

Abstract
Objectives
This study aimed to estimate the prevalence of orthodontic treatment in France among children and teenagers aged 8 to 18 years, by sex and by age, and to investigate the specific role of social and economic characteristics on use of orthodontic treatment.
Methods
We analysed data from the cross-sectional national health survey conducted in France in 2002–2003, which included a sample of 5988 children aged 8 to 18 years. All data were collected by interview including the question on orthodontic treatment. Other data used in our study were family social status and income, maternal educational attainment and place of birth, whether the child was covered by a supplementary health insurance and whether the residence was urban or rural. We also calculated the density of orthodontists in the district. Multivariate logistic regression analyses were used to study the relationships between these social and economic factors and orthodontic treatment.
Results
The prevalence of orthodontic treatment was 14% of all children aged 8 to 18, 15% for girls, and 13% for boys, and 23% in the 12 to 15-year age group. Children were less likely to have orthodontic treatment when parents were service or sales workers compared with children whose parents were managers or professionals (aOR=0.50; 95%CI: [0.34;0.76]), when family income was in the lowest, compared with highest quartile (aOR=0,62; 95%CI: [0.45;0.85]), when children had no supplementary insurance compared with children covered by private insurance (aOR=0.53; 95%CI: [0.34;0.81]), or when they lived in rural compared with urban areas (aOR=0.70; 95%CI: [0.54;0.91]).
Conclusion
There are social inequalities in orthodontic treatment in France, associated mainly with social status, annual income, supplementary insurance, and the residence area.
Keywords: Adolescent; Age Distribution; Child; Child, Preschool; Cross-Sectional Studies; Educational Status; Female; France; Health Status Disparities; Healthcare Disparities; Humans; Income; Insurance, Dental; Interviews as Topic; Logistic Models; Male; Multivariate Analysis; Orthodontics, Corrective; economics; statistics & numerical data; Questionnaires; Rural Population; Sex Distribution; Social Class; Urban Population
INTRODUCTION
Malocclusion is any incorrect position of the teeth that results in imperfect contact between mandibular and maxillary teeth (1). According to a US study (2), only 40% of Americans have ideal overjet, 50% ideal incisor overlap and 40% ideal incisor irregularity. The prevalence of malocclusion in the US between 1930 and 1935 was variously estimated as 35% to 95%, depending on investigators’ differing criteria for “how much the deviation from the ideal” is acceptable. Orthodontic treatment globally consists in moving and straightening teeth, to align and level them and to correct the bite (3), and thus achieve a long-lasting balanced occlusion. Nonetheless all malocclusions do not need to be corrected (4). There is no evidence of an association between malocclusions and dental caries (5, 6). Whether malocclusion has a negative effect on periodontal health remains both unclear (7, 8) and controversial (9, 10). Several reviews have concluded that there is no evidence of an improvement in periodontal health associated with orthodontic treatment (10–12). A recent 20-year cohort study in Wales (13), intended to assess the effects of orthodontic treatment on oral health, provided evidence that lack of orthodontic treatment is not associated with psychological difficulties in later life (13, 14) and that orthodontic treatment neither causes nor prevents temporomandibular disorders (15). But it has been suggested that some severe malocclusions should be reduced to enhance the longevity of the dentition (7, 16–18). French guidelines recommend orthodontic treatment when oral and nasal functions are impaired, anterior teeth are exposed to trauma, incorrect tooth alignment increases plaque accumulation risk, or poor aesthetics is an issue for the patient (4). Most orthodontic treatment takes place around puberty (approximately from the age of 12 to 15 years) (19), in young adult dentition.
In France, the cost of orthodontic treatment is not fixed. National health insurance covers only a part of the cost, 20% on average (20, 21), and then only if treatment starts before the patient’s 16th birthday and for a maximum of 3 years. In addition to national health insurance coverage, most families have supplementary private health insurance policy that can reimburse all of the balance but most often covers only some of it. Families with extremely low income have supplementary government insurance, which is supposed to ensure total coverage of the cost of orthodontic treatment, which is fixed for these families at 928 euros per year. Otherwise, costs range approximately from 1000 to 3000 euros a year.
In France as elsewhere, there are social inequalities in oral health care (22, 23). Expenditures are closely related to socio-economic status: managers spend much more on oral health care than manual workers do (22). The particularity of the French system for oral health lies in the distinction between conservative care on the one hand and prosthetic and orthodontic care on the other. The national health insurance offers relatively good coverage for conservative care, which is low-priced whereas its coverage for the much more costly prosthetic and orthodontic care is poor (24). There remain social disparities in conservative care, despite the coverage by the national health insurance of 70% of its cost. Because orthodontic treatment is covered much less completely, we suppose that the social and economic inequalities are greater in orthodontic treatment than in conservative care.
