

Abstract
Background:
Perioperative shivering is a common problem during anaesthesia. Apart from physical warming many drugs have also been used for prevention of shivering. Ketamine has been used for preventing shivering during anaesthesia in doses of 0.5 to 0.75mg kg-1, but even these doses causes too much sedation and hallucination. Ondansetron (8 mg) has been recently evaluated for its perioperative antishivering effect in patients under anaethesia. Present study was conducted to evaluate the efficacy and safety of low dose Ketamine (0.25mg kg-1) and Ondansetron (4 mg) for prevention of shivering during spinal anaesthesia.
Patients & Methods:
Total 120 patients undergoing lower abdominal surgery under spinal anaesthesia were included. 3ml of hyperbaric bupivacaine 0.5% was used for spinal anaesthesia. After intrathecal injection, the patients were randomly divided in 3 groups of 40 each who received Ketamine 0.25mg kg-1or Ondansetron 4mg IV or Saline. Vitals, temperature and shivering scores were recorded every 5 minutes. Side effects i.e. hypotension, nausea and vomiting, sedation and hallucinations were also recorded.
Results:
Fall in temperature was more significant in saline and ondansetron group (gp) than in ketamine group at all time interval. Out of 40 patients, shivering was maximum & seen in 17 patients (42.50%) in saline gp, 4 patients (10%) in ondansetron gp and in only 1patient (2.5%) in ketamine gp. Odd ratio of ketamine, ondansetron and saline are 1, 4.33 and 28.33 respectively which means that shivering in saline gp was 28.83 times higher than ketamine gp and 6.65 times higher than in ondansetron .Shivering rate was 4.33 times higher in ondansetron gp than in ketamine gp. Hypotension was lowest in ketamine gp (10%) in comparison to ondansetron gp (22.5%) and saline gp. (20%). Mild sedation was seen in almost all (95%) patients in ketamine gp,
Conclusion:
Prophylactic low dose ketamine (0.25mg kg-1) and Ondansetron (4mg) significantly decreased shivering in patients undergoing spinal anaesthesia without significant side effects.
Keywords: Shivering, Spinal anaesthesia, Ketamine, Ondansetron
The normal human core temperature ranges from 36.5°C to 37.5°C.1 Thermal inputs are integrated at the level of the anterior hypothalamus, which compares peripheral information with a threshold value, or the set-point. Temperatures higher than this set point will trigger responses to cool the body, while temperatures lower than this set point will activate reflexes to warm the body.2 Both general and regional anaesthesia is known to affect the efficiency of this homeostatic system and may result in different degrees of perioperative hypothermia. Regional anaesthesia also decreases this threshold by 0.5°C, triggering vasoconstriction and shivering above level of block.3 this reduction in threshold is proportional to the number of spinal segments blocked, advanced age and high-level spinal blockade.4 Perioperative hypothermia and shivering is one of the frequent, undesirable and unpleasant complications of both general and regional anaesthesia. The incidence of shivering is up to 40-60% even in regional anaesthesia.5 Shivering causes increased metabolic activity and increased oxygen consumption up to 100%. It also cause arterial hypoxia and has been shown to correlate with increased risk of myocardial ischemia. It also increases intracranial and intraocular pressure. The other effects are increase in cardiac output, peripheral resistance, carbon dioxide production, lactic acidosis. Moreover it also interferes with ECG and oxygen saturation monitoring (pulse oximetry).6 The most reliable method and gold standard of core temperature monitoring is tympanic temperature monitoring by using tympanic probe.7
Perioperative hypothermia and shivering is usually prevented by physical methods like surface warming. and pharmacologically by drugs like pethidine, tramadol, and clonidine etc.8
Recently ketamine and ondansetron have been tried to prevent shivering during anaesthesia with good results. Ketamine a competitive NMDA receptor antagonist has a role in thermoregulation at various levels. NMDA receptor modulates noradrenergic and serotoninergic neurons in locus coeruleus. It is used as antishivering agent in dose of 0.5-0.75mg kg-1 IV. But even in these doses it causes side effects i.e. drowsiness, hallucination and delirium.6,9
Ondansetron is 5HT 3 receptor antagonist, primarily used to prevent emesis. Recently it has also been tried successfully for prevention of shivering in dose of 8mg IV without any side effects.10 As there are very few studies in relation to use of prophylactic ketamine and ondansetron for prevention of shivering during spinal anaesthesia and there is no comparative study evaluating use of low dose ketamine and ondansetron for prevention of shivering during spinal anaesthesia. So we conducted the present study to evaluate and compare the relative efficacy and safety of low dose ketamine (0.25 mg kg-1) and ondansetron (4 mg) for prevention of shivering during spinal anaesthesia.
