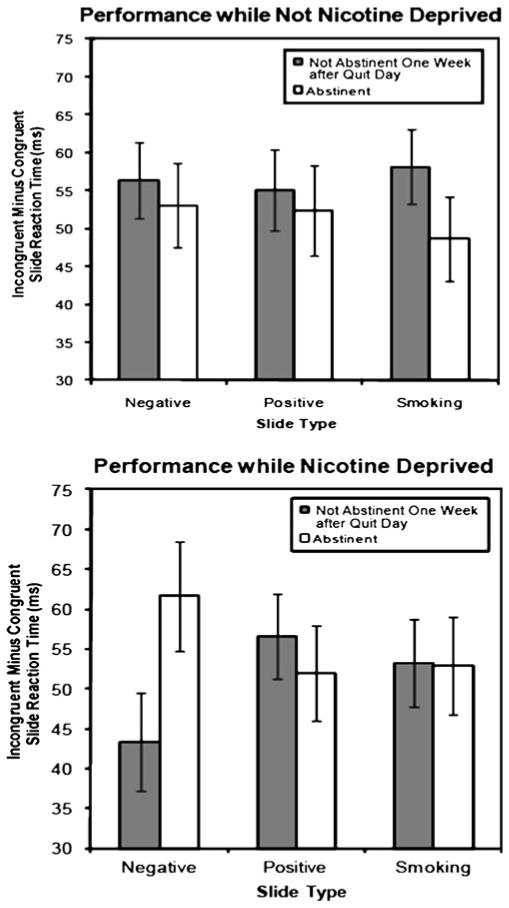
Incongruent probe reaction times minus congruent probe reaction times across three slide types (negative, positive, and smoking) under pre-quit conditions of nicotine deprivation and no deprivation for participants who were or were not abstinent at 1 week post-quit. Figures are point estimates from the model (±SE)
Additional findings
For the cessation outcome of initial cessation, the second orthogonal Helmert contrast was significant in addition to the first. This second contrast found an interaction of Slide Type (positive vs. smoking slides)×Probe Congruency (congruent vs. incongruent)× Initial Cessation, F(1, 361)=4.18, p=0.04, ηp2=0.01. Examination of Fig. 2 suggests that participants who did not quit smoking for at least 1 day took a particularly long time to respond to incongruent probes following positive slides relative to congruent probes following positive slides, whereas they responded to incongruent probes following smoking slides only somewhat more slowly than they responded to congruent probes following smoking slides. On the other hand, participants who quit smoking for at least 1 day had roughly comparable incongruency effects (incongruent minus congruent probe reaction times) for both positive and smoking slides.
Discussion
In our first hypothesis, we predicted smokers would be more likely to have poor cessation outcomes if they showed sticky attention (i.e., slower responses to slide–probe mismatch than match trials) in response to appetitive (smoking and positive) versus negative target slides. However, we found no evidence to support this hypothesis, nor did we find evidence of sticky attention altogether (see Preliminary Analyses). It is possible that elements of the task design led to this null finding (e.g., perhaps participants did not need to shift their eye gaze from the target slide location to view a probe on the opposite side of the screen or perhaps sticky attention is more evident in the visual probe task than in the modified Simon task). Nevertheless, our finding is consistent with the Waters et al. (2003a) finding that a measure intended to index sticky attention did not predict outcome in treatment-seeking smokers.
In our second hypothesis, we predicted that the degree of executive control impairment participants showed on the task (i.e., the degree of probe congruency effects) across all three slide types would predict poor cessation outcomes, but we found that it did not. Although our first two hypotheses were not supported, our final hypothesis was partially supported. We found that smokers' pre-quit performance on the modified Simon task in response to specific cues predicted their smoking cessation outcomes (across four different outcome indices). As predicted in the third hypothesis, poor cessation outcomes were related to greater executive control impairment (i.e., greater probe incongruency effects) following appetitive (smoking and positively valenced) cues than following negatively valenced cues. Our hypothesis that this effect would be especially apparent under conditions of nicotine withdrawal was supported only for abstinence at 1 week. For the other three cessation outcomes, the prediction was supported except it did not depend on whether participants were nicotine-deprived. That is, across both deprived and nondeprived trials, participants who had poor cessation outcomes generally had larger incongruency effects following appetitive (positive and smoking) stimuli and smaller incongruency effects following negative stimuli than did those who maintained abstinence.
