

Abstract
Menstrually related migraine (MRM) is a particularly difficult-to-treat pain condition, associated with substantial disability. Aim of this study was to compare the efficacy and safety of frovatriptan and zolmitriptan in the treatment of MRM attacks, analyzing data from a multicenter, randomized, double blind, cross-over study. We analyzed the subset of 76 regularly menstruating women who participated in one head-to-head multicenter, randomized, double blind, cross-over clinical trial and who took the study drugs to treat MRM attacks. In a randomized sequence, each patient received frovatriptan 2.5 mg or zolmitriptan 2.5 mg: after treating three episodes of migraine in no more than 3 months with the first treatment, the patient had to switch to the other treatment. MRM was defined according to the criteria listed in the Appendix of the last Classification of Headache disorders of the International Headache Society. A total of 73 attacks, classified as MRM, were treated with frovatriptan and 65 with zolmitriptan. Rate of pain relief at 2 h was 52% for frovatriptan and 53% for zolmitriptan (p = NS), while rate of pain free at 2 h was 22 and 26% (p = NS), respectively. At 24 h, 74 and 83% of frovatriptan-treated and 69 and 82% of zolmitriptan-treated patients were pain free and had pain relief, respectively (p = NS). Recurrence at 24 h was significantly (p < 0.05) lower with frovatriptan (15 vs. 22% zolmitriptan). Frovatriptan proved to be effective in the immediate treatment of MRM attacks, similarly to zolmitriptan, but showed lower recurrence rates, and thus a better sustained relief.
Keywords: Frovatriptan, Migraine attacks, MRM, Zolmitriptan
Introduction
Migraine is a particularly frequent disease in women of fertile age, in whom it usually occurs in the perimenstrual period [1]. Menstrually related migraine (MRM) is associated with substantial disability and attacks are more severe, longer in duration, and have a poorer response to analgesics than non-menstrual ones [2]. Drug prophylaxis may be useful for menstrual migraine [3]. However, since this type of migraine is characterized by relatively low attack frequency, acute treatment may be more indicated [4].
Triptans proved to be the most effective specific acute antimigraine medications and are preferable for MRM treatment in view of its difficult-to-treat nature [4, 5]. Prospective, randomized, controlled trials as well as retrospective analyses and open label studies support the use of triptans as acute therapy for menstrual migraine [5]. Sumatriptan has been shown to be well tolerated and effective in providing pain relief in MRM when administered in the mild pain phase, also in combination with analgesics [6–12]. Second generation triptans such as zolmitriptan [13–15], naratriptan [16], rizatriptan [17–21] and more recently almotriptan [14, 22] and frovatriptan [23] have been also successfully tested, their different pharmacokinetic and pharmacodynamic features as respect to sumatriptan potentially rendering them particularly suitable for treating menstrual migraine. Recent guidelines now recommend sumatriptan 50 and 100 mg or rizatriptan 10 mg for acute treatment of MRM, and frovatriptan 2.5 mg or naratriptan 1 mg twice daily for preventive treatment of this condition [4, 24].
Though there is presently strong evidence of the preventive efficacy of frovatriptan [25–28], there is less information on its efficacy in treating acute MRM attacks of menstrual migraine. In addition, there are presently no head-to-head studies comparing efficacy of frovatriptan with that of another second generation triptan in menstrual migraineurs.
In order to fill this gap we planned an analysis of a subgroup of MRM sufferers who participated in a recently published head-to-head multicenter, randomized, double blind, cross-over clinical trial comparing the efficacy of frovatriptan versus zolmitriptan [29]. Results of such a subgroup analysis are reported in the present paper.
