

Abstract
Syringe exchange programs (SEPs) can reduce HIV risk among injecting drug users (IDUs) but their use may depend heavily on contextual factors such as local syringe policies. The frequency and predictors of transitioning over time to and from direct, indirect, and non-use of SEPs are unknown. We sought, over one year, to: (1) quantify and characterize transition probabilities of SEP attendance typologies; (2) identify factors associated with (a) change in typology, and (b) becoming and maintaining direct SEP use; and (3) quantify and characterize transition probabilities of SEP attendance before and after changes in policy designed to increase access. Using data collected from 583 IDUs participating in a three-city cohort study of SEPs, we conducted a latent transition analysis and multinomial regressions. Three typologies were detected: Direct SEP users, Indirect SEP users and Isolated IDUs. Transitions to direct SEP use were most prevalent. Factors associated with becoming or maintaining direct SEP use were female sex, Latino ethnicity, fewer injections per syringe, homelessness, recruitment city, injecting speedballs (cocaine and heroin), and police contact involving drug paraphernalia possession. Similar factors influenced transitions in the syringe policy change analysis. Policy change cities experienced an increase in Indirect SEP users (43% to 51%) with little increased direct use (29% to 31%). We found that, over time, IDUs tended to become Direct SEP users. Policies improving syringe availability influenced SEP use by increasing secondary syringe exchange. Interactions with police around drug paraphernalia may encourage SEP use for some IDUs and may provide opportunities for other health interventions.
Keywords: syringe exchange, injecting drug use, HIV/AIDS, longitudinal study, latent transition analysis
1. INTRODUCTION
The injection of drugs is one of the main risk factors for HIV infection in the United States. Through 2007, more than one-quarter of AIDS cases in the country have occurred in individuals whose greatest risk for HIV infection is injection drug use. (Centers for Disease Control and Prevention, 2009) The sharing of injection equipment has consistently been linked to HIV transmission. (Chaisson et al., 1987; Marmor et al., 1987; Schoenbaum et al., 1989) Syringe exchange programs (SEPs) were one of the first strategies implemented to slow the spread of HIV infection among injection drug users (IDUs). (Singer et al., 1991) Such programs directly decrease the transmission of HIV by providing clean injection equipment and can indirectly benefit IDUs by providing prevention information, condoms, infectious disease screening, and referral to medical care or drug treatment for those attending the programs. (Bastos and Strathdee, 2000; Heinzerling et al., 2007; Strathdee et al., 1999) SEPs have remained controversial in the United States despite strong evidence that they have been successful in slowing the spread of HIV infection among participating IDUs. (Bastos and Strathdee, 2000; Des Jarlais et al., 1996; Heimer et al., 2002b; Huo et al., 2005)
Early studies characterized SEP participation as a dichotomous variable that, by definition, excluded non-participants from deriving benefit, thereby missing any salutary effects of SEP program participants who might exchange for others or otherwise redistribute sterile syringes or other prevention supplies and information obtained from a SEP, i.e., “indirect” or “secondary” exchange. However, while ecological studies suggested that IDUs in areas with SEPs may benefit from them even if they do not use them directly, few studies have specifically examined the impact of secondary exchange on IDUs. Existing studies have been equivocal with some showing benefits (Huo et al., 2005; Sears et al., 2001) to indirect SEP users and others indicating no impact (Valente et al., 1998) or increased risk. (Bryant and Hopwood, 2009; De et al., 2008; Lorvick et al., 2006; Sears et al., 2001) Understanding the role of secondary exchange on HIV injection-related risk has been hampered by inconsistencies in definitions of secondary exchange and the lack of a non-SEP user comparison. (Bastos and Strathdee, 2000; Bryant and Hopwood, 2009; Huo et al., 2005; Valente et al., 1998) No studies have reported the longitudinal effects of varying SEP contact at the individual level, or of the extension of SEP benefit beyond the program participant when the level of SEP exposure itself is time-varying.
From 1998 to 2001, the Diffusion of Benefit through Syringe Exchange (DOB) Study was conducted to determine if SEP benefits –including clean syringes, condoms, prevention interventions and health educational materials--diffuse beyond direct participants to other drug users in the community, such as those who arrange to have someone else use the SEP for them (indirect exchangers). (Bluthenthal et al., 2004) The DOB study involved annual assessments of IDUs specifically recruited in Hartford, CT, Oakland, CA, and Chicago, IL, to represent varying SEP types. By comparing data from SEPs that had different syringe dispensing policies, offered different levels of service, and operated in different social contexts (Table 1), it was possible to explore whether programmatic or other policy-level factors create limitations on diffusion of SEP benefit. (Bluthenthal et al., 2004)
Table 1.
Characteristics of SEPs at the time of the Diffusion of Benefit (DOB) Study (1998–2001)
| HARTFORD | OAKLAND | CHICAGO | |
|---|---|---|---|
| Exchange volume (syringes distributed per IDU per visit, pre-policy change) | Small, avg. <5 syringes exchanged/participant | Large, >100 syringes exchanged/participant | Large, >100 syringes exchanged/participant |
| Limits/nature | Cap of 10/1-for-1; cap increased to 30 on 9/1/1999 | No cap; 1-for-1 plus 5; 7 syringe starter pack | No cap; 2-for-1 to 10; 1-for-1 thereafter. 6/1/2000 then 1: ‘as needed’ |
| Legal status/organizational type | Legal; non-governmental organization run | Legal; non-governmental organization run | Exempt; non-governmental organization run |
| Estimated HIV prevalence in IDUs | 38%* | 18%† | 33%‡ |
| Pharmacy access to syringes | YES, cap of 10 until 9/1/1999 then cap of 30 | NO | NO |
| Drug paraphernalia law+ | NO | YES | YES; SEP users exempt |
Singer M and Weeks MR. Hartford Targeted Sampling Plan. Hartford. CT: Community Alliance for AIDS Programs, 1992.
Bluthenthal RN and Watters JK. “Multimethod research: from targeted sampling to HIV risk behaviors”, in Qualitative Methods in the Prevention of Drug Abuse, E. Y. Lambert, R.S. Ashery, and R.H. Needle, eds. National Institute on Drug Abuse: Rockville, MD. Pp. 212–230; 1995.
Personal communication, with Dan Bigg, executive director of the Chicago Recovery Alliance (CRA)
A drug paraphernalia law is one that restricts the possession or provision of injecting equipment
In a unique natural experiment, during the study syringe policies at two of the three study sites, Hartford and Chicago, underwent a change. Specifically, in Hartford, where a strict one-for-one policy of syringe exchange was in place, the maximum number of syringes obtainable per visit was increased from 10 syringes to 30 syringes. (Heimer et al., 2002b) In Chicago, the syringe dispensing policy changed in the summer of 2000 from a syringe exchange (two-for-one with a cap of ten syringes and one-for-one exchange for >10 syringes) to a need-based syringe distribution (i.e., receiving as many syringes ‘as needed’). Details of the three DOB study sites and their varying legal and service provision characteristics are given in Table 1. In previous cross-sectional studies differences in syringe dispensing policies have been associated with differences in syringe re-use, syringe coverage, and syringe sharing among IDUs as well as influencing SEP attendance patterns. (Bluthenthal et al., 2007a; Bluthenthal et al., 2007b; Heimer, 2008; Heimer et al., 2002b; Kral et al., 2004) What is not known is whether these differences influence the probability of an IDU becoming a Direct SEP user nor do we know what other factors might influence transitions into direct SEP use.