PATIENTS AND METHODS
This was a prospective, randomized, and placebo controlled study. After the approval of the institute's ethics committee and obtaining written informed consent 120 adult patients of ASA physical status I&II, undergoing elective lower abdominal surgical procedures (general and gynaecological surgery) were included. Surgical procedure included Hernioplasty, appendicectomy or cystolithotomy. Gyanaecological procedure included vaginal hysterectomy or abdominal hysterectomy. Patients with thyroid disorder, severe cardiopulmonary disease, pregnancy, uncooperative patients and patients requiring blood transfusion were excluded. The selected patients were randomly allocated to 3 groups containing 40 patients each according to the study drug; Placebo or Saline group (Group P), Ondansetron 4mg group (Group O) and Ketamine 0.25 mg kg-1group (Group K).
All the patients were premedicated with 0.2mg kg-1of oral Diazepam at night and 1 hour before coming to the operation room. In the operating room routine standard monitoring was used in all patients. The temperature of the operating room was maintained at 24°C-26°C by adjusting the temperature setting of air conditioner. Before the spinal anaesthesia procedure, each patient was preloaded with 15ml kg-1of Ringer Lactate solution. Subarachnoid anaesthesia was instituted at either L3/4 or L4/5 interspace with 3ml of 0.5% hyperbaric Bupivacaine. Tympanic temperature was monitored with Braun thermoscan thermometer every 5 minute till end of the surgical procedure. The intravenous fluid kept at room temperature (24°C- 26°C) were infused and all the patients were covered with standard single blanket.
Just after the intrathecal injection, one of the study drugs was given as IV bolus. During surgery, shivering score was recorded at 5 min interval. Shivering was graded using a scale similar to that validated by Tsai and Chu.8 In which Grade 0: no shivering, Grade 1: piloerection or peripheral vasoconstriction but no visible shivering, Grade 2: muscular activity in only one muscle group, Grade 3: muscular activity in more than one muscle group but not generalized and Grade 4: shivering involving the whole body.
If 15 minutes after spinal anaesthesia and concomitant administration of a prophylactic dose of one of the study drugs, the patients shivered to at least grade 3, shivering was considered significant and prophylaxis as ineffective and Pethidine 0.5mg kg-1IV was given as rescue drug. Side effects such as hypotension, nausea and vomiting, sedation and hallucinations were recorded.
The degree of sedation was assessed on 5 point scale where 1: fully awake and oriented patient, 2:Drowsy, 3:eyes closed, arousable on command, 4 :eyes closed, arousable to physical stimuli, 5: eyes closed and patient unarousable to physical stimuli.
Data analysis was done in SPSS 11.5 and Epi Info 3.3.2. Parametric test was applied to identify the significance of the variables. P value of <0.05 was considered significant for the test. Odds ratio was calculated to find the effectiveness of different groups in prevention of shivering.