Methods
Study population
The main study foresaw inclusion of subjects of both genders, aged 18–65 years, with a current history of migraine with or without aura, according to International Headache Society (IHS) 2004 criteria, and with at least one, but no more than six migraine attacks per month for 6 months prior to entering the study [29, 30]. Details of study design, including exclusion criteria, are available from the main study publication [29]. In the present analysis women with MRM were selected. This condition was defined according to IHS criteria as migraine without aura attacks in a menstruating woman, occurring on day 1 ± 2 (namely days −2 to +3) of menstruation in at least two out of three menstrual cycles and additionally at other times of the cycle [30].
Study design
The study design has been extensively reported in a previous publication [29]. Briefly, this was a multicenter, randomized, double blind, cross-over study, including 14 Italian centers (see Appendix). Each patient received frovatriptan 2.5 mg or zolmitriptan 2.5 mg in a randomized sequence: after treating three episodes of migraine in no more than 3 months with the first treatment, the patient had to switch to the other treatment. Subjects were encouraged to treat one to three attacks for a maximum period of 6 months and to visit the center three times. Subjects having no migraine episodes during one of the two observation periods were excluded from the study.
Data analysis
This analysis was carried out in all normally menstruating women randomized to any of the two treatment sequences, having not positively refused to receive either study treatment and having treated at least one episode of menstrual migraine with both medications (intention-to-treat population).
Study endpoints were (1) the number of pain-relief episodes at 2 and 24 h; (2) the decrease in migraine intensity from severe or moderate to mild or none at 2 and 24 h; (3) the number of pain-free episodes at 2 and 24 h (absence of migraine episodes at 2 and 24 h after intake of one dose of study drug ± rescue medication]; (4) recurrence, defined as an episode of migraine occurring 24 h after the previous episode, with a migraine-free period between the two attacks.
Analysis of pain-free episodes was carried out also according to baseline headache intensity (mild, moderate or severe). Frequency of pain-free and pain-relief episodes was also assessed and compared between MRM and non-MRM attacks.
Continuous variables were summarized by computing average values and standard deviation (SD), while categorical variables by computing the absolute value and the frequency (as percentage). Endpoints were compared between groups by generalized estimating equation analysis. Kaplan–Meyer curves for cumulative hazard of recurrence over the 48 h were also drawn. P value refers to the statistical significance of between-treatment difference. The level of statistical significance was kept at 0.05 throughout the whole study.
Results
The main study population consisted of 107 subjects, of which 85 women [29]. Overall 76 out of the 85 women had a regular menstrual cycle and were thus included in this analysis.
Average subjects’ age was 34 ± 8 years, age at onset of migraine was 17 ± 5 years, proportion of migraine attack duration >2 days was 20% and average MIDAS score was 22 ± 18. No statistically significant differences were observed between the main study and MRM subgroup population.
Overall efficacy of study drugs
A total of 73 attacks (32% of all attacks) classified as MRM were treated with frovatriptan and 65 (30%) with zolmitriptan.
Rate of pain-relief episodes at 2 h was similar (p = NS) between frovatriptan (52%) and zolmitriptan (53%). The same figure applied to the rate of pain relief at 24 h (83% frovatriptan vs. 82% zolmitriptan, p = NS). Also the rate of pain-free episodes at 2 and 24 h did not differ between the two treatment groups (22 and 74% frovatriptan vs. 26 and 69% zolmitriptan; p = NS for both) (Table 1).
Table 1.
Results for the comparison of study endpoints between the two treatment groups
| Frovatriptan | Zolmitriptan | p | |
|---|---|---|---|
| Pain-relief episodes at 2 h | 31 (52) | 26 (53) | NS |
| Pain-free episodes at 2 h | 16 (22) | 17 (26) | NS |
| Pain-relief episodes at 24 h | 50 (83) | 40 (82) | NS |
| Pain-free episodes at 24 h | 54 (74) | 45 (69) | NS |
| Recurrent episodes at 24 h | 11 (15) | 14 (22) | <0.05 |
Data are reported as absolute (n) and relative (%) frequency. P refers to the statistical significance of the difference between the two study drugs
Conversely, the risk of recurrence over the 24 h was significantly (p < 0.05) lower under frovatriptan than under zolmitriptan (15 vs. 22%). This was the case also when recurrence was expressed as cumulative hazard ratio over the observation period (Fig. 1).