In this report, we aim to (1) quantify and characterize the transition probabilities of syringe exchange attendance typologies over a one-year period among IDUs involved in a multi-city longitudinal cohort study; (2) identify factors associated with (a) change in SEP user status in one year’s time and (b) transition to Direct SEP use and maintenance of Direct SEP use over one year; and (3) quantify and characterize the transition probabilities of SEP attendance typologies before compared to after a change in syringe access policy.
2. METHODS
2.1 Data source
Data derived from participants who reported injecting drugs within the previous 30 days and who consented to DOB study participation. All study procedures, instruments, and consent materials were approved by the human subject protection committees of the four institutions participating in this multi-site cohort study. The DOB Study employed snowball sampling techniques to recruit active IDUs and members of their injection drug using networks. By design, recruitment of IDUs who directly attended SEPs was capped at 25% of the sample to promote the potential for greater penetration into the larger non-SEP-using IDU community. A second sample of street outreach-recruited IDUs who did not directly access SEPs themselves was also recruited. Details of the study have been previously reported. (Grau et al., 2005; Heimer et al., 2002a) Follow-up procedures standard for maintaining contact with drug using populations were employed and included obtaining multiple collateral contacts, use of monetary incentives for completion of the follow-up assessments, and outreach to the SEPs to locate participants. Follow-up rates were 51% for all sites at the first follow-up visit and 45% for the second follow-up visit. Analyses revealed that missing data were associated with not having been stopped by police in the past year for drug paraphernalia (35.6% missing data vs. 64.4% not missing data, χ2=7.48, p<0.01), female sex (66.1% missing vs. 33.9% not missing, χ2=49.8, p<0.0001), and city of recruitment (Oakland vs. Chicago; 64.2% missing vs. 35.8% not, χ2=17.95, p<0.0001). All of these variables were included in the LTA models to control for data missing at random. No other sociodemographics or covariates were associated with missingness and none of the LTA indicators were associated with differential missingness. For the policy change analysis, 8.3% of cases had missing data and missingness was associated with city of recruitment (Hartford vs. Chicago-reference) and homelessness (both p<0.01). Both of these variables were included in the LTA as covariates to control for data missing at random.
For the purposes of addressing research aims 1 and 2, we limited the time points of interest in the longitudinal DOB Study to baseline and the one-year follow-up, which permitted use of data from 583 participants from all three study sites. To examine how the policy change impacted the SEP attendance membership groups (research aim 3), we conducted an analysis on assessments collected at the time prior to the policy change and those collected after the policy change. We constructed the LTA Time 1 and Time 2 from the DOB assessments, according to the city and the date of the policy change. Time 1 could therefore represent a baseline or follow-up 1 value (pre-policy change) while Time 2 could be a follow-up 1 or follow-up 2 value (i.e., the assessment conducted after the policy change). Dates of the policy change are noted in the Table 1. The Oakland SEP did not experience a policy change during the study period. Thus Oakland participant data were not included in the policy analysis (i.e., analysis n=228).
2.2 Analysis
Based on their self-reported use and involvement with SEPs and intensive, baseline-only network interview data, our previous work reported post-hoc categorization of participants into four groups: (1) direct syringe exchange users, (2) secondary exchange users (i.e., receives syringes and materials from someone who attends a syringe exchange), (3) knows a direct syringe exchange user but does not receive any SEP syringes or materials from them, and (4) does not know a syringe exchange attendee and does not receive SEP syringes or materials. (Grau et al., 2005)
For the set of research questions in this analysis, we were interested in exploring how typologies of SEP use change over time. A novel, latent variable approach to categorization of typologies of SEP use might offer additional insight into the operation of this key HIV and public health intervention, its utilization, and the change in its client population over time and in response to alterations in syringe policy. Therefore, we applied latent transition analysis (LTA) with covariates. This approach allows latent variable modeling techniques to empirically categorize and identify meaningful typologies of SEP use rather than the use of a priori definitions of expected typologies. Covariates could then be added directly to the LTA to test what variables influence the categories and the transitions between the categories over time. To accomplish the LTA, three dichotomous (yes/no) indicators of typologies of SEP use were included: (1) having used an SEP in the past 12 months; (2) knowing someone who has used an SEP in the past 12 months; and (3) having received syringes and/or materials from someone who exchanges injection materials at an SEP.
Using Proc LTA (Lanza and Collins, 2008) in SAS version 9.1 and Mplus software version 5.2 (Muthen and Muthen, 2007), we first performed exploratory latent class analyses on the baseline data, to determine the range of the number of latent classes that would fit the data. Then, competing LTA models of latent class sizes 2 to 4 were constructed for the baseline and follow-up. The absolute fit of the models was checked using the G2 (deviance) statistic< degrees of freedom. Relative fit of model groups (class sizes 2–4) was assessed by comparing both the Bayesian Information Criteria (BIC) and Akaike’s Information Criteria (AIC). Measurement invariance across time was tested in the final models by comparing differences in the G2 statistic for measurement variant and invariant models to the relevant χ2 values for the degrees of freedom of difference. LTA assumes data are missing at random, an assumption that was checked and fulfilled in a prior analysis. (Green et al., 2006) Next, we explored how the pre-specified covariates might influence the class membership at Time 1 and the probability of transitioning between classes from Time 1 to Time 2. Covariates of interest derived from Time 1 and included age, duration of injecting, sex, ethnicity (African American, Latino, or White/other), city, income, past month injection of cocaine, past month injection of speedball, smoked crack in the past month, homelessness status, number of shots used per syringe (log-transformed), educational status (≤high school versus > high school), self-reported hepatitis (i.e., hepatitis B or C virus infected) and HIV status, having experienced an overdose in the past year, self-rated health status, frequent healthcare use in the past year (dichotomized as <5 versus ≥5 visits, based on the distribution of responses), and having been stopped, detained, or arrested by the police in the past year for possession of drug paraphernalia (i.e., syringes or injecting equipment). The LTA analysis examining policy change employed an identical analytic approach except that covariates that could change over time were linked to the assessment from which the indicators derived. In this way, the policy model could explore baseline covariates as well as variables influencing the transition probabilities between the SEP groups over time.
Finally, to determine what factors might predict becoming a Direct SEP user and maintaining SEP user status at Time 2, we conducted a multinomial logistic regression analysis (PROC GLOGIST in SAS v.9.1) with this three-level outcome. Covariates derived from the literature and from preliminary bivariate analyses. All statistical tests were two-sided and were conducted at the alpha=0.05 level.