In European and American studies, the prevalence of orthodontic treatment ranges from 10 to 35% and is lower in less privileged groups (2, 25–27). A study describing inequalities in orthodontic treatment in Northern Ireland where orthodontic treatment is free for teenagers showed that several factors were associated with orthodontic treatment including regular dentist visits and good oral hygiene, but did not find any relation between socio-economic factors and orthodontic treatment (28). An English study showed that discontinuation of orthodontic treatment was more frequent among children in less privileged social classes (29). In France, two studies estimated that 11% of schoolchildren aged in average 10–11 years and 27% of schoolchildren aged in average 14–15 years had orthodontic treatment (26, 27). In both studies, the treatment rate was twice as high among managers’ as among manual workers’ children. Economic issues do not appear to explain fully this disparity (22, 28). Education and culture may play a specific role (30, 31), as may accessibility of care. To our knowledge, the specific roles of all these dimensions on orthodontic treatment have not been explored.
The aim of this study was to estimate the prevalence of orthodontic treatment in France among children and teenagers aged 8 to 18 years, by sex and by age, and to investigate the specific role of social and economic characteristics on use of orthodontic treatment.
MATERIALS AND METHODS
Population
The study is based on data from the 2002–2003 Decennial Heath Survey conducted by INSEE (French National Institute of Statistics and Economics Studies), a cross-sectional study of a representative sample of the population living in France. It used unequal probability sampling of 25021 homes, randomly selected from a database of homes included in the 1999 census questionnaire and another database of new homes constructed after 1999. Each home was considered a household. The random selection of homes was stratified by region and by urban size. A sampling weight was associated with each person, based on the probability of his or her inclusion and on adjustments for non-responders (32). The sample was recruited during one year, in 5 waves, from October 2002 to October 2003.
Information was collected by interview. One reference adult from each household was interviewed about the household demographic, social and economic characteristics. Then all adults in the household (including the reference subject) were interviewed about their own demographic, social and economic characteristics and their health. A designated adult answered questions about the household members younger than 18 years.
Because the national health insurance covers part of the cost of orthodontic treatment if it starts before the subject’s 16th birthday and for a maximum of three years, we limited the study to subjects younger than 18. Because this treatment is very rare before the age of 8, we excluded children younger than 8 years (only 3 of whom had orthodontic treatment). Of 40796 individuals, 6175 were aged from 8 to 18 (figure 1). Among them, only children of either the household reference or of his/her partner were included in the study. This led to the exclusion of 140 subjects. Among these excluded subjects, 36 lived on their own, i.e. were themselves the household reference or his/her partner; they were therefore not included because they were not comparable to children living with their parents in their social characteristics. The health questionnaire was incomplete for 47 subjects. Thus, the study sample included 5988 subjects aged 8 to 18 living with their parents who completed the health questionnaire. We will refer to them as children.
Figure 1.
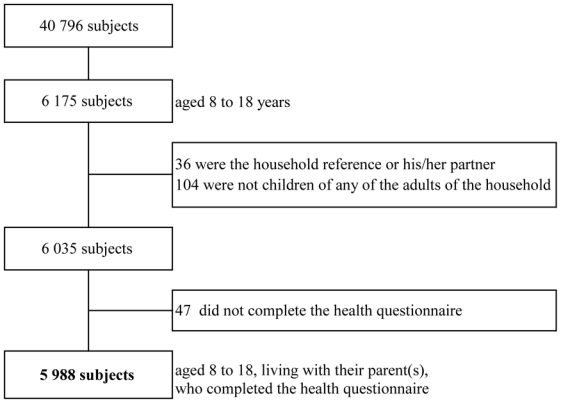
Participation chart
Data
Orthodontic treatment was assessed by the combination of two questions: “Does X have a dental appliance? Yes/No”, and if so “Orthodontic appliance? Yes/No”. From these two questions, we identified the children who were receiving orthodontic treatment. The demographic characteristics considered were the child’s sex and age, family structure (standard two-parent family; blended family; or single-parent family), and number of children in the household (that is, living in the household at the time of the survey). The social factors considered were the place of birth of mother or stepmother (France; other country in Europe; Africa; or other country in the world), her educational attainment (no or primary education; vocational qualification; general secondary education (middle or high school diploma); postsecondary certification (any university diploma)), family social status defined as the higher of the parents’ occupational group, based on current or most recent job if currently unemployed (professionals and managers; intermediate professionals; office workers, self-employed, farmers and shopkeepers; service and sales workers; or manual workers), annual household income (in quartiles), supplementary insurance covering the child (private; government; or none). When children lived with their father but not with their mother we considered the father’s partner, if there was one, to be the stepmother. Families were classified as living in urban or rural areas according to the INSEE definition (33). Finally, we considered the density of orthodontists in the district (administrative division) of residence. There are 95 districts in France. The density of orthodontists in the district was assessed by the number of orthodontists in 1999 divided by the number of children aged 10–15 years in 1999. We ranked in quintiles the 95 densities calculated, and then we used this classification in our study.
Statistical analysis
We chose to use weighted estimates in all analyses for consistency with the survey design (34). Thus, all analyses were weighted; all percentages, odds ratios and p-values were calculated; and the weights were taken into account at an individual level. The first step was the bivariate analysis of the prevalence of orthodontic treatment and the various individual and family characteristics.