This finding suggests that participants who have poor cessation outcomes may find appetitive cues in their environment (both drug and nondrug) particularly distracting and difficult to shrug off; these cues may occupy their working memory resources and induce cravings (Franken 2003), resulting in less executive control resources available for other self-regulatory tasks. Indeed, one study (Littel and Franken 2007) measured event-related potentials and found that current smokers showed a greater processing bias (i.e., enhanced processing) for smoking-relevant photographs than both never-smokers and former smokers who had been abstinent for at least 6 months. Another study (Munafo et al. 2003) similarly found smokers were slower to name smoking-relevant words than neutral words on the Stroop task, but a group of never-smokers and former smokers did not show this bias. These findings are compatible with our finding that smokers with poor versus good cessation outcomes showed a greater incongruency effect (i.e., a greater processing bias) following appetitive (smoking and positive) slides and a smaller incongruency effect following negative slides when they completed the task pre-quit.
The relatively large incongruency effect seen with appetitive slides in participants with unsuccessful outcomes may seem anomalous. One possible account is that this interference reflects the greater attentional salience of smoking slides per se due to their high level of incentive salience (Berridge 2007) for participants with poor cessation outcomes. An incentive salience model though would seem to predict that incentive salience would be greater for smoking cues than for other sorts of appetitive cues. However, participants with unsuccessful versus successful cessation outcomes tended to be maximally dissimilar in response to the negative versus positive slides; their responses to the smoking slides were often somewhat intermediate. Thus, the results may be more consistent with an affective priming or novelty account than with an incentive salience account.
The affective priming account holds that participants' engagement with the pictorial stimuli reflects a match/ mismatch with their trait-like or ongoing affective tone (the greater the mismatch, the greater the processing demand). According to this account, high ongoing negative affect (or low positive affect) would have produced poor cessation outcomes. This relation is well-documented (e.g., Baker et al. 2004; Kenford et al. 2002; Piper et al. 2008), although the causal link between high negative affect or low positive affect and poor cessation outcomes is unclear. In this affective priming account, high negative affect would also render the negative slides more familiar (and prime their content), which would reduce the call for cognitive processing. Positive slides would constitute a greater mismatch for people routinely processing distress-related information and therefore would engender a greater allocation of executive control resources. Smoking slides often produced an intermediate interference effect for participants with unsuccessful cessation outcomes. This suggests that such slides were intermediate to positive and negative slides in affective tone (e.g., Wiers et al. 2006, p. 343). The results of the current study do not allow us to distinguish the time course of such familiarity or priming effects (i.e., whether such effects are more state-like or trait-like).
If the effects observed with the appetitive slides (and particularly with the positive slides) are really due to familiarity with, or priming of, affect, then the same participants who showed relatively larger incongruency effects following positive stimuli (participants who had poor cessation outcomes), should have shown relatively smaller incongruency effects following negative stimuli. This pattern is indeed what was found and is compatible with the notion that participants with poor cessation outcomes often have high levels of negative affect/low levels of positive affect and thus, may be primed to process negative stimuli quickly or to engage in experiential avoidance and avoid processing negative stimuli. Experiential avoidance has been associated with emotional distress and psychopathology (Kashdan et al. 2006; Brown et al. 2005). The pattern of results is also consistent with Erickson et al.'s (2005) finding with the Affective Go/No-Go Task that healthy controls process happy stimuli faster than sad stimuli while depressed people process sad stimuli faster than happy stimuli.
While responses to the positive versus smoking slides can be distinguished in some regards, it is important to bear in mind that the strongest findings with regards to the prediction of cessation outcomes involved the first Helmert contrast in which responses to the smoking plus the positive slides were contrasted with responses to the negative slides. (For only one cessation outcome—initial cessation—was the second orthogonal Helmert contrast of positive versus smoking slides significant.) While this finding might merely reflect factors such as enhanced reliability, the finding does suggest that response to the smoking slides covaried meaningfully with response to the positive slides and possessed predictive validity with regards to cessation outcomes. This may speak less to the similarity of the positive and smoking slides though and more to the uniqueness of the negative slides (i.e., essentially, there were really two types of slides, those that were negative, and those that were not).