RESULTS
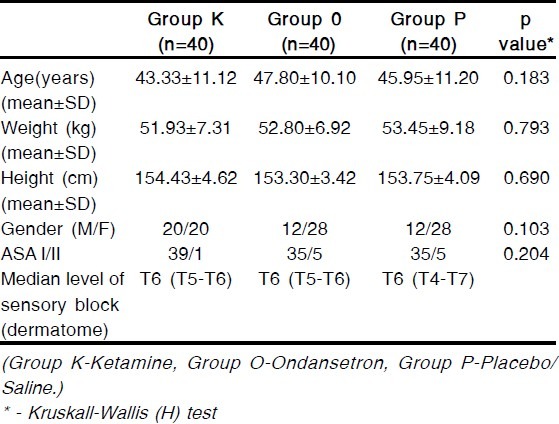
Total 120 patients were enrolled in this study, 40 in ketamine group (Group K), 40 in ondansetron group (Group O) and 40 in normal saline or placebo group (Group P). The groups were comparable with respect to age, gender, weight, ASA grade and median level of sensory block. (Table 1)
Table 1.
Comparison of patient characteristics among three groups
Ear temperature was recorded every 5 minutes during intraoperative period till the end of operation. All patients in all the 3 groups had decrease in ear temperature from baseline value after spinal anaesthesia. Temperature decreased more in ondansetron and saline groups than in ketamine group. p value was found to be significant (<0.05) at every measurement between ketamine and ondansetron groups and ketamine and normal saline groups throughout the study period. (Figure- 1)
Figure 1.
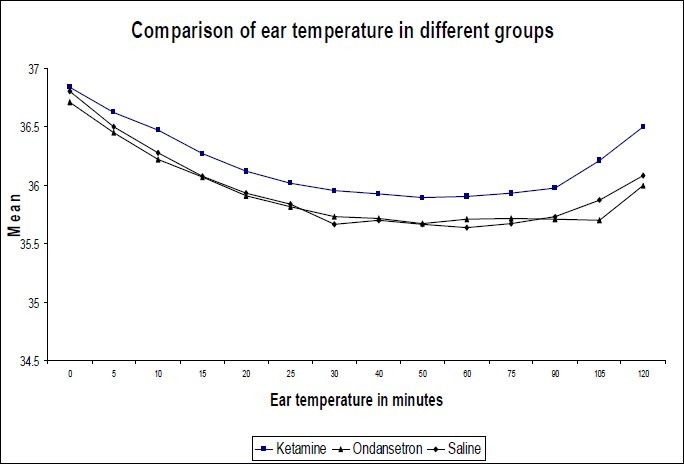
Comparison of ear temperature
In this study out of 40 patients in each group, shivering was seen in 17 patients (42.50%) in normal saline group, 4 patients (10%) in ondansetron group and 1patient (2.5%) in ketamine group. Shivering was taken as significant when the patient shivered at least to grade 3 (Tsai and chu grading of shivering) and occurred after 15 minutes of spinal anaesthesia. Such patients were treated with pethidine 0.5mg kg-1IV. Among the groups, shivering is highly significant (p<0.001) where odds of ketamine, ondansetron and normal saline are 1, 4.33 and 28.33 respectively. The odds between ketamine and normal saline is 1:28.83 (p<0.001). Similarly, the odds between ketamine and ondansetron is 1:4.33 (p<0.001) and the odds between ondansetron and normal saline is 1:6.65 ( p<0.001), which means that shivering in saline gp was 28.83 times higher than ketamine gp and 6.65 times higher than in ondansetron Shivering rate was 4.33 times higher in ondansetron gp than in ketamine gp. (Figure- 2)
Figure 2.