3. RESULTS
3.1 Change in SEP attendance probabilities over the course of the DOB Study
The final, best-fitting framework was a three-class model with measurement invariance over time (BIC 4-class model 200.42 versus BIC 3-class model 146.71). The overall fit of the three-class model was good (G2=38.42<46 degrees of freedom in model), and a model that did not assume measurement invariance had inferior fit (BIC 190.21).
3.1.1 SEP class typologies
The item-response probabilities (Figure 1) for the 3-class model solution convey the meaning and differentiating characteristics of the three SEP latent class typologies. Class 1 had the highest response probabilities for obtaining their syringes from an SEP, knowing others who used an SEP, and receiving syringes that they knew came from an SEP. Based on this response pattern, Class 1 best represented Direct SEP exchangers who are well networked with other SEP users. People in Class 2 indicated that they did not use an SEP, but they knew others who used an SEP and they received syringes that they knew came from an SEP. This class best represented a group of IDUs labeled here as Indirect SEP users. The third and final class was comprised of people who reported that they knew others who used SEPs but that they did not attend an SEP themselves nor did they receive syringes that they knew came from an SEP. Thus, we called this class the Isolated IDUs.
Figure 1.
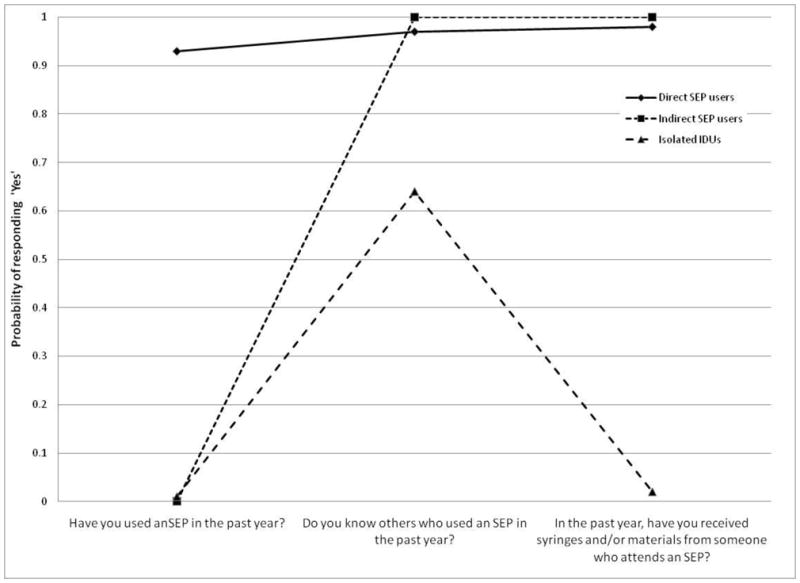
Item-response probabilities for SEP class typologies. Note, the item-response probabilities are conditional upon latent class membership. For example, the probability of responding ‘Yes’ to the item ‘Have you used an SEP in the past year?’ conditional upon membership in the Direct SEP users class is 0.93.
Table 2 reports the overall prevalence of the class typologies at Time 1 and Time 2. The study design called for disproportionate recruitment of non-SEP using IDUs, yet one year later, most IDUs had transitioned into Direct SEP users. It appears that more people who were Indirect users (versus Isolated IDUs) became Direct SEP users during this year’s time.
Table 2.
Prevalence at Time 1 and 2 for SEP class typologies
| Class | Label | Prevalence (%) at Time 1 | Prevalence (%) at Time 2 |
|---|---|---|---|
| 1 | Direct SEP users | 29.2 | 44.9 |
| 2 | Indirect SEP users | 34.2 | 21.4 |
| 3 | Isolated IDUs | 36.6 | 33.7 |
Table 3 lists the transition probabilities, that is, the probability of transitioning from one class to another, from Time 1 (baseline), to Time 2 (the one-year follow-up). The probability of being in the same class from Time 1 to Time 2 was greatest for the Direct SEP users. The probability of being in the same class one year later was substantially lower for all other groups. The probability of Time 1 Indirect SEP users becoming Direct SEP users at Time 2 was greater than the probability of remaining Indirect users or becoming Isolated IDUs at Time 2. Isolated users at Time 1 were more likely to become Direct SEP users than to become Indirect SEP users at Time 2. Most movement, in short, was toward direct SEP use. Finally, the overall transitions suggest a movement over time toward becoming more involved and connected with other drug users through the SEP or through connections with people who attend SEPs rather than a movement over time toward greater isolation (i.e., values below the diagonal are greater than those above the diagonal).
Table 3.
Transition probabilities from Time 1 to Time 2
| Time 2 status | |||
|---|---|---|---|
| Time 1 status | Direct SEP users | Indirect SEP users | Isolated IDUs |
| Direct SEP users | .686* | .078 | .236 |
| Indirect SEP users | .375 | .337 | .287 |
| Isolated IDUs | .328 | .208 | .464 |
Thus the probability of maintaining Direct SEP user at Time 1 and 2 is 0.686 while the probability of transitioning from the Direct SEP user class to the Isolated IDUs is 0.236.
Several covariates differentiated membership in the SEP classes at Time 1. City of recruitment, educational status, past month injection of speedballs, and the (log of the) number of injections per syringe were associated with the SEP classes at Time 1. No other socio-demographic, drug use, or risk behavior variables were significantly (p<.05) associated with Time 1 SEP class membership. Inclusion of the covariates did not meaningfully alter the item-response probabilities, the transition probabilities (data not shown), or the interpretations presented above. There was only a slight change in the LTA-generated prevalence of the SEP attendance typologies when the covariates were included in the model. Table 4 displays the characteristics of the typologies of SEP use and reports the adjusted Time 1 prevalence.
Table 4.