The present results underscore the relation between negative affect processing and smoking cessation failure and support the potential worth of smoking cessation interventions that address negative affect including pharmacotherapies and psychological interventions that have been adapted for smoking cessation or combined with standard cessation treatment such as Acceptance and Commitment Therapy (Gifford et al. 2004), behavioral activation (MacPherson et al. 2010), distress-tolerance treatment (Brown et al. 2008), and mindfulness (Davis et al. 2007). However, it is important to recognize that the particular information processing effects reported in this research may not play any direct causal role in cessation failure; the effects may predict outcome only because they index negative affect.
Some limitations of this study need to be acknowledged. First, the effects obtained were small in magnitude (Cohen 1992). Many factors cause people to be slower or faster on a task (for example, age, which we controlled for) and to be successful or unsuccessful in quitting smoking. Obviously, executive control deficits are only one such factor. Second, the study design and analyses did not allow us to examine participants' reaction times following neutral versus positive, smoking, or negative slides. Thus, we do not know how smokers with poor versus good outcomes would respond following neutral slides relative to the other slide types. Third, in the nicotine-deprived session, participants completed the task while deprived of both nicotine and caffeine, and therefore we cannot determine whether the limited effects found for the deprived versus nondeprived session are attributable to nicotine deprivation, caffeine deprivation for those participants who consume caffeine regularly, or both. Finally, we did not ask participants to give a CO sample to confirm their abstinence prior to completing the information processing task while “deprived,” and we did not ask all participants to smoke immediately prior to their nondeprived session to standardize the time elapsed since last cigarette. Nevertheless, participants were required to report smoking within 2 h prior to the nondeprived session, and those who had not smoked within this time period were asked to go outside and smoke prior to completing the task. The study's strengths included a large sample size (N=365) and the use of photographs—which are presumably more ecologically valid than words. Further strengths include the use of multiple cessation outcome indices and the use of a modified Simon task that allowed us to test multiple factors within the same paradigm.
To conclude, this study found that smokers' performance on a modified Simon task (the extent to which they showed less executive control after viewing positive plus smoking slides versus negative slides) predicted poor cessation outcomes. The results suggest that differences in relatively automatic responses to affective cues distinguish smokers who are successful and unsuccessful in the first 8 weeks of a smoking cessation attempt.
Acknowledgments
Timothy B. Baker has served as an investigator on research projects sponsored by pharmaceutical companies including Pfizer, Glaxo Wellcome, Sanofi, and Nabi.
This research was conducted at the University of Wisconsin-Madison and was supported by grant #P50 DA019706 from NIH/ NIDA; by grant #M01 RR03186 from the General Clinical Research Centers Program of the National Center for Research Resources, NIH; by grant 1UL1RR025011 from the Clinical and Translational Science Award (CTSA) program of the National Center for Research Resources, NIH; and by grant #1K05CA139871 from NIH. Medication was provided to participants at no cost under a research agreement with GlaxoSmithKline (GSK); no part of this manuscript was written or edited by anyone employed by GSK. The authors are solely responsible for the analyses, content, and writing of this article. The authors have full control of all primary data, and they agree to allow the journal to review the data if requested.
We declare that this research complies with the current laws of the USA. All participants gave written informed consent, and the study was approved by the University of Wisconsin Health Sciences Institutional Review Board.
We would like to thank the staff at the Center for Tobacco Research and Intervention in the University of Wisconsin School of Medicine and Public Health for their help with this research. We are particularly grateful to Linda Kurowski, Christine Ripley, and Wendy Theobald for their assistance.
Footnotes
Trials involving two neutral slides were included as filler trials and were not analyzed.
The mean arousal and valence ratings for the smoking slides were computed for a set of 36 smoking slides developed by Shi (1998). The current study used a subset of 24 of those 36 smoking slides. Ratings for the individual slides were not accessible.
We also calculated the following attentional bias scores (by subtracting slide–probe match from slide–probe mismatch reaction times) for negative (M=2 ms, SD=67.6), positive (M=−3 ms, SD= 59.6), and smoking slides (M=5 ms, SD=68.2). These findings suggest there was not a meaningful effect of slide–probe match (i.e., sticky attention) for any of the slide types. Although the findings seemingly conflict with findings from the visual probe task discussed earlier, the current study used the modified Simon task which may explain the different findings.