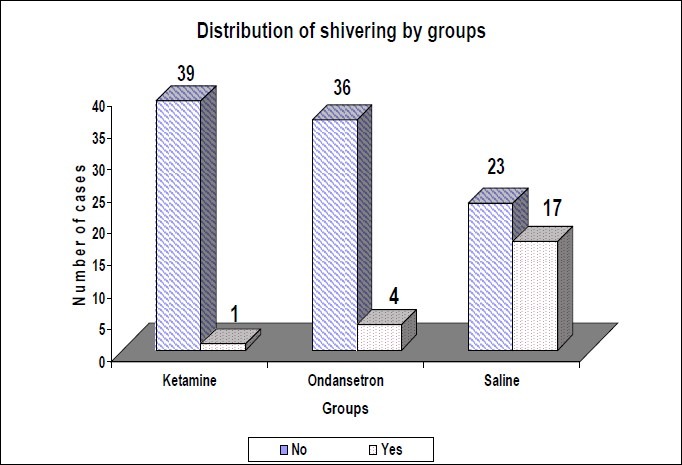
Distribution of shivering
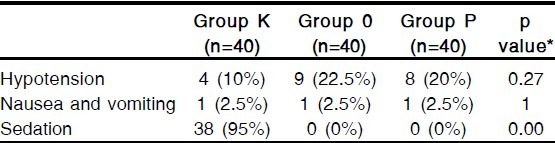
Hypotension was seen in 4 cases (10%) in ketamine group, 9 cases (22.5%) in ondansetron group and 8 cases (20%) in normal saline group. Mild sedation was seen in 38 cases (95%) in ketamine group, most of them were sedated to grade 2 and only 2 were of grade 3. It is obvious that no sedation was seen in ondansetron and normal saline groups. Hallucination was not noted even in the ketamine group. (Table-2)
Table 2.
Hypotension, nausea and vomiting and sedation incidence of groups:
DISCUSSION
In our study we investigated the comparative efficacy and safety of prophylactic low dose of ondansetron and ketamine (with different mechanism of action) for prevention of shivering during spinal anaesthesia. The median level of sensory block after 15 minutes of spinal anaesthesia was comparable (up to T6) in all 3 study groups. Hemodynamic parameters like heart rate, systolic blood pressure, diastolic blood pressure and mean arterial pressure were monitored every 5 minutes throughout intraoperative period. There was no difference among the 3 groups in relation to hemodynamic parameters. These results were consistent with previous studies by Sagir et al9 and Kelsaka et al10. In their study also there was no difference among the groups regarding hemodynamic values. In this study, tympanic temperature was measured using non invasive Braun thermoscan thermometer. Tympanic temperature is one of the most reliable site for measurement of core temperature and correlates well with brain temperature. The mean tympanic temperature decreased significantly after spinal anaesthesia in all groups with respect to baseline values. This is expected because hypothermia occurs during spinal anaesthesia due to internal redistribution of body heat, heat loss to environment and inhibition of centrally mediated thermoregulatory control. In this study mean tympanic temperature decreased significantly in ondansetron and saline groups than in ketamine group. p value was found to be significant (p<0.05) at every measurement between ketamine and ondansetron groups. Likewise p value was found to be significant at 10, 15, 30, 40, 50, 60, 75 and 90 minutes when comparing between ketamine (0.25mg kg-1) and normal saline groups. In the study done by Kelsaka et al10 core temperature was preserved in group's ondansetron (8mg) and pethidine (0.4mg kg-1) with respect to control group during intraoperative period after spinal anaesthesia. In the study done by Sagir et al9 , the decrease of core temperature seen in control group were significantly more than other groups beginning from the 10[th]minutes (p<0.001). Other groups were ketamine (0.5mg kg-1), granisetron (3mg), ketamine (0.25mg) + granisetron (1.5mg). In our study also, temperature was preserved in ketamine group with respect to control group. This relative preservation of temperature may be due to vasoconstrictive action of ketamine. But in the study of Kelsaka et al10 , the temperature was preserved with respect to control group in ondansetron group also which was not seen in our study. We used small dose (4mg) of ondansetron while Kelsaka et al10 , used 8 mg ondansetron that may be one of the reason.
In this study, shivering was graded using a scale that was validated by Tsai and Chu.8 The prophylactic drug was considered ineffective if the patient shivered to grade 3 and pethidine 0.5mg kg-1IV was given to control the shivering. Sagir et al9 in their study used same protocol. In our study, the incidence of shivering was 42.50% in the control group. In the study by Sagir et al,9 the shivering rate was 55% in the control group. Shivering was observed in 36% in Kelsaka et al study.10 In the study done by Bilotta et al,11 shivering rate was 57% in the control group. In our study, tablet diazepam (0.2mg kg-1) was used as premedication. In the study of Kelsaka et al,10 also 10mg of diazepam was used as premedication. In the study of Sagir and Bilotta, no premedication was used. The relatively low incidence of shivering in the control group in our study and study by Kelsaka et al may be attributable to diazepam which has antishivering property.