Characteristics of the SEP attendance groups at Time 1, adjusted LTA model
| Direct SEP users n= 154 | Indirect SEP users n=212 | Isolated IDUs n=204 | P value | ||
|---|---|---|---|---|---|
| 27% | 37.2% | 35.8% | |||
| City of recruitment | Hartford | 29.9 (46) | 5.7 (12) | 41.2 (84) | <0.0001 |
| Oakland | 31.8 (49) | 29.7 (63) | 14.2 (29) | <0.0001 | |
| Chicago | 38.3 (59) | 64.6 (137) | 44.6 (91) | <0.0001 | |
| Median age[IQR] | 42.5 [36, 48] | 41 [36, 48] | 39 [33, 45] | 0.0003 | |
| Female | 48.0 (74) | 41.0 (87) | 37.7 (77) | NS | |
| >high school education | 47.4 (73) | 60.4 (128) | 38.7 (79) | <0.0001 | |
| Homeless* | 32.5 (50) | 34.4 (73) | 38.2 (78) | NS | |
| Race/ethnicity | White/other | 24.0 (37) | 23.1 (49) | 14.2 (29) | χ24=15.15, p=0.004 |
| African-American | 34.4 (53) | 47.2 (100) | 42.2 (86) | ||
| Latino | 41.6 (64) | 29.7 (63) | 43.6 (89) | ||
| Past month injected cocaine | 29.2 (45) | 24.2 (51) | 19.7 (40) | NS | |
| Past month injected speedball | 49.3 (76) | 45.7 (97) | 38.2 (78) | 0.09 | |
| Past month Crack use | 51.6 (79) | 50.2 (106) | 42.9 (87) | NS | |
| Police contact* | 18.2 (28) | 15.1 (32) | 12.7 (26) | NS | |
| Overdose* | 20.8 (32) | 17.9 (38) | 12.7 (26) | NS | |
| Median number of injections per syringe [IQR] | 4.9 [1, 12.5] | 12.5 [1, 40.7] | 12.5 [4.9, 86.2] | <0.0001 |
IQR=interquartile range
in the past year
The direction of the associations between the covariates and Time 1 status indicated that Chicago participants were more likely to be in the Isolated IDUs (AOR 1.33) and Indirect SEP user (AOR 1.18) classes compared to the Direct users class. Hartford participants were least likely to be Indirect SEP users (AOR 0.19), and Oakland participants were least likely to be in the Isolated IDUs class (AOR 0.42). Indirect SEP users were more likely to have higher education levels (AOR 1.48). A greater number of injections per syringe was associated with membership in the Isolated IDUs (AOR 1.69) and Indirect SEP users class (AOR 1.54). Finally, past month injection of speedballs was least likely to occur among the Isolated IDU class (AOR 0.56).
The transition from one SEP user class to another in one year’s time was significantly (p<.05) influenced by city of recruitment, ethnicity, sex, educational status, having been stopped, cited, or arrested for carrying drug paraphernalia in the past year, homelessness status, and injecting speedballs. These associations are presented in Table
3.2 Multinomial regression results
3.2.1 Predictors of becoming a Direct SEP user
Variables associated with becoming a Direct SEP user versus transitioning to any other status included homelessness (AOR=2.0 [95% CI: 1.27, 3.14]), city of recruitment: Oakland (AOR=11.26 [95% CI: 6.27, 20.22]), past month injection of speedballs (AOR=1.82 [95% CI: 1.1, 2.94]), and having been stopped by the police for drug paraphernalia (AOR=2.98 [95% CI: 1.61, 5.52]).
3.2.2 Predictors of maintaining Direct SEP user status
Variables associated with remaining a Direct SEP user from Time 1 to Time 2 versus transitioning to any other status included female sex (AOR=1.81 [95% CI: 1.13, 2.91]), Latino ethnicity (AOR=1.89 [95% CI: 1.08, 3.30]), city of recruitment: Oakland (AOR=8.57 [95% CI: 4.48, 16.39]) or Hartford (AOR=2.89 [95% CI: 1.60, 5.23]), lower syringe re-use (AOR=0.45 [95% CI: 0.33, 0.60]), past month injection of speedballs (AOR=2.27 [95% CI: 1.38, 3.75]), and having been stopped by the police for drug paraphernalia (AOR=2.58 [95% CI: 1.29, 5.17]).
3.3 The effect of syringe exchange policy change on SEP attendance probabilities
As with the previous LTA, the final, best-fitting model for the data exploring syringe dispensing policy effects was a three-class model with measurement invariance over time. Also similar to the previous LTA, the three SEP attendance groups were replicated.
In the policy change cities there was, overall, a stronger maintenance of Indirect SEP user status (transition probability=0.736 Indirect SEP user vs. 0.56 for Isolated IDUs and Direct SEP users) over time and a higher increase in the prevalence of Indirect SEP users (from 43.2% to 50.6%) than of Direct SEP users (29.2% to 31.5%). Those who were Indirect SEP users at Time 1 were more likely to maintain their status or to become Direct SEP users at Time 2. With moderate probability, Direct SEP users were more likely to maintain their group or to become Indirect SEP users at Time 2. People who were Isolated IDUs at Time 1 had a greater probability of becoming an Indirect SEP user than becoming a Direct SEP user at Time 2 (Table 6).
Table 6.
Prevalence of SEP user typologies and transition probabilities over time
| Prevalence of typologies over time: Cities with changes to syringe policy only (N=228) | |||
|---|---|---|---|
| Group | Label | Prevalence at Time 1 | Prevalence at Time 2 |
| 1 | Direct SEP users | 29.2 | 31.5 |
| 2 | Indirect SEP users | 43.2 | 50.6 |
| 3 | Isolated IDUs | 27.6 | 17.8 |
| Transition probabilities from Time 1 to Time 2: Cities with changes to syringe policy (N=228) | |||
| Time 1 status | Time 2 status | ||
| Direct SEP users | Indirect SEP users | Isolated IDUs | |
| Direct SEP users | 0.557 | 0.391 | 0.052 |
| Indirect SEP users | 0.245 | 0.736 | 0.019 |
| Isolated IDUs | 0.170 | 0.269 | 0.560 |
Several covariates influenced the Time 1 status and the transitions over time in the two cities with altered syringe polices. Factors influencing the Time 1 typologies were city of recruitment, injecting cocaine in the past month, and ethnicity (all p<.05). Factors that affected the probability of any transition from one SEP user status to another included city of recruitment, homelessness status, injecting cocaine in the past month, and being stopped by the police for drug paraphernalia in the past year (Table 7). In particular, compared to Chicago, Direct SEP users in Hartford, where a nominal increase in the syringe cap policy was introduced, were more likely to become Isolated IDUs (AOR=20.76) than Indirect users if they transitioned classes from Time 1 to Time 2. Isolated IDUs in Hartford were more likely to become Direct SEP users (AOR=2.07), but Indirect SEP users experienced little change in status. Other factors influencing transitions from Time 1 to Time 2 revealed that being homeless increased the odds of Direct SEP users transitioning to Isolated IDUs at Time 2 (AOR=10.65) but homelessness also increased the odds of Indirect SEP users transitioning to the Direct SEP users class at Time 2 (AOR=2.00).
Table 7.
Adjusted odds ratios for covariates significantly (p<.05) associated with probability of transitioning from one status to another over one year’s time: syringe policy change analysis
| Time 1 | Time 2: Cities with changes to syringe policy (N=228) |
||
|---|---|---|---|
| Direct SEP users | Indirect SEP users | Isolated IDUs | |
| Hartford (ref=Chicago) | |||
| Direct SEP users | - | 0.33 | 20.76 |
| Indirect SEP users | 1.09 | - | 0.55 |
| Isolated IDUs | 2.07 | 0.57 | - |
| Homeless* | |||
| Direct SEP users | - | 1.69 | 10.65 |
| Indirect SEP users | 2.00 | - | 0.70 |
| Isolated IDUs | 0.80 | 1.07 | - |
| Injected cocaine | |||
| Direct SEP users | - | 0.79 | 0.33 |
| Indirect SEP users | 1.20 | - | 6.77 |
| Isolated IDUs | 1.35 | 0.81 | - |
| Stopped by police for drug paraphernalia* | |||
| Direct SEP users | - | 2.14 | 0.26 |
| Indirect SEP users | 1.05 | - | 8.46 |
| Isolated IDUs | 2.15 | 1.38 | - |
in the past year
Past month injection of cocaine was also associated with transitioning from Indirect SEP user to Isolated user status (AOR=6.77), but Direct SEP users who injected cocaine were less likely to change their status at Time 2 (AOR Indirect SEP users=0.79; AOR Isolated IDUs=0.33).