Because boys and girls grow at different rates and orthodontic treatment varies according to age, sex and age were included in the multivariate analysis. Other covariates were selected if the p-value of Pearson χ2 for association with orthodontic treatment was less than or equal to 0.05. All variables except family structure were thus selected. Because the family’s social status, mother’s or stepmother’s educational attainment and family income were closely linked, only two of the three were kept in the model. Income was selected because it appeared to be a major trait associated with orthodontic treatment. It then appeared relevant to study the role of social status on the one hand and of maternal education on the other. Finally we used two separate models, one including family social status and the other including maternal educational attainment. Adjusting for the number of parents in the family seemed essential for studying the role of income. Family structure was therefore modified as a dichotomous variable: two “parents” (standard two-parent family and blended family) or one parent (single-parent family).
Because most orthodontic treatment occurs between the age of 12 and 15 years, we conducted a separate analysis for this age group only.
Children from the same family share the same family characteristics. To take into account the intra-family correlation, we applied a marginal model that used generalized estimating equations (GEE), with family as level 2.
Crude and adjusted odds ratios were calculated for each selected variable. The reference classes were either the most well-off or the largest groups.
SAS software (9.1 version) was used for the analyses.
RESULTS
Table 1 describes the characteristics of the study population; boys accounted for 51% of the study sample. Most children (74%) lived in standard two-parent families and were covered (86%) by private supplementary insurance; 17% lived in a rural area, 15% in a district with a low density of orthodontists and 25% in a district with a high density of orthodontists.
Table 1.
Prevalence of orthodontic treatment by social and economic characteristics
| n | wg %1 | OT2 | OT | p4 | |
|---|---|---|---|---|---|
| n | wg %3 | ||||
| Total | 5 988 | 100 | 837 | 14 | |
| Sex | |||||
| Boys | 3 089 | 51 | 394 | 13 | |
| Girls | 2 899 | 49 | 443 | 15 | 0.020 |
| Age group | |||||
| 8–11 years | 2 077 | 33 | 180 | 9 | |
| 12–15 years | 2 287 | 38 | 520 | 23 | |
| 16–18 years | 1 624 | 29 | 137 | 9 | <0.001 |
| Family structure | |||||
| Standard two-parent | 4 532 | 74 | 657 | 14 | |
| Blended | 465 | 8 | 52 | 13 | |
| Single-parent | 991 | 18 | 128 | 13 | 0.480 |
| Number of children | |||||
| 1 | 1 665 | 30 | 199 | 12 | |
| 2 | 2 599 | 42 | 431 | 16 | |
| 3 | 1 232 | 21 | 174 | 15 | |
| 4 and more | 492 | 7 | 33 | 7 | <0.001 |
| Place of birth of mother (or stepmother) | |||||
| France | 4 735 | 82 | 702 | 15 | |
| Other Europe | 248 | 4 | 38 | 15 | |
| Africa | 723 | 12 | 58 | 8 | |
| Other World | 118 | 2 | 21 | 16 | <0.001 |
| Maternal educational attainment | |||||
| No or primary education | 1 473 | 24 | 122 | 8 | |
| Vocational qualification | 1 565 | 28 | 210 | 13 | |
| General secondary education diploma | 1 417 | 24 | 212 | 15 | |
| Post secondary certification | 1 395 | 24 | 278 | 20 | <0.001 |
| Family social status | |||||
| Professionals, managers | 1 206 | 20 | 249 | 21 | |
| Intermediate professionals | 1 542 | 26 | 250 | 16 | |
| Office workers, self-employed, farmers, shopkeepers | 1 603 | 27 | 203 | 13 | |
| Service and sales workers | 713 | 12 | 65 | 9 | |
| Manual workers | 882 | 14 | 69 | 8 | <0.001 |
| Income (euros) | |||||
| < 18 000 | 1 422 | 25 | 134 | 10 | |
| 18 000 – 27 000 | 1 596 | 26 | 181 | 11 | |
| 27 000 – 39 000 | 1 465 | 25 | 209 | 14 | |
| > 39 000 | 1 505 | 25 | 313 | 21 | <0.001 |
| Supplementary insurance | |||||
| Private | 5 001 | 86 | 753 | 15 | |
| Government | 354 | 6 | 34 | 9 | |
| None | 534 | 9 | 32 | 6 | <0.001 |
| Residence area | |||||
| Urban | 5 082 | 83 | 737 | 15 | |
| Rural | 906 | 17 | 100 | 11 | 0.0018 |
| Density of orthodontists5 | |||||
| < 21.5 | 945 | 15 | 105 | 11 | |
| 21.5 – 26.8 | 963 | 18 | 127 | 13 | |
| 26.8 – 33.7 | 1 681 | 29 | 220 | 13 | |
| 33.7 – 53.3 | 902 | 13 | 126 | 14 | |
| > 53.3 | 1 497 | 25 | 259 | 17 | 0.0021 |
weighted percentage of each class within covariate
orthondontic treatment
weighted percentage of orthodontic treatment in each class
Pearson χ2 p-value
in the department for 100 000 inhabitants, aged 10 to 15 years
The prevalence of orthodontic treatment was 14% for all children aged 8 to 18 years, 23% for those 12 to 15, and 9% for the youngest and oldest age groups. Orthodontic treatment was slightly more frequent for girls (15%) than for boys (13%) (table 1).