Ondansetron, which is a specific 5-HT3 receptor antagonist, is widely used antiemetic drug. The mechanism of action could be related to the inhibition of serotonin reuptake on the preoptic anterior hypothalamic region. 5-HT3 receptors may also influence both heat production and heat loss pathways. The recommended doses of Ondansetron for prevention of postoperative nausea & vomiting is 4-8 mg in adult patients. Kelsaka et al10 compared the 8mg ondansetron with pethidine for prevention of shivering and found the same antishivering effect and the incidence of shivering was 8% in ondansetron group. In our study, low dose of ondansetron (4mg) was used and the incidence of shivering was only 10% in the ondansetron group. The mean weight of patient was 76kg in Kelsaka study while in our study mean weight of patient was 52.80 kg. So obviously the dose requirement of ondansetron would be less in our group of population. Hence, 4mg of ondansetron showed almost same result in term of incidence of shivering.
Very few studies are available till date in relation to use of ketamine for prevention of shivering during general or regional anaesthesia probable because of its undesirable side effects like too much sedation ,hallucination and nausea and vomiting.
In our study, very low dose of ketamine (0.25mg kg-1) was used to minimize the side effect and we found that it was significantly effective and the shivering was observed only in 1 patient out of 40 (2.5%). Ketamine is competitive receptor antagonist of N- methyl-D-aspartic acid (NMDA) has a role in thermoregulation in various levels. Ketamine probably controls shivering by non- shivering thermo genesis either influencing the hypothalamus or by the beta adrenergic effect of nor epinephrine. Dal et al12 showed that ketamine 0.5mg kg-1was effective in prevention of post anaesthetic shivering in patients receiving general anaesthsia. Sagir et al9 showed that 0.5mg kg-1of ketamine was also effective in prevention of shivering during spinal anaesthesia. The shivering was not observed in any patients receiving ketamine. In our study, 0.25mg kg-1of ketamine was also as effective as 0.5mg kg-1of ketamine. The shivering was seen in only one patient.
In present study, when the effectiveness of ondansetron and ketamine was compared, ketamine was found to be more effective in prevention of shivering. The odds between ketamine and ondansetron is 1: 4.33 where p< 0.001.that is shivering rate is 4.33 times higher in ondansetron than in ketamine. The hypotensive episode was also found to be less in ketamine as compared to ondansetron and normal saline group. Only 4 patients out of 40 had hypotension requiring mephentermine IV. There were 9 cases of hypotension in ondansetron and 8 in normal saline group. Ketamine has sympathetic stimulation and vasoconstrictive effect which explains the less incidence of hypotension. In our study, most of the patients (38 out of 40) in ketamine group were sedated to grade 2 and only 2 patients were sedated to grade 3. Sedative effect was present for first 30 minutes of intraoperative period. This was obvious finding because ketamine in low dose has sedative effect but there was lesser grade of sedation with dose of 0.25 mg kg-1. Sagir et al9 used 0.5mg kg-1of ketamine and sedation grade was 3 in most patients. This mild sedation observed may be an advantage during surgery under spinal anaesthesia as it avoids the need of giving other sedative or anxiolytic drug like midazolam. The other significant finding of our study was that no hallucination was seen with 0.25mg kg-1 of ketamine which was observed in previous study with higher doses.
Few of the limitations of our study are that we did not include a positive control group using an established agent such as meperidine. Precisely because meperidine's dose and efficacy are already established and also the grade 1and 2 shivering during was ignored. Only grade 3 shivering was taken as significant.