Being stopped by the police for carrying drug paraphernalia displayed a curious influence on the transition probabilities. At Time 1, Direct SEP users who reported being stopped by the police for paraphernalia were more likely to become Indirect SEP users (AOR=2.14) than to become Isolated IDUs (AOR=0.26) whereas Indirect SEP users who had been stopped by the police recently were more likely to become Isolated IDUs at Time 2 (AOR=8.46). However, the probability of transitioning from the Indirect SEP user class to the Isolated IDU class in the policy change cities was very low (probability=0.019). Isolated IDU were more likely to become Direct SEP users (AOR=2.15) than to become Indirect SEP users (AOR=1.38) if they had been stopped by the police for drug paraphernalia in the past year. Injection-related risk behaviors and healthcare utilization did not predict transition probabilities. Table 7 reports statistically significant associations.
4. DISCUSSION
This study found that, in one year’s time, IDUs living in three US cities with three different HIV risk environments and SEP operating characteristics tended to transition to direct use of SEPs. Transition probabilities in general and the odds over time of becoming and maintaining Direct SEP user status in specific were significantly influenced by city of recruitment, ethnicity, homelessness status, injecting speedballs, and police contact involving possession of drug paraphernalia in the past year. Of the SEP attendance typologies, Direct SEP users had the lowest rate of syringe re-use, indicating their better access to syringes.
Interestingly, changes in syringe dispensing policy were associated with an increase in the prevalence of Indirect SEP users from 43% to 51% with little impact on direct SEP use (29% to 31%). This finding is consistent with previous studies, reporting that legislation that modestly increased the cap on drug injectors’ access to clean syringes at SEPs had little effect on increasing syringe availability, decreasing risk of HIV transmission, or altering syringe re-use or receptive syringe sharing. (Bluthenthal et al., 2004; Heimer et al., 2002b) Policy changes may impact IDUs in the communities in many different ways; the present analysis was not designed to comprehensively assess the effects of these changes. Our findings do suggest that changes to syringe availability may have had more impact on expanding secondary exchange networks than on increasing the number of Direct SEP users. With greater syringe availability in the community, IDUs may have altered their SEP use behaviors due to police contact (as suggested by data reported in Table 7), due to stigma or discrimination associated with disclosure of injecting status that can accompany SEP use, or due to easier access through subsequently better equipped secondary exchange networks. While there is much gained by greater syringe availability through secondary exchange, it is important to note that one result of the shift to indirect SEP use following a dispensing policy change is the missed opportunity for exposure to relevant health information and access to other services such as vaccinations or treatment referrals which are derived from direct use of an SEP. Other, more creative means may be necessary to connect populations not using SEPs directly to services and public health information.
Factors associated with SEP user transitions in our analysis also included homelessness, injection of cocaine and speedballs, and being stopped by police for drug paraphernalia. Homelessness was associated with transitions away from direct SEP use. Perhaps because of their more transient status, homeless persons may find it more difficult to maintain direct SEP use and, lacking a stable housing situation, homeless persons are at greater risk of arrest for possession of syringes and tend to be more mobile. In addition, our analysis detected this association in multivariate logistic regressions, which found that homelessness predicted becoming but not maintaining Direct SEP user status, and in both of the LTAs, where homelessness influenced Direct SEP users to become Isolated users although this transition occurred with low probability. We also found that homelessness influenced Indirect SEP users to become Direct SEP users, a transition that occurred with moderate probability in one year’s time (probability=0.37 and 0.24 across LTAs). While their study did not consider transitions to or from indirect SEP use, Hagan et al., in a cohort study of IDUs in Washington state, found that IDUs who reported living on the streets or in a shelter were more than twice as likely as other IDUs to begin to use an exchange, but not to stop using an SEP if they had been using them after one year.
Injection of cocaine and speedballs were associated with the probability of transitioning to Direct SEP use and in the multivariate logistic regressions predicted becoming and maintaining Direct SEP use. These associations suggest that drug preference may have influenced SEP use. Due to the high frequency of injections necessitated by cocaine’s short half-life, (Hankins et al., 2002) cocaine injectors require the use of more clean syringes, otherwise IDUs must re-use their syringes. This analysis suggests that frequent injectors are seeking out SEPs, continuing to use this resource, and for those maintaining SEP use, are less often reusing their syringes (as Table 4 indicates), all key components of reducing HIV transmission and other potential harms associated with syringe re-use.
We also found that contact with police around drug paraphernalia was associated with becoming and maintaining Direct SEP user status in all cities while, in cities with a syringe dispensing policy change, police contact simultaneously improved direct SEP use for some typologies and reduced SEP use for others. Ethnographic and epidemiological research among IDUs has repeatedly found that fear of arrest is a factor in the syringe possession behavior of IDUs, (Bourgois, 1998; Clatts et al., 1998; Grund et al., 1992; Koester, 1994) and intensive, targeted street-level police interventions have been shown to reduce SEP use. (Bluthenthal et al., 1997; Davis et al., 2005; Heimer et al., 1996) By contrast, our findings, supplemented by research from a recent survey of SEPs in the United States, suggest that the relationship between SEP attendance and police contact may be a more nuanced one. In their survey of SEPs, Beletsky et al. found that, while some programs reported substantial burden of police interference with program functioning, approximately 20% of programs reported deriving new clients from police referrals.(Beletsky et al., 2009) Participation in the SEP equips IDUs in some cities in the U.S. with program identity cards that can shield individuals from police intervention, although it is not clear whether street-level officers are aware of and behave in compliance with these rules.(Beletsky et al., 2005; Beyer et al., 2002) Our findings provide individual level evidence of these aggregate trends. Being stopped by the police for drug paraphernalia possession in cities with a syringe dispensing policy change appeared to strongly influence Indirect SEP users into greater isolation (AOR=8.5), but this change was a rare occurrence (transition probability=0.02) among Indirect SEP users. More commonly (transition probability =0.39), police contact influenced Direct SEP users to become Indirect SEP users (AOR=2.1) and did not push them into the class of Isolated users (AOR=0.26). On a positive note, the syringe dispensing policy analysis revealed that Isolated IDUs who were stopped by the police were strongly influenced to become Direct SEP users (AOR=2.1), a transition that occurred with modest probability (transition probability=0.17).