The rate of orthodontic treatment was significantly lower when there were 4 children or more in the household, when the mother or the stepmother was born in Africa, when the parents were service or sales workers or manual workers, when the child had no supplementary insurance, or when the family lived in a rural area (table 1). The orthodontic treatment rate was higher when parents were professionals or managers, had a high income, or when the child lived in an area with a high density of orthodontists (table 1). The frequency of orthodontic treatment did not differ according to the family structure.
The first multivariate model included family social status but not maternal educational attainment (table 2). Children with a mother or a stepmother born in Africa were less likely to have orthodontic treatment (aOR=0.61; 95%CI: [0.44;0.85]) compared with children with mothers or stepmothers born in France. Family social status was associated with orthodontic treatment: compared with children whose parents were managers or professionals, children were less likely to have orthodontic treatment if their parents were service or sales workers (aOR=0.50; 95%CI: [0.34;0.76]), manual workers (aOR=0.56; 95%CI: [0.39;0.81]), or office workers, self-employed, farmers, or shopkeepers, (aOR=0.73; 95%CI: [0.56;0.96]). There was a gradient in the association between the annual income and orthodontic treatment. When the annual income of the family was low, children were less likely to have orthodontic treatment (aOR=0.62; 95%CI: [0.45;0.85]) than children of families with high income. Children without supplementary insurance were less likely to have orthodontic treatment (aOR=0.53; 95%CI: [0.34;0.81]) than children covered by private supplementary insurance. Children who lived in rural areas were less likely to have orthodontic treatment (aOR=0.70; 95%CI: [0.54;0.91]) than those who lived in urban areas. No significant association was found between orthodontic treatment and density of orthodontists (table 2).
Table 2.
Relations between orthodontic treatment and social characteristics (weighted multivariate logistic regression)
| cOR1 | 95%CI | aOR2 | 95%CI | p3 | aOR4 | 95%CI | p5 | |
|---|---|---|---|---|---|---|---|---|
| Sex | ||||||||
| Boys | ref | ref | ref | |||||
| Girls | 1.21 | [1.03–1.41] | 1.20 | [1.01–1.42] | 0.036 | 1.20 | [1.01–1.42] | 0.035 |
| Age group | ||||||||
| 8–11 years | 0.34 | [0.28–0.42] | 0.33 | [0.27–0.41] | 0.33 | [0.27–0.41] | ||
| 12–15 years | ref | ref | ref | |||||
| 16–18 years | 0.32 | [0.26–0.40] | 0.33 | [0.26–0.41] | <0.001 | 0.33 | [0.27–0.42] | <0.001 |
| Family structure | ||||||||
| Two-parent | ref | ref | ref | |||||
| One-parent | 0.89 | [0.72–1.11] | 1.21 | [0.92–1.60] | 0.177 | 1.18 | [0.90–1.56] | 0.235 |
| Number of children | ||||||||
| 1 | 0.70 | [0.57–0.85] | 0.78 | [0.63–0.96] | 0.79 | [0.64–0.98] | ||
| 2 | ref | ref | ref | |||||
| 3 | 0.87 | [0.71–1.07] | 0.93 | [0.75–1.17] | 0.94 | [0.76–1.72] | ||
| 4 and more | 0.41 | [0.28–0.61] | 0.55 | [0.36–0.86] | 0.009 | 0.56 | [0.36–0.86] | 0.014 |
| Place of birth of mother (or stepmother) | ||||||||
| France | ref | ref | ref | |||||
| Other Europe | 1.04 | [0.71–1.52] | 1.03 | [0.70–1.52] | 1.05 | [0.71–1.56] | ||
| Africa | 0.46 | [0.34–0.62] | 0.61 | [0.44–0.85] | 0.63 | [0.45–0.88] | ||
| Other World | 1.09 | [0.66–1.78] | 1.24 | [0.71–2.16] | 0.024 | 1.25 | [0.71–2.19] | 0.032 |
| Maternal educational attainment | ||||||||
| No or primary education | 0.36 | [0.28–0.46] | 0.59 | [0.43–0.81] | ||||
| Vocational qualification | 0.61 | [0.49–0.75] | 0.77 | [0.60–0.98] | ||||
| General secondary education dilpoma | 0.72 | [0.58–0.88] | 0.85 | [0.68–1.08] | ||||
| Post secondary certification | ref | ref | 0.009 | |||||
| Family social status | ||||||||
| Professionals, managers | ref | ref | ||||||
| Intermediate professionals | 0.75 | [0.61–0.92] | 0.89 | [0.70–1.13] | ||||
| Office workers, self-employed, farmers, shopkeepers | 0.55 | [0.44–0.69] | 0.73 | [0.56–0.96] | ||||
| Service and sales workers | 0.39 | [0.28–0.54] | 0.50 | [0.34–0.76] | ||||
| Manual workers | 0.34 | [0.25–0.46] | 0.56 | [0.39–0.81] | 0.002 | |||
| Income (euros) | ||||||||
| < 18 000 | 0.42 | [0.33–0.53] | 0.62 | [0.45–0.85] | 0.56 | [0.41–0.76] | ||
| 18 000 – 27 000 | 0.48 | [0.39–0.59] | 0.64 | [0.49–0.83] | 0.60 | [0.47–0.77] | ||
| 27 000 – 39 000 | 0.63 | [0.51–0.78] | 0.76 | [0.60–0.96] | 0.003 | 0.74 | [0.59–0.94] | |
| > 39 000 | ref | ref | ref | <0.001 | ||||
| Supplementary insurance | ||||||||
| Private | ref | ref | ref | |||||
| Government | 0.59 | [0.40–0.87] | 0.89 | [0.53–1.48] | 0.97 | [0.61–1.53] | ||
| None | 0.35 | [0.24–0.52] | 0.53 | [0.34–0.81] | 0.013 | 0.53 | [0.35–0.81] | 0.013 |
| Residence area | ||||||||
| Urban | ref | ref | ref | |||||