Fig. 1.
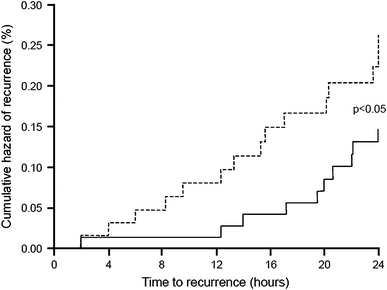
Cumulative hazard of recurrence over the 24 h during treatment with frovatriptan (continuous line) or zolmitriptan (dashed line) in the 76 women with MRM
Efficacy of study drugs according to baseline migraine intensity
Most of the treated attacks had a baseline moderate or severe intensity. In these attacks the rates of pain free at 2 or 24 h were slightly larger in frovatriptan- than in zolmitriptan-treated patients, especially at 2 h (Table 2).
Table 2.
Pain-free episodes at 2 and 24 h according to baseline headache intensity in the two treatment groups
| Frovatriptan | Zolmitriptan | p | |
|---|---|---|---|
| Pain-free episodes at 2 h | |||
| Mild | 5 (31) | 8 (47) | NS |
| Moderate–severe | 11 (69) | 9 (53) | |
| Pain-free episodes at 24 h | |||
| Mild | 11 (20) | 11 (24) | NS |
| Moderate–severe | 43 (80) | 34 (76) | |
Data are reported as absolute (n) and relative (%) frequency. P refers to the statistical significance of the difference between the two study drugs
MRM and non-MRM attacks
Table 3 shows the number and proportion of pain-free and pain-relief episodes 2 and 24 h after frovatriptan intake for the 73 attacks related to and for the 156 attacks unrelated to the menstrual cycle. Frequency of pain relief at 2 and 24 h was 52 and 83% in menstrually related attacks and 63 and 90% in non-menstrually related attacks, with no statistically significant difference between the two type of migraine (p = NS). Similarly, the rate of pain-free episodes at 2 and 24 h was 22 and 74% in MRM and 28 and 81% in non-MRM (p = NS).
Table 3.
Pain-free and pain-relief episodes at 2 and 24 h in MRM (n = 73) and non-MRM (n = 156) attacks treated with frovatriptan
| MRM | Non-MRM | p | |
|---|---|---|---|
| Pain-relief episodes at 2 h | 31 (52) | 82 (63) | NS |
| Pain-free episodes at 2 h | 16 (22) | 43 (28) | NS |
| Pain-relief episodes at 24 h | 50 (83) | 118 (90) | NS |
| Pain-free episodes at 24 h | 54 (74) | 127 (81) | NS |
Data are reported as absolute (n) and relative (%) frequency. P refers to the statistical significance of the difference between the two types of migraine attacks
Discussion
In this analysis acute treatment of MRM with frovatriptan and zolmitriptan resulted in similar proportions of pain-relief episodes at 2 and 24 h and of pain-free episodes at 2 and 24 h, indicating a superimposable efficacy of the two triptans. However, as respect to zolmitriptan, frovatriptan showed lower rates of headache recurrence over the 24 h. These differences in efficacy between the two study drugs may be largely attributable to the different pharmacokinetics of the two compounds. Zolmitriptan has a slightly shorter time to maximum concentration than frovatriptan (1.5 h vs. 2–4 h), but frovatriptan has a longer half-life than zolmitriptan (25–26 h vs. 3 h), which might explain the same frequencies of pain-relief and pain-free episodes with the two study drugs and why frovatriptan, unlike zolmitriptan, greatly reduced the risk of migraine recurrence [31–33]. Interestingly, frovatriptan showed a similar efficacy in MRM and non-MRM episodes, this being particularly important since MRM attacks are usually longer lasting, more severe and more difficult to treat than non-menstrually related ones.