In conclusion, the findings of our study suggest that the prophylactic administration of low dose ketamine (0.25 mg kg-1) and ondansetron (4mg) produces significant antishivering effect in comparison to placebo, in patients undergoing spinal anaesthesia without any significant side effects. Ketamine (0.25 mg kg-1) is significantly more effective than ondansetron(4mg) during spinal anaesthesia.
Authors disclosure: There is no conflict of interest financial ties involved.
REFERENCES
- 1.Sellden E, Lindahl S. Aminoacid-induced thermogenesis reduces hypothermia during anaesthesia and shortens hospital stay. Anesth analg. 1999;89:1551–6. doi: 10.1097/00000539-199912000-00045. [DOI] [PubMed] [Google Scholar]
- 2.Berti M, Fanelli G, Casati A, et al. Hypothermia prevention and treatment. Anaesthesia. 1998;53(Suppl.2):46–7. doi: 10.1111/j.1365-2044.1998.tb15151.x. [DOI] [PubMed] [Google Scholar]
- 3.Joris J, Ozaki N, Sessler D, et al. Epidural anesthesia impairs both central and peripheral thermoregulatory control during general anesthesia. Anesthesiology. 1994;80:268–77. doi: 10.1097/00000542-199402000-00006. [DOI] [PubMed] [Google Scholar]
- 4.Frank SM, El-Rahmany HK, Cattaneo CG, Barns RA. Predictors of hypothermia during spinal anesthesia. Anesthesiology. 2000;92:1330–4. doi: 10.1097/00000542-200005000-00022. [DOI] [PubMed] [Google Scholar]
- 5.Bhattacharya PK, Bhattacharya L, Jain RK, Agrarwal RC. Post anaesthesia shivering (PAS): A review. Indian J Anaesth. 2003;47(2):88–93. [Google Scholar]
- 6.Dal D, Kose A, Honca M, Akinci B, Basgul E, Aypar U. Efficacy of prophylactic ketamine in preventing postoperative shivering. Br J Anaesth. 2005;95:189–192. doi: 10.1093/bja/aei148. [DOI] [PubMed] [Google Scholar]
- 7.Cattaneo CG, Frank SM, Hesel TW, et al. The accuracy and precision of body temperature monitoring methods during regional and general anesthesia. Anesth Analg. 2000;90:938–45. doi: 10.1097/00000539-200004000-00030. [DOI] [PubMed] [Google Scholar]
- 8.Tsai YC, Chu KS. A comparison of tramadol, amitriptyline, and meperidine for postepidural anesthetic shivering in parturients. Anesth Analg. 2001;93:1288–92. doi: 10.1097/00000539-200111000-00052. [DOI] [PubMed] [Google Scholar]
- 9.Sagir O, Gulhas N, Toprak H, Yucel A, Begec Z, Ersoy O. Control of shivering during regional anaesthesia: prophylactic ketamine and granisetron. Acta Anaesthesiol Scand. 2007;51:44–49. doi: 10.1111/j.1399-6576.2006.01196.x. [DOI] [PubMed] [Google Scholar]
- 10.Kelsaka E, Sibel B, Deniz K, Binnur S. Comparison of ondansetron and meperidine for prevention of shivering in patients undergoing spinal anesthesia. Reg Anesth Pain Med. 2006;31:40–45. doi: 10.1016/j.rapm.2005.10.010. [DOI] [PubMed] [Google Scholar]
- 11.Bilotta F, Pietropaoli P, Sanita R, Liberatori G, Rosa G. Nefopam and Tramadol for the prevention of shivering during Neuraxial anesthesia. Reg Anesth Pain Med. 2002;27:380–84. doi: 10.1053/rapm.2002.33563. [DOI] [PubMed] [Google Scholar]
- 12.Dal D, Kose A, Honca M, Akinci SB, Basgul E, Aypar U. Efficacy of prophylactic ketamine in preventing postoperative shivering. Br J Anaesth. 2005;95:189–92. doi: 10.1093/bja/aei148. [DOI] [PubMed] [Google Scholar]