As mentioned earlier, we selected short-term outcomes because we believed long-term outcomes would be less sensitive to baseline information processing biases and more sensitive to fortuitous events. When longer-term outcomes were examined (i.e., 6-month abstinence), task performance did not predict cessation outcome.
These findings were fairly robust when simple contrasts instead of planned Helmert contrasts were used for the Slide Type factor (i.e., when we first tested that the omnibus F-test was significant and then followed-up with simple contrasts for negative versus positive slides and for smoking versus negative slides). For three of the four cessation outcomes, the omnibus F-test showed that the Slide Type× Probe Congruency×Cessation Outcome Measure interaction was significant. (For the cessation outcome abstinence at 8 weeks post-quit, this interaction was not significant, although the effect was in the right direction, p=0.09). We then followed up the three significant omnibus F-tests with simple contrasts. For the first simple contrasts (negative versus positive slides), the Slide Type (negative versus positive slides)×Probe Congruency×Cessation Outcome Measure interaction was significant for the three cessation outcomes. For the second simple contrasts (smoking versus negative slides), we found only a Slide Type (smoking versus negative slides)×Probe Congruency×Abstinence interaction at 1 week post-quit (p=0.01).
Tanya R. Schlam, Sandra J. Japuntich, Megan E. Piper, Rebecca Gloria, and John J. Curtin have no potential conflicts of interest to disclose.
Contributor Information
Tanya R. Schlam, Email: trschlam@ctri.medicine.wisc.edu, Center for Tobacco Research and Intervention, School of Medicine and Public Health, University of Wisconsin, 1930 Monroe St., Suite 200, Madison, WI 53711, USA, Department of Medicine, School of Medicine and Public Health, University of Wisconsin, Madison, WI, USA.
Sandra J. Japuntich, Center for Tobacco Research and Intervention, School of Medicine and Public Health, University of Wisconsin, 1930 Monroe St., Suite 200, Madison, WI 53711, USA, Department of Psychology, University of Wisconsin-Madison, 1202 West Johnson Street, Madison, WI 53706, USA
Megan E. Piper, Center for Tobacco Research and Intervention, School of Medicine and Public Health, University of Wisconsin, 1930 Monroe St., Suite 200, Madison, WI 53711, USA, Department of Medicine, School of Medicine and Public Health, University of Wisconsin, Madison, WI, USA
Rebecca Gloria, Department of Psychology, University of Wisconsin-Madison, 1202 West Johnson Street, Madison, WI 53706, USA.
Timothy B. Baker, Center for Tobacco Research and Intervention, School of Medicine and Public Health, University of Wisconsin, 1930 Monroe St., Suite 200, Madison, WI 53711, USA, Department of Medicine, School of Medicine and Public Health, University of Wisconsin, Madison, WI, USA
John J. Curtin, Department of Psychology, University of Wisconsin-Madison, 1202 West Johnson Street, Madison, WI 53706, USA
References
- Ayduk O, Mendoza-Denton R, Mischel W, Downey G, Peake PK, Rodriguez M. Regulating the interpersonal self: strategic self-regulation for coping with rejection sensitivity. J Pers Soc Psychol. 2000;79:776–792. doi: 10.1037//0022-3514.79.5.776. [DOI] [PubMed] [Google Scholar]
- Baker TB, Piper ME, McCarthy DE, Majeskie MR, Fiore MC. Addiction motivation reformulated: an affective processing model of negative reinforcement. Psychol Rev. 2004;111:33–51. doi: 10.1037/0033-295X.111.1.33. [DOI] [PubMed] [Google Scholar]
- Berridge KC. The debate over dopamine's role in reward: the case for incentive salience. Psychopharmacol (Berl) 2007;191:391–431. doi: 10.1007/s00213-006-0578-x. [DOI] [PubMed] [Google Scholar]