This is the first study proving the efficacy of frovatriptan as acute treatment of MRM. The finding adds to and completes that of previous efficacy studies of frovatriptan as intermittent preventive therapy for menstrual migraine: frovatriptan started 2 days before the expected onset of headache and continued for 6 days, was always found superior to placebo in reducing the frequency of menstrual migraine. A randomized, double-blind, placebo controlled study involving 410 women showed a headache incidence of only 8% when frovatriptan was given at dosage of 2.5 mg twice-daily and of 31% when given once-daily, while the incidence was 58% under placebo [26]. A post-hoc analysis of a randomized, double-blind, placebo controlled study in a population of 179 women experiencing MRM showed a significantly less prevalence of this condition with frovatriptan 2.5 mg twice (38%) or once-daily (51%) than with placebo (67%) [27]. These latter results are in line with those of a previous randomized, double-blind, placebo-controlled study of the same authors carried out in 546 women migraineurs [28].
As regards zolmitriptan, some evidence as acute treatment of menstrual migraine is available from the literature and thus a comparison may be inferred from previous studies. In published studies pain relief at 2 h with zolmitriptan ranged between 48 and 69% [13–15], pain free at 2 h between 28 and 41% [13, 14] and recurrence at 24 h between 29 and 35% [13, 14]: in our study the corresponding figures for zolmitriptan were very similar with respect to pain relief at 2 h (53%) and slightly lower for pain free at 2 h (26%) and recurrence at 24 h (22%). These differences might be attributed to differences in study design, patients’ characteristics and dose of zolmitriptan employed.
This is also the first direct comparison study between frovatriptan and another triptan in MRM. Our study and a comparison study between almotriptan and zolmitriptan [14] are the only two available head-to-head double-blind, randomized studies comparing the efficacy of two triptans in MRM. Though both studies share the limitations of post-hoc analysis, they are useful because no such prospective studies on triptans in menstrual migraine have yet been carried out. Limitations of our study are at least partially contrasted by the large number of subjects included in the analysis, approximating two-third of those of the main study. In addition, baseline characteristic of our subgroup of migraineurs were quite similar to those of the main study population and the results for the efficacy endpoints explored and for frovatriptan were not different for MRM and non-MRM attacks [29]. We also limited as much as possible the number of endpoints and analyses, and the study assumptions, considering this subgroup analysis as a starting point for subsequent clinical trials to confirm or refute the finding, rather than being viewed as a definitive result.
Thus, the good sustained relief shown by frovatriptan in our study, seems to support indication of frovatriptan not only, as previously suggested, for preventive treatment of MRM [24], but also for managing the acute attack. Though frovatriptan and zolmitriptan showed a similar efficacy in the immediate, the sustained analgesic effect of frovatriptan supported by a lesser risk of recurrence makes this drug the best choice for those patients with long-duration or recurrent migraine attacks [34, 35].
Conclusions
Our analysis of data from a multicenter, randomized, double-blind, head-to-head study suggests that frovatriptan and zolmitriptan are similarly effective in the immediate treatment of women with MRM. The study provides the first evidence that frovatriptan is superior to zolmitriptan in reducing recurrence in menstrual migraine patients, showing a better sustained relief.
Acknowledgments
The present study was supported by Istituto Lusofarmaco d’Italia.
Conflict of interest
All authors have occasionally served as scientific consultants for manufacturers of frovatriptan or zolmitriptan. Dario Zava is an employee of the manufacturer of frovatriptan.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Appendix: List of study sites
Coordinator: G. Bussone (Milan)
Investigators: M. Gionco (Turin), C. Benedetto, G.Allais (Turin), M. Aguggia (Novi Ligure/Asti), B. Colombo (Milan), M. Turla (Esine), F. Perini (Vicenza), A. Ganga (Sassari), E. Agostoni (Lecco), C. Narbone (Messina), A. Moschiano (Merate), M. Vacca (Cagliari), M. Bartolini (Ancona), A. Ambrosini (Pozzilli), R. De Simone (Napoli), V. Petretta, F. D’Onofrio (Avellino), G. Reggiardo (Biostatistical Unit, Mediservice, Milan), F. Sacchi (Clinical Unit, Mediservice, Milan), A. Camagni (Istituto Lusofarmaco d’Italia, Milan).