| Rural | 0.68 | [0.54–0.87] | 0.70 | [0.54–0.91] | 0.008 | 0.68 | [0.53–0.89] | 0.004 |
| Density of orthodontists6 | ||||||||
| < 21.5 | 0.60 | [0.46–0.79] | 0.76 | [0.57–1.01] | 0.83 | [0.61–1.14] | ||
| 21.5 – 26.8 | 0.75 | [0.59–0.96] | 0.79 | [0.61–1.02] | 0.79 | [0.58–1.07] | ||
| 26.8 – 33.7 | 0.75 | [0.60–0.92] | 0.82 | [0.65–1.03] | 0.84 | [0.66–1.05] | ||
| 33.7 – 53.3 | 0.75 | [0.58–0.97] | 0.80 | [0.61–1.06] | 0.80 | [0.63–1.01] | ||
| > 53.3 | ref | ref | 0.211 | ref | 0.302 | |||
crude odds-ratio and 95% confidence interval
adjusted odds-ratio for all variables in the table except maternal educational attainment and 95% confidence interval
adjusted Wald χ2 p-value for all variables in the table except maternal educational attainment
adjusted odds-ratio for all variables in the table except family social status and 95% confidence interval
adjusted Wald χ2 p-value for all variables in the table except family social status
in the department for 100 000 inhabitants, aged 10 to 15 years
The second multivariate model included maternal educational attainment but not family social status (table 2). The aORs showed a gradient in the relation between educational attainment (from no or primary education to university) and orthodontic treatment. Children whose mother had the least education were less likely to have orthodontic treatment (aOR=0.59; 95%CI: [0.43;0.81]) compared with children whose mother or stepmother obtained a university diploma. The other aORs were very similar to those described in table 2.
We conducted a sensitivity analysis to verify that our results for the entire sample were consistent with those for the children aged 12 to 15 years, which is the common age for orthodontic treatment. It showed pretty much the same associations as for the sample as a whole, but the aORs were closer to 1, and the confidence intervals were larger (results not shown). The results of the GEE taking into account the intra-family correlation are very close to those of the multivariate regression analysis and thus indicate that the non-independence of the data of children from the same family does not affect the results (not shown).
The multivariate analysis excluded 283 children because of missing information on the place of birth of mother or stepmother (138 lived with their father and no mother or stepmother), family social status, or supplementary insurance. Twelve percent of these excluded children had orthodontic treatment.
DISCUSSION
This study of a large national sample of the population living in France explored the relations between social and economic characteristics and orthodontic treatment. The prevalence of orthodontic treatment was 14% for children aged 8 to 18 years and 23% for those aged 12–15. Orthodontic treatment was mainly associated with family social status, maternal educational level, family income and supplementary health insurance. Orthodontic treatment was also associated with sex, number of children in the household, the place of birth of mother or stepmother, and the residence area.
As it was a cross-sectional survey, we have a snapshot of orthodontic treatment at the time of the survey. So we may assume that the prevalence of orthodontic treatment was correctly estimated.
The 47 children with incomplete questionnaires on health were excluded. Only 5% (283) of the children were excluded from the multivariate analysis for missing data on covariates. These exclusions are thus unlikely to have modified the estimated associations.
The observed prevalence of orthodontic treatment, 23% among children aged 12 to 15 years, and 9% among those aged 8 to 11, is not very different to the prevalence observed in other French studies in 2004 (26, 27), considering that the age groups are not similar. These findings are also consistent with those of the international literature. In Europe, 28% of teenagers in Northern Ireland (15–16 years old) had or were about to have orthodontic treatment (28). In the NHANES III study of a representative sample of the US population conducted between 1988 and 1991, 30% of white Americans aged 12 to 17 years had orthodontic treatment.
As in other international and French studies, we found that the prevalence of orthodontic treatment was slightly higher among girls than boys (25, 26, 28, 35). Nonetheless, the literature does not show any sex difference in the need for orthodontic treatment (25, 36–39). Requests for aesthetic reasons are probably higher among girls, and parents might be more attentive to the appearance of their daughters than to their sons. Girls may also be more concerned about their oral health than boys, and may go more easily and regularly to the dentist. They would be thus more likely to accept orthodontic treatment. That was suggested in one study of American adults (40).