- Bolt DM, Piper ME, McCarthy DE, Japuntich SJ, Fiore MC, Smith SS, Baker TB. The Wisconsin predicting patients' relapse questionnaire. Nicotine Tob Res. 2009;11:481–492. doi: 10.1093/ntr/ntp030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bradley B, Field M, Mogg K, De Houwer J. Attentional and evaluative biases for smoking cues in nicotine dependence: component processes of biases in visual orienting. Behav Pharmacol. 2004;15:29–36. doi: 10.1097/00008877-200402000-00004. [DOI] [PubMed] [Google Scholar]
- Brown RA, Lejuez CW, Kahler CW, Strong DR, Zvolensky MJ. Distress tolerance and early smoking lapse. Clin Psychol Rev. 2005;25:713–733. doi: 10.1016/j.cpr.2005.05.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown RA, Palm KM, Strong DR, Lejuez CW, Kahler CW, Zvolensky MJ, Hayes SC, Wilson KG, Gifford EV. Distress tolerance treatment for early-lapse smokers: rationale, program description, and preliminary findings. Behav Modif. 2008;32:302–332. doi: 10.1177/0145445507309024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen J. A power primer. Psychol Bull. 1992;112:155–159. doi: 10.1037//0033-2909.112.1.155. [DOI] [PubMed] [Google Scholar]
- Cohen J, Cohen P, West SG, Aiken LS. Lawrence Erlbaum Associates. 3rd. Lawrence Erlbaum Associates; Hillsdale, NJ: 2003. Applied multiple regression/correlation analysis in the behavioral sciences. [Google Scholar]
- Cox WM, Fadardi JS, Pothos EM. The addiction-Stroop test: theoretical considerations and procedural recommendations. Psychol Bull. 2006;132:443–476. doi: 10.1037/0033-2909.132.3.443. [DOI] [PubMed] [Google Scholar]
- Curtin JJ, McCarthy DE, Piper ME, Baker TB. Implicit and explicit drug motivational processes: a model of boundary conditions. In: Weirs RW, Stacy AW, editors. Handbook of implicit cognition and addiction. Sage; Thousand Oaks: 2006. pp. 233–250. [Google Scholar]
- Davis JM, Fleming MF, Bonus KA, Baker TB. A pilot study on mindfulness based stress reduction for smokers. BMC Complement Altern Med. 2007;7:2. doi: 10.1186/1472-6882-7-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dawkins L, Powell JH, West R, Powell J, Pickering A. A double-blind placebo-controlled experimental study of nicotine: II—effects on response inhibition and executive functioning. Psychopharmacol (Berl) 2007;190:457–467. doi: 10.1007/s00213-006-0634-6. [DOI] [PubMed] [Google Scholar]
- Elliott R, Rubinsztein JS, Sahakian BJ, Dolan RJ. The neural basis of mood-congruent processing biases in depression. Arch Gen Psychiatry. 2002;59:597–604. doi: 10.1001/archpsyc.59.7.597. [DOI] [PubMed] [Google Scholar]
- Erickson K, Drevets WC, Clark L, Cannon DM, Bain EE, Zarate CA, Jr, Charney DS, Sahakian BJ. Mood-congruent bias in affective go/no-go performance of unmedicated patients with major depressive disorder. Am J Psychiatry. 2005;162:2171–2173. doi: 10.1176/appi.ajp.162.11.2171. [DOI] [PubMed] [Google Scholar]
- Field M, Mogg K, Bradley BP. Eye movements to smoking-related cues: effects of nicotine deprivation. Psychopharmacol (Berl) 2004;173:116–123. doi: 10.1007/s00213-003-1689-2. [DOI] [PubMed] [Google Scholar]
- Fiore MC, Jaen CR, Baker TB, Bailey WC, Benowitz N, Curry SJ, Dorfman SF, Froelicher ES, Goldstein MG, Healton CG, Henderson PN, Heyman RB, Koh HK, Kottke TE, Lando HA, Mecklenburg RE, Mermelstein RJ, Mullen PD, Orleans CT, Robinson L, Stitzer M, Tommasello AC, Villejo L, Wewers ME. Treating tobacco use and dependence: 2008 update. Rockville, MD: US Department of Health and Human Services, US Public Health Service, US Department of Health and Human Services, US Public Health Service; 2008. [Google Scholar]