References
- 1.Martin VT, Lipton RB. Epidemiology and biology of menstrual migraine. Headache. 2008;48(Suppl. 3):S124–S130. doi: 10.1111/j.1526-4610.2008.01310.x. [DOI] [PubMed] [Google Scholar]
- 2.Allais G, Castagnoli Gabellari I, De Lorenzo C, Mana O, Benedetto C. Menstrual migraine: clinical and therapeutical aspects. Expert Rev Neurother. 2007;7:1105–1120. doi: 10.1586/14737175.7.9.1105. [DOI] [PubMed] [Google Scholar]
- 3.Recober A, Geweke LO. Menstrual migraine. Curr Neurol Neurosci Rep. 2005;5:93–98. doi: 10.1007/s11910-005-0005-4. [DOI] [PubMed] [Google Scholar]
- 4.MacGregor EA. Prevention and treatment of menstrual migraine. Drugs. 2010;70:1799–1818. doi: 10.2165/11538090-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 5.Mannix LK, Files JA. The use of triptans in the management of mestrua migraine. CNS Drugs. 2005;19:951–972. doi: 10.2165/00023210-200519110-00005. [DOI] [PubMed] [Google Scholar]
- 6.Facchinetti F, Allais G, Nappi RE, Gabellari IC, Di Renzo GC, Genazzani AR, Bellafronte M, Roncolato M, Benedetto C. Sumatriptan (50 mg tablets vs. 25 mg suppositories) in the acute treatment of menstrually related migraine and oral contraceptive-induced menstrual migraine: a pilot study. Gynecol Endocrinol. 2010;26:773–779. doi: 10.3109/09513590.2010.487607. [DOI] [PubMed] [Google Scholar]
- 7.Mannix LK, Martin VT, Cady RK, Diamond ML, Lener SE, White JD, Derosier FJ, McDonald SA. Combination treatment for menstrual migraine and dysmenorrhea using sumatriptan-naproxen: two randomized controlled trials. Obstet Gynecol. 2009;114:106–113. doi: 10.1097/AOG.0b013e3181a98e4d. [DOI] [PubMed] [Google Scholar]
- 8.Schreiber CP, Cady RK. Diagnosis of menstrual headache and an open-label study among those with previously undiagnosed menstrually related migraine to evaluate the efficacy of sumatriptan 100 mg. Clin Ther. 2007;29(Suppl):2511–2519. doi: 10.1016/j.clinthera.2007.11.018. [DOI] [PubMed] [Google Scholar]
- 9.Dowson AJ, Massiou H, Aurora SK. Managing migraine headaches experienced by patients who self-report with menstrually related migraine: a prospective, placebo-controlled study with oral sumatriptan. J Headache Pain. 2005;6:81–87. doi: 10.1007/s10194-005-0156-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Landy S, Savani N, Shackelford S, Loftus J, Jones M. Efficacy and tolerability of sumatriptan tablets administered during the mild-pain phase of menstrually associated migraine. Int J Clin Pract. 2004;58:913–919. doi: 10.1111/j.1368-5031.2004.00295.x. [DOI] [PubMed] [Google Scholar]
- 11.Nett R, Landy S, Shackelford S, Richardson MS, Ames M, Lener M. Pain-free efficacy after treatment with sumatriptan in the mild pain phase of menstrually associated migraine. Obstet Gynecol. 2003;102:835–842. doi: 10.1016/S0029-7844(03)00659-8. [DOI] [PubMed] [Google Scholar]
- 12.Salonen R, Saiers J. Sumatriptan is effective in the treatment of mestrua migraine: a review of prospective studies and retrospective analyses. Cephalalgia. 1999;19:16–19. doi: 10.1111/j.1468-2982.1999.1901016.x. [DOI] [PubMed] [Google Scholar]