Orthodontic treatment was associated with maternal level of education, family social status, income and supplementary insurance. In other words, in equal income groups, and with equal supplementary coverage, family social status or maternal education still influenced orthodontic treatment. This treatment costs approximately € 1000 to € 3000 a year. Our data provide no information about the amount covered by private insurance, but it can vary from € 100 to € 1000 a year, according to the policy. The group of children with private insurance is therefore probably heterogeneous, mixing children with excellent coverage and those with basic insurance. The association between orthodontic treatment and income is therefore not surprising but it is interesting to estimate it, especially when taking into account supplementary insurance and social status. Social status is clearly linked to income (as well as maternal education) but the persistence of the association after adjustment for income probably reflects the influence of the social environment and maternal education on orthodontic treatment.
As every country has its own health care system (41), comparisons between countries are difficult. Nevertheless, social differences in orthodontic treatment have been observed in the United States, where both treatment and insurance are expensive (2, 42), and in France (26, 27), but also in England, where treatment is free for teenagers (25, 29, 43, 44).
Children whose mother or stepmother was born in Africa had orthodontic treatment at a lower rate than those whose mother or stepmother was born in France. This is consistent with a German study that reported that immigrant status of either parent or child was associated with a lower prevalence of orthodontic treatment in a population with low socio-economic status (30). Women born in Africa may have been less exposed to orthodontic treatment than their French counterparts and thus may be less aware of its potential benefits.
Orthodontic treatment was less frequent in rural areas, possibly because longer distances to reach an orthodontist may be an obstacle to orthodontic treatment, which requires regular visits. However, there was no significant association between orthodontic treatment and density of orthodontists, although such a link has been observed in England (31). In our study, density of orthodontists was calculated as a mean density in the district of residence, but districts are large administrative divisions and density may therefore vary substantially within the district.
This study dealt with orthodontic treatment but we had no information about either the type of malocclusion or the need for treatment. Orthodontic treatment needs seem to vary between populations, for instance they have been estimated at around 21% in a population aged 9 to 12 in France (37), and 35% among 12 year-olds in England (25). Both European and American studies found that immigrant background (30, 45), lower income (2), and lower socio-economic group (31, 46) are associated with higher orthodontic treatment need. The same factors thus appear to be associated with both a higher rate of orthodontic treatment need and a lower rate of orthodontic treatment, and the actual social inequalities are probably even greater than that we observed.
Several mechanisms may explain these social differences: fewer spontaneous requests for orthodontic treatment from less privileged families, fewer dental visits, thus fewer occasions for need assessment, and when need is identified, either a more restrictive attitude by dentists to recommending treatment for patients from low income families because of its cost or more refusals from these families for the same reason. Exploring the respective role of each of these mechanisms could help trying to bring needs and treatment closer together.
CONCLUSION
This study revealed social inequalities in orthodontic treatment in France. Our findings point to the importance of assessing orthodontic treatment needs and of improving access to orthodontic treatment; to reach the goal of equal opportunity for oral health.
Acknowledgments
This study was founded by DREES/MiRe (Ministry of Health). We thank Jean-Louis Lanoë, Laurence Watier and Laetitia Marchand for their cooperation.
References
- 1.Lathrop ST. The American Heritage Stedman’s Medical Dictionary: Houghton Mifflin. 2005. [Google Scholar]
- 2.Proffit WR, Fields HW, Jr, Moray LJ. Prevalence of malocclusion and orthodontic treatment need in the United States: estimates from the NHANES III survey. Int J Adult Orthodon Orthognath Surg. 1998;13:97–106. [PubMed] [Google Scholar]