Our findings suggest that police contact may act to promote SEP use. Martinez et al., (Martinez et al., 2007) in their cross-sectional study of SEPs in California, reported an association between legal SEP use and police contact involving drug paraphernalia. In light of our findings, the greater odds of police contact among users of legal versus illegal SEPs detected in their study might reflect the same higher odds of becoming and maintaining Direct SEP user status that we report. Other examples in the literature suggest that police contact can facilitate referrals of IDUs to harm reduction programs including supervised injecting facilities (DeBeck et al., 2008) and may spur drug treatment initiation. (Shutz et al., 1994; Weatherburn and Lind, 2001) Taken together, these data suggest that interactions between IDUs and police around drug paraphernalia have the potential to encourage SEP use which may, in turn, promote other harm reducing interventions. The critical issue is the nature of police-IDU interaction. Interactions where an IDU may be referred to a service rather than facing adverse consequences for being in possession of injecting equipment are likely to produce different subsequent responses on the part of the IDU. We did not examine whether police had received training in promoting SEP use among IDUs in these communities, however, it is likely that IDUs would benefit from police training in referral to critical public health interventions such as SEP, drug treatment, and primary care. Finally, we note that engaging in injection-related risk behaviors and frequent healthcare utilization did not predict transitions in SEP use over one year or over time in policy-change cities. Longitudinal studies of IDUs who transition to and away from direct and indirect SEP use could help better understand the potential changes in risk behaviors, healthcare utilization, and syringe (re)distribution in the community that may occur subsequent to transition.
These findings must be considered in relation to a number of study limitations and leveraged by its strengths. All data from this study were self-reported thus measurement error and reporting biases may have occurred. The full information maximum likelihood approach of the LTA permitted use of data from all participants, even if data were missing on the SEP use indicators at either time point. This approach is an improvement over traditional regression techniques that would have dropped these participants from the analysis or would have required imputation techniques to retain their data. Low follow-up rates precluded the exploration of time 2 covariate effects on latent transitions. Unmeasured confounders such as community characteristics, incidence of police crackdowns, and harm reduction policing interventions that may have taken place during the study period could explain some of the observed associations and transitions over time. The non-random sampling scheme may not have resulted in recruitment of a sample representative of the IDU communities in the three study cities, so generalizability of our findings beyond predominantly minority urban IDU populations in places with legal SEPs may be questionable. Demographic and drug use characteristic differences were few between the SEP user classes, suggesting they were recruited from similar networks of IDUs. The injection risk behaviors, especially syringe re-use and sharing behaviors (though not statistically significant), did reflect differences between direct SEP users and non SEP users that were consistent with other studies (Vlahov et al., 1997; Heimer et al., 1998; Bluthenthal et al., 2000). Thus, while our sampling strategy may have resulted in narrowing the sociodemographic differences between SEP customers and non-customers, there were differences in risk behaviors consistent with expectations based on previous studies. The use of a three-city sample as well as two independent recruitment methods—through networks or by independent street outreach—suggests that the results may be applicable to other areas in the US.
The question of whether the sampling scheme may have influenced the probability of transitioning to SEP use is important to consider. While people in the outreach sample may or may not be part of a network of IDUs with one or more members who use the SEP, one may assume that it is more likely that non-users whose social network includes one or more SEP users will transition to SEP use, given the influence of social networks on individual behaviors. However, the purpose of this manuscript was to identify factors that increase or decrease the likelihood of transitioning to a safe source for obtaining syringes and other injection supplies and not to accurately determine the percentage of people who switched based on latent class, since the exact proportion is, ultimately, influenced by factors that are not generalizeable. A minority (roughly 30%) of participants changed class and although most moved closer to SEP use, some moved away. The fact that the proportion of people who changed their SEP use status in one year’s time was consistent with that found in another study examining change in SEP use in a six-month follow-up period among high-risk IDUs (approximately a third)(Bluthenthal et al., 2000) is encouraging of the validity of the findings.
Participation in the DOB study may have influenced health and social service utilization, including SEP use. If participants requested information or referrals to services in the community, study personnel provided this information; doing otherwise would have been unethical. Such provision of information or referrals may have influenced the absolute value of the transitions we detected, but is unlikely to have influenced the overall findings that (1) SEP users are likely to remain such, (2) indirect and isolated non-users transition with similar probability (.375 and .328, respectively), and (3) policy changes had little impact on promoting uptake of SEP use by non-users. While we could look generally at the effect of syringe availability policy change on SEP use, there was insufficient power to stratify by city to examine what type of policy change produced the most effect. It is possible that moving from an exchange to a distribution policy in Chicago had the potential to drastically increase syringe availability and therefore indirect SEP use, whereas the small cap increase implemented in Hartford only favored increasing direct SEP use. We did not analyze whether transitions to or from SEP use in this sample were associated with subsequent changes in syringe distribution to others or with reductions in receptive syringe sharing or other HIV risk behaviors. The sample size within these transition cells was too small to analyze such associations; a future cohort study could address this limitation. Finally, we lacked the sample size to stratify our LTAs by city, which would have permitted exploration of the effects of the specific syringe dispensing policy changes, or by ethnicity, which would have allowed for exploration of possible ethnic disparities in SEP use typologies and transitions.
Nonetheless, this study suggests that IDUs alter their SEP use status over one year’s time and that Direct SEP users rarely sever ties entirely with the SEP. Cross-sectional analyses of direct SEP use may underestimate the effects of SEPs and SEP-based interventions if they do not consider the sizable reach of secondary exchange networks. This is especially important because secondary syringe exchange appears to be affected more than direct syringe exchange by syringe dispensing policies that increase syringe availability. Results from this study point to the influence of police contact involving possession of drug paraphernalia as a possible tool in public health interventions for IDUs, including, counterintuitively, the encouragement of SEP attendance.
Table 5.