- 13.Tuchman M, Hee A, Emeribe U, Silberstein S. Efficacy and tolerability of zolmitriptan oral tablet in the acute treatment of menstrual migraine. CNS Drugs. 2006;20:1019–1026. doi: 10.2165/00023210-200620120-00005. [DOI] [PubMed] [Google Scholar]
- 14.Allais G, Acuto G, Cabarrocas X, Esbri R, Benedetto C, Bussone G. Efficacy and tolerability of almotriptan versus zolmitriptan for the acute treatment of menstrual migraine. Neurol Sci. 2006;27(Suppl.2):S193–S197. doi: 10.1007/s10072-006-0600-4. [DOI] [PubMed] [Google Scholar]
- 15.Loder E, Silberstein SD, Abu-Shakra S, Mueller L, Smith T. Efficacy and tolerability of oral zolmitriptan in menstrually associated migraine: a randomized, prospective, parallel-group, double-blind, placebo-controlled study. Headache. 2004;44:120–130. doi: 10.1111/j.1526-4610.2004.04027.x. [DOI] [PubMed] [Google Scholar]
- 16.Massiou H, Jamin C, Hinzelin G, Bidaut-Mazel C, French Naramig Collaborative Study Group Efficacy of oral naratriptan in the treatment of menstrually related migraine. Eur J Neurol. 2005;12:774–781. doi: 10.1111/j.1468-1331.2005.01076.x. [DOI] [PubMed] [Google Scholar]
- 17.Bigal M, Sheftell F, Tepper S, Tepper D, Ho TW, Rapoport A. A randomized double-blind study comparing rizatriptan, dexamethasone, and the combination of both in the acute treatment of menstrually related migraine. Headache. 2008;48:1286–1293. doi: 10.1111/j.1526-4610.2008.01092.x. [DOI] [PubMed] [Google Scholar]
- 18.Nett R, Mannix LK, Mueller L, Rodgers A, Hustad CM, Skobieranda F, Ramsey KE. Rizatriptan efficacy in ICHD-II pure menstrual migraine and menstrually related migraine. Headache. 2008;48:1194–1201. doi: 10.1111/j.1526-4610.2008.01093.x. [DOI] [PubMed] [Google Scholar]
- 19.Martin V, Cady R, Mauskop A, Seidman LS, Rodgers A, Hustad CM, Ramsey KE, Skobieranda F. Efficacy of rizatriptan for menstrual migraine in an early intervention model: a prospective subgroup analysis of the rizatriptan TAME (Treat A Migraine Early) studies. Headache. 2008;48:226–235. doi: 10.1111/j.1526-4610.2008.01310.x. [DOI] [PubMed] [Google Scholar]
- 20.Silberstein SD, Massiou H, McCarroll KA, Lines CR. Further evaluation of rizatriptan in menstrual migraine: retrospective analysis of long-term data. Headache. 2002;42:917–923. doi: 10.1046/j.1526-4610.2002.02214.x. [DOI] [PubMed] [Google Scholar]
- 21.Silberstein SD, Massiou H, Le Jeunne C, Johnson-Pratt L, McCarroll KA, Lines CR. Rizatriptan in the treatment of menstrual migraine. Obstet Gynecol. 2000;96:237–242. doi: 10.1016/S0029-7844(00)00880-2. [DOI] [PubMed] [Google Scholar]
- 22.Diamond ML, Cady RK, Mao L, Biondi DM, Finlayson G, Greenberg SJ, Wright P. Characteristics of migraine attacks and responses to almotriptan treatment: a comparison of menstrually related and nonmenstrually related migraines. Headache. 2008;48:248–258. doi: 10.1111/j.1526-4610.2007.01019.x. [DOI] [PubMed] [Google Scholar]