- 3.Proffit WR. Contemporary orthodontics. 4. St. Louis: Mosby Elsevier; 2007. [Google Scholar]
- 4.ANAES. Recommandations. 2002. Indications de l’orthopédie dento-faciale et dento-maxillo-faciale. [Google Scholar]
- 5.Shaw WC, Addy M, Ray C. Dental and social effects of malocclusion and effectivenessof orthodontic treatment: a review. Community Dent Oral Epidemiol. 1980 Feb;8(1):36–45. doi: 10.1111/j.1600-0528.1980.tb01252.x. [DOI] [PubMed] [Google Scholar]
- 6.Helm S, Petersen PE. Causal relation between malocclusion and caries. Acta Odontol Scand. 1989 Aug;47(4):217–21. doi: 10.3109/00016358909007704. [DOI] [PubMed] [Google Scholar]
- 7.Geiger AM. Malocclusion as an etiologic factor in periodontal disease: a retrospective essay. Am J Orthod Dentofacial Orthop. 2001 Aug;120(2):112–5. doi: 10.1067/mod.2001.114537. [DOI] [PubMed] [Google Scholar]
- 8.Bollen AM. Effects of malocclusions and orthodontics on periodontal health: evidence from a systematic review. J Dent Educ. 2008 Aug;72(8):912–8. [PubMed] [Google Scholar]
- 9.Ngom PI, Diagne F, Benoist HM, Thiam F. Intraarch and interarch relationships of the anterior teeth and periodontal conditions. Angle Orthod. 2006 Mar;76(2):236–42. doi: 10.1043/0003-3219(2006)076[0236:IAIROT]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 10.van Gastel J, Quirynen M, Teughels W, Carels C. The relationships between malocclusion, fixed orthodontic appliances and periodontal disease. A review of the literature. Aust Orthod J. 2007 Nov;23(2):121–9. [PubMed] [Google Scholar]
- 11.Helm S, Petersen PE. Causal relation between malocclusion and periodontal health. Acta Odontol Scand. 1989 Aug;47(4):223–8. doi: 10.3109/00016358909007705. [DOI] [PubMed] [Google Scholar]
- 12.Bollen AM, Cunha-Cruz J, Bakko DW, Huang GJ, Hujoel PP. The effects of orthodontic therapy on periodontal health: a systematic review of controlled evidence. J Am Dent Assoc. 2008 Apr;139(4):413–22. doi: 10.14219/jada.archive.2008.0184. [DOI] [PubMed] [Google Scholar]
- 13.Shaw WC, Addy M, Dummer PM, Ray C, Frude N. Dental and social effects of malocclusion and effectiveness of orthodontic treatment: a strategy for investigation. Community Dent Oral Epidemiol. 1986 Feb;14(1):60–4. doi: 10.1111/j.1600-0528.1986.tb01497.x. [DOI] [PubMed] [Google Scholar]
- 14.Shaw WC, Richmond S, Kenealy PM, Kingdon A, Worthington H. A 20-year cohort study of health gain from orthodontic treatment: psychological outcome. Am J Orthod Dentofacial Orthop. 2007 Aug;132(2):146–57. doi: 10.1016/j.ajodo.2007.04.009. [DOI] [PubMed] [Google Scholar]
- 15.Macfarlane TV, Kenealy P, Kingdon HA, Mohlin BO, Pilley JR, Richmond S, et al. Twenty-year cohort study of health gain from orthodontic treatment: temporomandibular disorders. Am J Orthod Dentofacial Orthop. 2009 Jun;135(6):692 e1–8. doi: 10.1016/j.ajodo.2008.10.017. discussion -3. [DOI] [PubMed] [Google Scholar]
- 16.Bastone EB, Freer TJ, McNamara JR. Epidemiology of dental trauma: a review of the literature. Aust Dent J. 2000 Mar;45(1):2–9. doi: 10.1111/j.1834-7819.2000.tb00234.x. [DOI] [PubMed] [Google Scholar]
- 17.Malandris M, Mahoney EK. Aetiology, diagnosis and treatment of posterior cross-bites in the primary dentition. Int J Paediatr Dent. 2004 May;14(3):155–66. doi: 10.1111/j.1365-263X.2004.00546.x. [DOI] [PubMed] [Google Scholar]
- 18.Helm S, Kreiborg S, Solow B. Malocclusion at adolescence related to self-reported tooth loss and functional disorders in adulthood. Am J Orthod. 1984 May;85(5):393–400. doi: 10.1016/0002-9416(84)90160-x. [DOI] [PubMed] [Google Scholar]
- 19.Guay AH, Brown LJ, Wall T. Orthodontic dental patients and expenditures--2004. Am J Orthod Dentofacial Orthop. 2008 Sep;134(3):337–43. doi: 10.1016/j.ajodo.2008.01.012. [DOI] [PubMed] [Google Scholar]
- 20.Arrêté du 30 mai 2006. Journal officiel de la République française; 2006.
- 21.Dentalespace. L’orthodontie chez l’enfant et l’adulte. 2005. [cited; Available from: http://www.dentalespace.com/patient/soins-dentaires/21-orthodontie-chez-enfant-adulte.htm.
- 22.Leclerc A, Kaminski M, Lang T. Inégaux face à la santé. Paris: La Découverte/Inserm; 2008. [Google Scholar]
- 23.Dargent-Paré C, Bourgeois D. La santé bucco-dentaire. Les inégalités sociales de santé. Paris: La Découverte/Inserm; 2000. pp. 267–82. [Google Scholar]
- 24.Azogui-Lévy S. Bulletin d’information en économie de la santé n°94 IRDES. 2005. Comportements de recours aux soins et santé bucco-dentaire. [Google Scholar]
- 25.Chestnutt IG, Burden DJ, Steele JG, Pitts NB, Nuttall NM, Morris AJ. The orthodontic condition of children in the United Kingdom, 2003. Br Dent J. 2006 Jun 10;200:609–12. doi: 10.1038/sj.bdj.4813640. [DOI] [PubMed] [Google Scholar]
