

Abstract
Caterpillar dermatitis (lepidopterism) is a disease that is caused by butterflies, moths and their caterpillars. Clinical signs and symptoms vary from itchy skin lesions to conjunctivitis, pharyngitis, malaise and anaphylactic reactions. We present the case of two brothers with typical skin lesions of leptidopterism. The older boy showed skin lesions after playing with caterpillars in the garden, whereas his younger brother was affected without direct contact to the caterpillars but only by playing with his brother. As the mother could show two caterpillars, lepidopterism could easily be diagnosed. Under a local therapy with a medium potent corticosteroid cream and a non-sedating orally administered antihistamine, all skin lesions as well as itching disappeared within 1 week.
Background
Lepidopterism is a disease that is triggered by the hairs of butterflies, moths and their caterpillars.1–5 In Central Europe, the two main causes of caterpillar dermatitis are the oak and pine processionary caterpillar. Due to climate changes in the recent years and a tendency towards warmer summers, an ongoing broadening from southwest to northeast and an increase in cases with lepidopterism is probable.1 6 We present this case to show typical clinical signs and symptoms of lepidopterism that is still unfamiliar to many physicians.
Case presentation
We report on two brothers at the age of 2 and 4 years who developed itchy maculopapulous lesions in June that showed partly urticaria-like infiltrates and several vesicles especially on uncovered skin. The elder brother had played in the garden 1 day ago and had played with a fallen nest of caterpillars. One hour later, he first developed urticaria-like lesions in his hands, followed by lesions in the other parts of his body (figure 1). His younger brother showed similar skin lesions 1 day later, although he had no direct contact with the caterpillars and had not played outside. Both children suffered from strongly itching papulous skin lesions with pronounced urticarial infiltrate and central blistering, especially on the uncovered parts of the body. They showed no conjunctivitis-like or pulmonary symptoms. As their mother was able to show the caterpillars suspicious of being the elicitors (figure 2), the diagnosis of caterpillar dermatitis could easily be made. Under a local therapy with a medium potent corticosteroid cream and a non-sedating orally administered antihistamine, all skin lesions as well as itching disappeared within 1 week.
Figure 1.

Maculopapulous lesions with surrounding urticaria-like infiltrate in the axilla (A), on the hands (B) and arms (C). Several skin lesions show a central vesiculous blistering (D).
Figure 2.
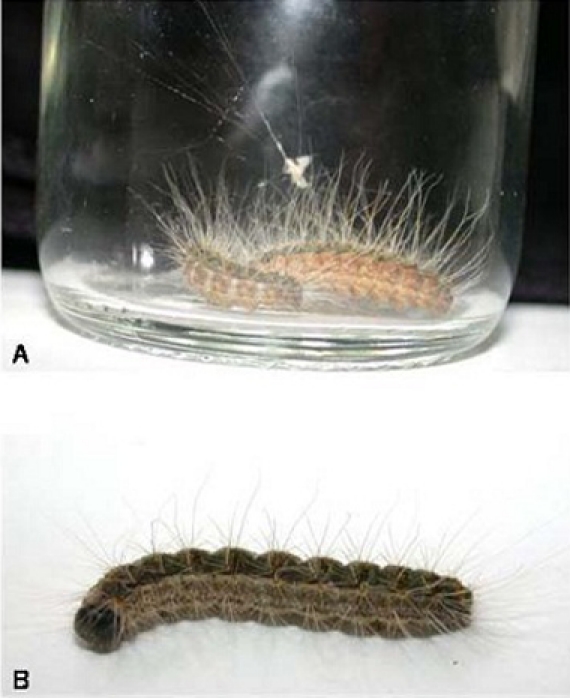
Caterpillars from the fallen nest with typical yellow-brown sides (A) and green-brownish back (B).
Differential diagnosis
Differential diagnosis includes strophulus infantum, insect or flea bites, contact urticaria, polymorphous light eruption, irritant dermatitis of another cause and drug-induced exanthema. In case of rhinoconjunctival or asthmatic symptoms, hay fever or allergic asthma bronchiale should be taken into consideration.