- 23.Newman LC, Harper S, Jones BA, Campbell J. Frovatriptan for acute treatment of migraine associated with menstruation: results from an open-label postmarketing surveillance study. J Womens Health (Larchmt) 2009;18:1265–1273. doi: 10.1089/jwh.2008.1031. [DOI] [PubMed] [Google Scholar]
- 24.Pringsheim T, Davenport WJ, Dodick D. Acute treatment and prevention of menstrually related migraine headache: evidence-based review. Neurology. 2008;70:1555–1563. doi: 10.1212/01.wnl.0000310638.54698.36. [DOI] [PubMed] [Google Scholar]
- 25.MacGregor EA, Pawsey SP, Campbell JC, Hu X. Safety and tolerability of frovatriptan in the acute treatment of migraine and prevention of mestrua migraine: results of a new analysis of data from five previously published studies. Gend Med. 2010;7:88–108. doi: 10.1016/j.genm.2010.04.006. [DOI] [PubMed] [Google Scholar]
- 26.Brandes JL, Poole A, Kallela M, Schreiber CP, MacGregor EA, Silberstein SD, Tobin J, Shaw R. Short-term frovatriptan for the prevention of difficult-to-treat menstrual migraine attacks. Cephalalgia. 2009;29:1133–1148. doi: 10.1111/j.1468-2982.2009.01840.x. [DOI] [PubMed] [Google Scholar]
- 27.Silberstein SD, Berner T, Tobin J, Xiang Q, Campbell JC. Scheduled short-term prevention with frovatriptan for migraine occurring exclusively in association with menstruation. Headache. 2009;49:1283–1297. doi: 10.1111/j.1526-4610.2009.01509.x. [DOI] [PubMed] [Google Scholar]
- 28.Silberstein SD, Elkind AH, Schreiber C, Keywood C. A randomized trial of frovatriptan for the intermittent prevention of menstrual migraine. Neurology. 2004;63:261–269. doi: 10.1212/01.wnl.0000134620.30129.d6. [DOI] [PubMed] [Google Scholar]
- 29.Tullo V, Allais G, Ferrari MD, Curone M, Mea E, Omboni S, Benedetto C, Zava D, Bussone G. Frovatriptan versus zolmitriptan for the acute treatment of migraine: a double-blind, randomized, multicenter, Italian study. Neurol Sci. 2010;31(Suppl. 1):S51–S54. doi: 10.1007/s10072-010-0273-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Headache Classification Subcommittee of the International Headache Society (2004) The International Classification of Headache Disorders, 2nd edn. Cephalalgia 24(Suppl. 1):9–160 [DOI] [PubMed]
- 31.Loder E (2010) Triptan therapy in migraine. N Engl J Med 363:63–70 [DOI] [PubMed]
- 32.Balbisi EA. Frovatriptan succinate, a 5-HT1B/1D receptor agonist for migraine. Int J Clin Pract. 2004;58:695–705. doi: 10.1111/j.1368-5031.2004.00218.x. [DOI] [PubMed] [Google Scholar]
- 33.Markus F, Mikko K. Frovatriptan review. Expert Opin Pharmacother. 2007;8:3029–3033. doi: 10.1517/14656566.8.17.3029. [DOI] [PubMed] [Google Scholar]
- 34.Kelman L. Review of frovatriptan in the treatment of migraine. Neuropsychiatr Dis Treat. 2008;4:49–54. doi: 10.2147/ndt.s1871. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Cady R, Elkind A, Goldstein J, Keywood C. Randomized, placebo-controlled comparison of early use of frovatriptan in a migraine attack versus dosing after the headache has become moderate or severe. Curr Med Res Opin. 2004;20:1465–1472. doi: 10.1185/030079904X2745. [DOI] [PubMed] [Google Scholar]