- 26.Guignon N. Etudes et résultats. DREES; 2007. La santé des adolescents scolarisés en classe de 3ème en 2003–2004. [Google Scholar]
- 27.Guignon N. Etudes et résultats. DREES; 2008. La santé des enfants scolarisés en CM2 en 2004–2005. [Google Scholar]
- 28.Breistein B, Burden DJ. Equity and orthodontic treatment: a study among adolescents in Northern Ireland. Am J Orthod Dentofacial Orthop. 1998 Apr;113(4):408–13. doi: 10.1016/s0889-5406(98)80012-7. [DOI] [PubMed] [Google Scholar]
- 29.Turbill EA, Richmond S, Wright JL. Social inequality and discontinuation of orthodontic treatment: is there a link? Eur J Orthod. 2003 Apr;25(2):175–83. doi: 10.1093/ejo/25.2.175. [DOI] [PubMed] [Google Scholar]
- 30.Bissar AR, Oikonomou C, Koch MJ, Schulte AG. Dental health, received care, and treatment needs in 11- to 13-year-old children with immigrant background in Heidelberg, Germany. Int J Paediatr Dent. 2007 Sep;17(5):364–70. doi: 10.1111/j.1365-263X.2007.00846.x. [DOI] [PubMed] [Google Scholar]
- 31.Morris E, Landes D. The equity of access to orthodontic dental care for children in the North East of England. Public Health. 2006 Apr;120(4):359–63. doi: 10.1016/j.puhe.2005.10.017. [DOI] [PubMed] [Google Scholar]
- 32.Wilms . Fiche récapitulative du plan de sondage de l’enquête santé. Paris: Institut national de la statistique et des études économiques;; 2002. Report No.: 048. [Google Scholar]
- 33.Bessy-Pietri Sicamois. Le zonage en aires urbaines en 1999. Paris: Insee première;; 2001. [Google Scholar]
- 34.Skinner C. Analysis of complex survey data. CREST course; 2006. Paris: Mar, 2006. [Google Scholar]
- 35.Jonsson T, Arnlaugsson S, Karlsson KO, Ragnarsson B, Arnarson EO, Magnusson TE. Orthodontic treatment experience and prevalence of malocclusion traits in an Icelandic adult population. Am J Orthod Dentofacial Orthop. 2007 Jan;131(1):8 e11–8. doi: 10.1016/j.ajodo.2006.05.030. [DOI] [PubMed] [Google Scholar]
- 36.Thilander B, Pena L, Infante C, Parada SS, de Mayorga C. Prevalence of malocclusion and orthodontic treatment need in children and adolescents in Bogota, Colombia. An epidemiological study related to different stages of dental development. Eur J Orthod. 2001 Apr;23(2):153–67. doi: 10.1093/ejo/23.2.153. [DOI] [PubMed] [Google Scholar]
- 37.Souames M, Bassigny F, Zenati N, Riordan PJ, Boy-Lefevre ML. Orthodontic treatment need in French schoolchildren: an epidemiological study using the Index of Orthodontic Treatment Need. Eur J Orthod. 2006 Dec;28(6):605–9. doi: 10.1093/ejo/cjl045. [DOI] [PubMed] [Google Scholar]
- 38.Evensen JP, Ogaard B. Are malocclusions more prevalent and severe now? A comparative study of medieval skulls from Norway. Am J Orthod Dentofacial Orthop. 2007 Jun;131(6):710–6. doi: 10.1016/j.ajodo.2005.08.037. [DOI] [PubMed] [Google Scholar]
- 39.Liepa A, Urtane I, Richmond S, Dunstan F. Orthodontic treatment need in Latvia. Eur J Orthod. 2003 Jun;25(3):279–84. doi: 10.1093/ejo/25.3.279. [DOI] [PubMed] [Google Scholar]
- 40.Whitesides J, Pajewski NM, Bradley TG, Iacopino AM, Okunseri C. Socio-demographics of adult orthodontic visits in the United States. Am J Orthod Dentofacial Orthop. 2008 Apr;133(4):489 e9–14. doi: 10.1016/j.ajodo.2007.08.016. [DOI] [PubMed] [Google Scholar]
- 41.Majnoni d’Intignano B. Economie de la santé. Paris: Presse Universitaire de France; 2001. [Google Scholar]
- 42.Reichmuth M, Greene KA, Orsini MG, Cisneros GJ, King GJ, Kiyak HA. Occlusal perceptions of children seeking orthodontic treatment: impact of ethnicity and socioeconomic status. Am J Orthod Dentofacial Orthop. 2005 Nov;128(5):575–82. doi: 10.1016/j.ajodo.2004.09.021. [DOI] [PubMed] [Google Scholar]
- 43.Turbill EA, Richmond S, Wright JL. A closer look at General Dental Service orthodontics in England and Wales. I: Factors influencing effectiveness. Br Dent J. 1999 Aug 28;187(4):211–6. doi: 10.1038/sj.bdj.4800242. [DOI] [PubMed] [Google Scholar]
- 44.Kenealy P, Frude N, Shaw W. The effects of social class on the uptake of orthodontic treatment. Br J Orthod. 1989 May;16(2):107–11. doi: 10.1179/bjo.16.2.107. [DOI] [PubMed] [Google Scholar]
- 45.Josefsson E, Bjerklin K, Lindsten R. Malocclusion frequency in Swedish and immigrant adolescents--influence of origin on orthodontic treatment need. Eur J Orthod. 2007 Feb;29(1):79–87. doi: 10.1093/ejo/cjl054. [DOI] [PubMed] [Google Scholar]
- 46.Tickle M, Kay EJ, Bearn D. Socio-economic status and orthodontic treatment need. Community Dent Oral Epidemiol. 1999 Dec;27(6):413–8. doi: 10.1111/j.1600-0528.1999.tb02040.x. [DOI] [PubMed] [Google Scholar]