Adjusted odds ratios of covariates significantly (p<.05) associated with probability of transitioning from one status to another over one year’s time
| Time 1 status | Time 2 status |
||
|---|---|---|---|
| Direct SEP users | Indirect SEP users | Isolated IDUs | |
| Hartford (ref=Chicago) | |||
| Direct SEP users | - | 0.30 | 1.01 |
| Indirect SEP users | 1.16 | - | 1.35 |
| Isolated IDUs | 1.02 | 0.44 | - |
| Oakland | |||
| Direct SEP users | - | 0.48 | 0.83 |
| Indirect SEP users | 1.52 | - | 0.89 |
| Isolated IDUs | 1.60 | 0.67 | - |
| White/other ethnicity (ref=African American) | |||
| Direct SEP users | - | 3.19 | 1.02 |
| Indirect SEP users | 1.14 | - | 0.92 |
| Isolated IDUs | 1.28 | 1.01 | - |
| Latino | |||
| Direct SEP users | - | 1.76 | 1.03 |
| Indirect SEP users | 1.11 | - | 0.85 |
| Isolated IDUs | 1.22 | 1.26 | - |
| Female (ref=Male) | |||
| Direct SEP users | - | 0.91 | 0.65 |
| Indirect SEP users | 1.10 | - | 0.99 |
| Isolated IDUs | 0.93 | 0.73 | - |
| >high school education | |||
| Direct SEP users | - | 0.54 | 0.99 |
| Indirect SEP users | 0.68 | - | 1.07 |
| Isolated IDUs | 1.19 | 0.91 | - |
| Stopped by police for drug paraphernalia* | |||
| Direct SEP users | - | 1.24 | 0.87 |
| Indirect SEP users | 1.29 | - | 1.26 |
| Isolated IDUs | 1.29 | 0.96 | - |
| Homeless* | |||
| Direct SEP users | - | 1.06 | 1.42 |
| Indirect SEP users | 1.70 | - | 1.09 |
| Isolated IDUs | 0.99 | 1.03 | - |
| Injected speedball | |||
| Direct SEP users | - | 0.33 | 1.01 |
| Indirect SEP users | 0.93 | - | 0.86 |
| Isolated IDUs | 1.17 | 1.05 | - |
In the past year;
- = reference cell in row. For example, reading from left to right, females who were Direct SEP users at Time 1 were 0.65 times as likely to become Isolated users than to maintain their Direct SEP user status (reference) at Time 2.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Bastos FI, Strathdee SA. Evaluating effectiveness of syringe exchange programmes: current issues and future prospects. Social science & medicine (1982) 2000;51:1771–1782. doi: 10.1016/s0277-9536(00)00109-x. [DOI] [PubMed] [Google Scholar]
- Beletsky L, Heimer R, Grau LE. AIDS Science Day. Yale Center for Interdisciplinary Research on AIDS; New Haven, CT: 2009. Police-Public Health Collaboration in HIV Prevention: A Needs-Assessment Survey. [Google Scholar]
- Beletsky L, Macalino GE, Burris S. Attitudes of Police Officers towards Syringe Access, Occupational Needle-Sticks, and Drug Use: A Qualitative Study of One City Police Department in the United States. International Journal of Drug Policy. 2005;16:267–274. [Google Scholar]
- Beyer L, Crofts N, Reid G. Drug offending and criminal justice responses: practitioners’ perspectives. The International journal on drug policy. 2002;13:199–207. [Google Scholar]
- Bluthenthal RN, Anderson R, Flynn NM, Kral AH. Higher syringe coverage is associated with lower odds of HIV risk and does not increase unsafe syringe disposal among syringe exchange program clients. Drug and alcohol dependence. 2007a;89:214–222. doi: 10.1016/j.drugalcdep.2006.12.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bluthenthal RN, Kral AH, Gee L, Erringer EA, Edlin BR. The effect of syringe exchange use on high-risk injection drug users: a cohort study. AIDS (London, England) 2000;14:605–611. doi: 10.1097/00002030-200003310-00015. [DOI] [PubMed] [Google Scholar]
- Bluthenthal RN, Kral AH, Lorvick J, Watters JK. Impact of law enforcement on syringe exchange programs: a look at Oakland and San Francisco. Medical anthropology. 1997;18:61–83. doi: 10.1080/01459740.1997.9966150. [DOI] [PubMed] [Google Scholar]
- Bluthenthal RN, Malik MR, Grau LE, Singer M, Marshall P, Heimer R. Sterile syringe access conditions and variations in HIV risk among drug injectors in three cities. Addiction (Abingdon, England) 2004;99:1136–1146. doi: 10.1111/j.1360-0443.2004.00694.x. [DOI] [PubMed] [Google Scholar]
- Bluthenthal RN, Ridgeway G, Schell T, Anderson R, Flynn NM, Kral AH. Examination of the association between syringe exchange program (SEP) dispensation policy and SEP client-level syringe coverage among injection drug users. Addiction (Abingdon, England) 2007b;102:638–646. doi: 10.1111/j.1360-0443.2006.01741.x. [DOI] [PubMed] [Google Scholar]
- Bourgois P. The moral economies of homeless heroin addicts: confronting ethnography, HIV risk, and everyday violence in San Francisco shooting encampments. Substance use & misuse. 1998;33:2323–2351. doi: 10.3109/10826089809056260. [DOI] [PubMed] [Google Scholar]
- Bryant J, Hopwood M. Secondary exchange of sterile injecting equipment in a high distribution environment: A mixed method analysis in south east Sydney, Australia. International Journal of Drug Policy. 2009;20:324–328. doi: 10.1016/j.drugpo.2008.06.006. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. HIV/AIDS Surveillance Report, 2007. Vol. 19. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; Atlanta: 2009. [Google Scholar]
- Chaisson RE, Moss AR, Onishi R, Osmond D, Carlson JR. Human immunodeficiency virus infection in heterosexual intravenous drug users in San Francisco. American journal of public health. 1987;77:169–172. doi: 10.2105/ajph.77.2.169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clatts MC, Sotheran JL, Luciano PA, Gallo TM, Kochems LM. The Impact of Drug Paraphernalia Laws on HIV Risk among Persons who Inject Illegal Drugs: Implications for Public Policy. In: Fish JM, editor. How to Legalize Drugs. Jason Aronson; Northvale, NJ: 1998. pp. 90–101. [Google Scholar]
- Davis CS, Burris S, Kraut-Becher J, Lynch KG, Metzger D. Effects of an intensive street-level police intervention on syringe exchange program use in Philadelphia, PA. American journal of public health. 2005;95:233–236. doi: 10.2105/AJPH.2003.033563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De P, Cox J, Boivin JF, Platt R, Jolly A. Social Network-Related Risk Factors for Bloodborne Virus Infections Among Injection Drug Users Receiving Syringes through Secondary Exchange. Journal of Urban Health. 2008;85:77–89. doi: 10.1007/s11524-007-9225-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeBeck K, Wood E, Zhang R, Tyndall M, Montaner J, Kerr T. Police and public health partnerships: evidence from the evaluation of Vancouver’s supervised injection facility. Substance abuse treatment, prevention, and policy. 2008;3:11. doi: 10.1186/1747-597X-3-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Des Jarlais DC, Marmor M, Paone D, Titus S, Shi Q, Perlis T, Jose B, Friedman SR. HIV incidence among injecting drug users in New York City syringe-exchange programmes. Lancet. 1996;348:987–991. doi: 10.1016/s0140-6736(96)02536-6. [DOI] [PubMed] [Google Scholar]