- Forster KI, Forster JC. DMDX: a windows display program with millisecond accuracy. Behav Res Meth Instrum Comput. 2003;35:116–124. doi: 10.3758/bf03195503. [DOI] [PubMed] [Google Scholar]
- Fozard JL, Vercryssen M, Reynolds SL, Hancock PA, Quilter RE. Age differences and changes in reaction time: the Baltimore Longitudinal Study of Aging. J Gerontol. 1994;49:179–189. doi: 10.1093/geronj/49.4.p179. [DOI] [PubMed] [Google Scholar]
- Franken IH. Drug craving and addiction: integrating psychological and neuropsychopharmacological approaches. Prog Neuropsychopharmacol Biol Psychiatry. 2003;27:563–579. doi: 10.1016/S0278-5846(03)00081-2. [DOI] [PubMed] [Google Scholar]
- Gifford EV, Kohlenberg BS, Hayes SC, Antonuccio DO, Piasecki MM, Rasmussen-Hall ML, Palm KM. Acceptance-based treatment for smoking cessation. Behav Ther. 2004;35:689–705. [Google Scholar]
- Gloria R, Angelos L, Schaefer HS, Davis JM, Majeskie M, Richmond BS, Curtin JJ, Davidson RJ, Baker TB. An fMRI investigation of the impact of withdrawal on regional brain activity during nicotine anticipation. Psychophysiology. 2009;46:681–693. doi: 10.1111/j.1469-8986.2009.00823.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heatherton TF, Kozlowski LT, Frecker RC, Fagerstrom KO. The Fagerstrom test for nicotine dependence: a revision of the Fagerstrom tolerance questionnaire. Br J Addict. 1991;86:1119–1127. doi: 10.1111/j.1360-0443.1991.tb01879.x. [DOI] [PubMed] [Google Scholar]
- Kashdan TB, Barrios V, Forsyth JP, Steger MF. Experiential avoidance as a generalized psychological vulnerability: comparisons with coping and emotion regulation strategies. Behav Res Ther. 2006;44:1301–1320. doi: 10.1016/j.brat.2005.10.003. [DOI] [PubMed] [Google Scholar]
- Kenford SL, Smith SS, Wetter DW, Jorenby DE, Fiore MC, Baker TB. Predicting relapse back to smoking: contrasting affective and physical models of dependence. J Consult Clin Psychol. 2002;70:216–227. [PubMed] [Google Scholar]
- Lang PJ, Bradley MM, Cuthbert BN. Center for Research in Psychophysiology, University of Florida, Center for Research in Psychophysiology. Gainesville, FL: University of Florida; 1999. International affective picture system (IAPS): Instruction manual and affective ratings Technical Report A-4. [Google Scholar]
- Leventhal AM, Waters AJ, Breitmeyer BG, Miller EK, Tapia E, Li Y. Subliminal processing of smoking-related and affective stimuli in tobacco addiction. Exp Clin Psychopharmacol. 2008;16:301–312. doi: 10.1037/a0012640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Littel M, Franken IH. The effects of prolonged abstinence on the processing of smoking cues: an ERP study among smokers, ex-smokers and never-smokers. J Psychopharmacol. 2007;21:873–882. doi: 10.1177/0269881107078494. [DOI] [PubMed] [Google Scholar]
- Lu CH, Proctor RW. The influence of irrelevant location information on performance: a review of the Simon and spatial Stroop effects. Psychon Bull Rev. 1995;2:174–207. doi: 10.3758/BF03210959. [DOI] [PubMed] [Google Scholar]
- MacPherson L, Tull MT, Matusiewicz AK, Rodman S, Strong DR, Kahler CW, Hopko DR, Zvolensky MJ, Brown RA, Lejuez CW. Randomized controlled trial of behavioral activation smoking cessation treatment for smokers with elevated depressive symptoms. J Consult Clin Psychol. 2010;78:55–61. doi: 10.1037/a0017939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCarthy DE, Gloria R, Curtin JJ. Attention bias in nicotine withdrawal and under stress. Psychol Addict Behav. 2009;23:77–90. doi: 10.1037/a0014288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Munafo M, Mogg K, Roberts S, Bradley BP, Murphy M. Selective processing of smoking-related cues in current smokers, ex-smokers and never-smokers on the modified Stroop task. J Psychopharmacol. 2003;17:310–316. doi: 10.1177/02698811030173013. [DOI] [PubMed] [Google Scholar]