Treatment
Under a local therapy with a medium potent corticosteroid cream and a non-sedating orally administered antihistamine, all skin lesions as well as itching disappeared within 1 week.
Outcome and follow-up
All skin lesions healed without scars.
Discussion
The oak processionary caterpillar (Thaumetopoea processionea) is a moth that affects trees in south or southwest exposition. In Central Europe, it is predominantly found in sunny and dry hollows.1 6 Due to climate changes in the recent years and a tendency towards warmer summers, an ongoing broadening from southwest to northeast is probable.1 6 Presumably, the yearly incidence of 100–100 cases will rise too. The dissemination of caterpillar hairs through the air or by contact with contaminated clothes is possible. One remarkable case is caterpillar dermatitis in a couple caused by indirect contact via their dog’s saliva after the dog had played with a fallen caterpillar nest.6 In the case of the children presented here, the younger brother was also affected without direct contact to the caterpillars but only by playing with his brother.
The oak processionary caterpillar can cause epidemic outbreaks of lepidopterism, especially between the end of April and the beginning of July. Gottschling and Meyer7 reported caterpillar dermatitis in a group of 90 persons who visited a recreational area at the border between Germany and France where oaks infested with the oak processionary caterpillar were found. Half of the group suffered from itching and weal and flare lesions and could be treated with antihistamines; five patients showed more severe symptoms such as bronchoconstriction, cough, wheeze and angiooedema and needed systemic steroids. In most cases, like in the case of the brothers presented here, a therapy including topical corticosteroid creams and the application of non-sedating antihistamines is sufficient. Hospitalisation and administration of systemic steroids or epinephrine is indicated only in cases with asthmatic symptoms, angioedema or anaphylactic reaction.
Learning points.
-
▶
Caterpillar dermatitis should be considered in the differential diagnosis in cases with itching papulous and urticaria-like skin lesions or patients with rhinoconjunctival or asthmatic symptoms.
-
▶
Trips in affected woods or parks should be avoided from April to September. Local forestry offices inform about possible affection.
-
▶
Caterpillars and nests should not be touched and only be removed by specialised companies.
-
▶
If skin lesions develop, clothes must be changed and washed in the washing machine. Patients should take a shower and wash their hair.
-
▶
In case of skin lesions or general symptoms, a physician should be contacted and informed about contact to caterpillar hairs.
-
▶
Allergic patients or patients with asthma who live in regions at risk should be equipped with an emergency pack containing an orally administrable corticoid and antihistamine and when indicated an epinephrine injector or inhaler.
Footnotes
Competing interests None.
Patient consent Obtained.
References
- 1.Diaz JH. The evolving global epidemiology, syndromic classification, management, and prevention of caterpillar envenoming. Am J Trop Med Hyg 2005;72:347–57 [PubMed] [Google Scholar]
- 2.Lamy M. Contact dermatitis (erucism) produced by processionary caterpillars (genus Thaumetopoea). J Appl Entomol 1990;110:425–37 [Google Scholar]
- 3.Werno J, Lamy M, Vincendeau P. Caterpillar hairs as allergens. Lancet 1993;342:936–7 [DOI] [PubMed] [Google Scholar]
- 4.Vega JM, Moneo I, Armentia A, et al. Pine processionary caterpillar as a new cause of immunologic contact urticaria. Contact Derm 2000;43:129–32 [DOI] [PubMed] [Google Scholar]
- 5.Santos-Magadán S, González de Olano D, Bartolomé-Zavala B, et al. Adverse reactions to the processionary caterpillar: irritant or allergic mechanism? Contact Derm 2009;60:109–10 [DOI] [PubMed] [Google Scholar]
- 6.Maronna A, Stache H, Sticherling M. Lepidopterism - oak processionary caterpillar dermatitis: appearance after indirect out-of-season contact. J Dtsch Dermatol Ges 2008;6:747–50 [DOI] [PubMed] [Google Scholar]
- 7.Gottschling S, Meyer S. An epidemic airborne disease caused by the oak processionary caterpillar. Pediatr Dermatol 2006;23:64–6 [DOI] [PubMed] [Google Scholar]