- Grau LE, Bluthenthal RN, Marshall P, Singer M, Heimer R. Psychosocial and behavioral differences among drug injectors who use and do not use syringe exchange programs. AIDS and behavior. 2005;9:495–504. doi: 10.1007/s10461-005-9020-3. [DOI] [PubMed] [Google Scholar]
- Green TC, Smith-Rohrberg D, Allen N, Heimer R, Grau LE. Exploring the diffusion of benefit of syringe exchange programs in a cohort of injecting drug users: Changes in injecting behaviors and injecting-related morbidity. Summer Institute in Longitudinal Research, Center for Advancing Longitudinal Drug Abuse Research, UCLA; Los Angeles, CA: 2006. [Google Scholar]
- Grund JP, Stern LS, Kaplan CD, Adriaans NF, Drucker E. Drug use contexts and HIV-consequences: the effect of drug policy on patterns of everyday drug use in Rotterdam and the Bronx. British journal of addiction. 1992;87:381–392. doi: 10.1111/j.1360-0443.1992.tb01939.x. [DOI] [PubMed] [Google Scholar]
- Hankins C, Alary M, Parent R, Blanchette C, Claessens C. Continuing HIV transmission among injection drug users in Eastern Central Canada: the SurvUDI Study, 1995 to 2000. Journal of acquired immune deficiency syndromes (1999) 2002;30:514–521. doi: 10.1097/00126334-200208150-00007. [DOI] [PubMed] [Google Scholar]
- Heimer R. Community coverage and HIV prevention: Assessing metrics for estimating HIV incidence through syringe exchange. The International journal on drug policy. 2008 doi: 10.1016/j.drugpo.2007.12.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heimer R, Bluthenthal RN, Singer M, Khoshnood K. Structural impediments to operational syringe-exchange programs. AIDS & public policy journal. 1996;11:169–184. [PubMed] [Google Scholar]
- Heimer R, Clair S, Grau LE, Bluthenthal RN, Marshall PA, Singer M. Hepatitis-associated knowledge is low and risks are high among HIV-aware injection drug users in three US cities. Addiction (Abingdon, England) 2002a;97:1277–1287. doi: 10.1046/j.1360-0443.2002.t01-1-00211.x. [DOI] [PubMed] [Google Scholar]
- Heimer R, Clair S, Teng W, Grau LE, Khoshnood K, Singer M. Effects of increasing syringe availability on syringe-exchange use and HIV risk: Connecticut, 1990–2001. J Urban Health. 2002b;79:556–570. doi: 10.1093/jurban/79.4.556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heimer R, Khoshnood K, Bigg D, Guydish J, Junge J. Syringe use and re-use: effects of syringe exchange programs in four cities. Journal of acquired immune deficiency syndrome and human retrovirology. 1998;18(Suppl 1):S37–44. doi: 10.1097/00042560-199802001-00008. [DOI] [PubMed] [Google Scholar]
- Heinzerling KG, Kral AH, Flynn NM, Anderson RL, Scott A, Gilbert ML, Asch SM, Bluthenthal RN. Human immunodeficiency virus and hepatitis C virus testing services at syringe exchange programs: Availability and outcomes. Journal of substance abuse treatment. 2007;32:423–429. doi: 10.1016/j.jsat.2006.11.002. [DOI] [PubMed] [Google Scholar]
- Huo D, Bailey SL, Hershow RC, Ouellet L. Drug use and HIV risk practices of secondary and primary needle exchange users. AIDS Educ Prev. 2005;17:170–184. doi: 10.1521/aeap.17.3.170.62900. [DOI] [PubMed] [Google Scholar]
- Koester SK. Copping, Running, and Paraphernalia Laws: Contextual and Needle Risk Behavior Among Injection Drug Users in Denver. Human Organization. 1994;53:287–295. [Google Scholar]
- Kral AH, Anderson R, Flynn NM, Bluthenthal RN. Injection risk behaviors among clients of syringe exchange programs with different syringe dispensation policies. Journal of acquired immune deficiency syndromes (1999) 2004;37:1307–1312. doi: 10.1097/01.qai.0000127054.60503.9a. [DOI] [PubMed] [Google Scholar]
- Lanza ST, Collins LM. A new SAS procedure for latent transition analysis: transitions in dating and sexual risk behavior. Developmental psychology. 2008;44:446–456. doi: 10.1037/0012-1649.44.2.446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lorvick J, Bluthenthal RN, Scott A, Gilbert ML, Riehman KS, Anderson RL, Flynn NM, Kral AH. Secondary Syringe Exchange Among Users of 23 California Syringe Exchange Programs. Substance use & misuse. 2006;41:865–882. doi: 10.1080/10826080600669041. [DOI] [PubMed] [Google Scholar]
- Marmor M, Des Jarlais DC, Cohen H, Friedman SR, Beatrice ST, Dubin N, el-Sadr W, Mildvan D, Yancovitz S, Mathur U, et al. Risk factors for infection with human immunodeficiency virus among intravenous drug abusers in New York City. AIDS (London, England) 1987;1:39–44. [PubMed] [Google Scholar]
- Martinez AN, Bluthenthal RN, Lorvick J, Anderson R, Flynn N, Kral AH. The impact of legalizing syringe exchange programs on arrests among injection drug users in California. J Urban Health. 2007;84:423–435. doi: 10.1007/s11524-006-9139-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthen LK, Muthen B. Mplus User’s Guide. Muthen & Muthen; Los Angeles: 2007. [Google Scholar]
- Schoenbaum EE, Hartel D, Selwyn PA, Klein RS, Davenny K, Rogers M, Feiner C, Friedland G. Risk factors for human immunodeficiency virus infection in intravenous drug users. The New England journal of medicine. 1989;321:874–879. doi: 10.1056/NEJM198909283211306. [DOI] [PubMed] [Google Scholar]
- Sears C, Guydish JR, Weltzien EK, Lum PJ. Investigation of a Secondary Syringe Exchange Program for Homeless Young Adult Injection Drug Users in San Francisco, California, U.S.A. JAIDS Journal of Acquired Immune Deficiency Syndromes. 2001;27:193–201. doi: 10.1097/00126334-200106010-00015. [DOI] [PubMed] [Google Scholar]
- Shutz C, Rapiti E, Vlahov D, Anthony J. Suspected determinants of enrollment into detoxification and methadone treatment among injecting drug users. Drug and alcohol dependence. 1994;36:129–138. doi: 10.1016/0376-8716(94)90095-7. [DOI] [PubMed] [Google Scholar]
- Singer M, Irizarry R, Schensul JJ. Needle Access as an AIDS Prevention Strategy for IV Drug Users: A Research Perspective. Human Organization. 1991;50:142–153. [Google Scholar]
- Strathdee SA, Celentano DD, Shah N, Lyles C, Stambolis VA, Macalino G, Nelson K, Vlahov D. Needle-exchange attendance and health care utilization promote entry into detoxification. J Urban Health. 1999;76:448–460. doi: 10.1007/BF02351502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Valente TW, Foreman RK, Junge B, Vlahov D. Satellite exchange in the Baltimore Needle Exchange Program. Public Health Rep. 1998;113(Suppl 1):90–96. [PMC free article] [PubMed] [Google Scholar]
- Vlahov D, Junge B, Brookmeyer R, Cohn S, Riley E, Armenian H, Beilenson P. Reductions in high-risk drug use behaviors among participants in the Baltimore needle exchange program. Journal of Acquired Immune Deficiency Syndromes and Human Retrovirology. 1997;16 (5):400–6. doi: 10.1097/00042560-199712150-00014. [DOI] [PubMed] [Google Scholar]
- Weatherburn D, Lind B. Street-level drug law enforcement and entry into methadone maintenance treatment. Addiction (Abingdon, England) 2001;96:577–587. doi: 10.1046/j.1360-0443.2001.9645776.x. [DOI] [PubMed] [Google Scholar]