- Olson SL, Schilling EM, Bates JE. Measurement of impulsivity: construct coherence, longitudinal stability, and relationship with externalizing problems in middle childhood and adolescence. J Abnorm Child Psychol. 1999;27:151–165. doi: 10.1023/a:1021915615677. [DOI] [PubMed] [Google Scholar]
- Piper ME, Federmen EB, McCarthy DE, Bolt DM, Smith SS, Fiore MC, Baker TB. Using mediational models to explore the nature of tobacco motivation and tobacco treatment effects. J Abnorm Psychol. 2008;117:94–105. doi: 10.1037/0021-843X.117.1.94. [DOI] [PubMed] [Google Scholar]
- Piper ME, Smith SS, Schlam TR, Fiore MC, Jorenby DE, Fraser D, Baker TB. A randomized placebo-controlled clinical trial of five smoking cessation pharmacotherapies. Arch Gen Psychiatry. 2009;66:1253–1262. doi: 10.1001/archgenpsychiatry.2009.142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shi FY. Dissertation. University of Wisconsin-Madison; Madison, WI: 1998. Smoking motivation, nicotine withdrawal and the startle probe response. [Google Scholar]
- Shiffman S, Scharf DM, Shadel WG, Gwaltney CJ, Dang Q, Paton SM, Clark DB. Analyzing milestones in smoking cessation: illustration in a nicotine patch trial in adult smokers. J Consult Clin Psychol. 2006;74:276–285. doi: 10.1037/0022-006X.74.2.276. [DOI] [PubMed] [Google Scholar]
- Shoda Y, Mischel W, Peake PK. Predicting adolescent cognitive and self-regulatory competencies from preschool delay of gratification: identifying diagnostic conditions. Dev Psychol. 1990;26:978–986. [Google Scholar]
- Simon JR, Rudell AP. Auditory S–R compatibility: the effect of an irrelevant cue on information processing. J Appl Psychol. 1967;51:300–304. doi: 10.1037/h0020586. [DOI] [PubMed] [Google Scholar]
- Thush C, Wiers RW, Ames SL, Grenard JL, Sussmann S, Stacy AW. Interactions between implicit and explicit cognition and working memory capacity in the prediction of alcohol use in at-risk adolescents. Drug Alcohol Depend. 2008;94:116–124. doi: 10.1016/j.drugalcdep.2007.10.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tiffany ST. A cognitive model of drug urges and drug-use behavior: role of automatic and nonautomatic processes. Psychol Rev. 1990;97:147–168. doi: 10.1037/0033-295x.97.2.147. [DOI] [PubMed] [Google Scholar]
- Waters AJ, Shiffman S, Bradley BP, Mogg K. Attentional shifts to smoking cues in smokers. Addiction. 2003a;98:1409–1417. doi: 10.1046/j.1360-0443.2003.00465.x. [DOI] [PubMed] [Google Scholar]
- Waters AJ, Shiffman S, Sayette MA, Paty JA, Gwaltney CJ, Balabanis MH. Attentional bias predicts outcome in smoking cessation. Health Psychol. 2003b;22:378–387. doi: 10.1037/0278-6133.22.4.378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Welsch SK, Smith SS, Wetter DW, Jorenby DE, Fiore MC, Baker TB. Development and validation of the Wisconsin Smoking Withdrawal Scale. Exp Clin Psychopharmacol. 1999;7:354–361. doi: 10.1037//1064-1297.7.4.354. [DOI] [PubMed] [Google Scholar]
- Wiers RW, Houben K, Smulders FTY, Conrod PJ, Jones BT. To drink or not to drink: the role of automatic and controlled cognitive processes in the etiology of alcohol-related problems. In: Wiers RW, Stacy AW, editors. Handbook of implicit cognition and addiction. Sage; Thousand Oaks: 2006. pp. 339–361. [Google Scholar]
- Williams JMG, Mathews A, MacLeod C. The emotional Stroop task and psychopathology. Psychol Bull. 1996;120:3–24. doi: 10.1037/0033-2909.120.1.3. [DOI] [PubMed] [Google Scholar]