

Abstract
Background:
Palmoplantar psoriasis is a frequently encountered variant of psoriasis. It is difficult to treat and even more difficult to maintain remission as it is exacerbated by friction and trauma of the patient's daily activities. Existing topical modalities of treatment are often inadequate and show unpredictable response.
Aim:
To study the efficacy and safety of a newer retinoid, tazarotene, as 0.1% cream in the treatment of palmoplantar psoriasis.
Materials and Methods:
Thirty adult patients with palmo-plantar psoriasis were randomized to therapy with once daily application of topical tazarotene cream (0.1%) or once daily application of clobetasol propionate cream (0.05%) for 12 weeks. The patients were assessed every 2 weeks for improvement in Erythema, Scaling, Fissures and Induration (ESFI) score and Physicians Global Assessment Scale.
Results:
At 12 weeks, the tazarotene group showed mean ESFI reduction to 1.12 (83.2%) from 6.65 at baseline. Complete clearance was noted in 52.9% of the patients. Clobetasol propionate group showed mean ESFI reduction to 0.62 (89.1%) from 5.69 at baseline, with complete clearance in 61.5% of the patients. Differences between the two groups were statistically insignificant. Side effects observed were initial irritation (41%) in the tazarotene group and hypopigmentation (53.8%) in the steroid-treated patients.
Conclusion:
Tazarotene is as effective as clobetasol propionate and provides a good alternative for the treatment of palmo-plantar psoriasis where hypopigmentation limits the use of clobetasol propionate cream.
Keywords: Psoriasis, palmoplantar psoriasis, tazarotene
Introduction
Palmoplantar psoriasis is a chronic relapsing variant of psoriasis. The patient suffers not only physically but also psychologically as it interferes with day to day activities, and deleteriously impacts the quality of life. Different treatment options are available such as potent topical steroids, phototherapy, topical tar or anthralin, topical retinoids and systemic modalities like methotrexate. However, they all have limitations in terms of efficacy or side effect profile.
Clobetasol propionate cream is a superpotent steroid, which is one of the modalities of treatment for this disease in India. But its long-term usage causes atrophy, thinning of skin, telangiectasias and tachyphylaxis. Tazarotene, a newer retinoid, is devoid of all the side effects caused by clobetasol propionate. It also has the potential to reduce the degree of skin atrophy associated with topical corticosteroids.[1] Efficacy of tazarotene cream (0.1%) has been earlier compared with that of moderately potent steroids such as mometasone furoate in chronic plaque psoriasis.[2]
However, there have been no comparative studies of tazarotene cream with highly potent steroids like clobetasol propionate, specifically in palmoplantar psoriasis to date.[3]
The aim of this study is to study the efficacy and safety of tazarotene cream (0.1%) in the treatment of palmoplantar psoriasis and to compare the same with the standard therapy using clobetasol propionate cream (0.05%).
Materials and Methods
Patients above 18 years of age, diagnosed to have palmoplantar psoriasis on clinical features and skin biopsy, were included. Patients on topical medications for 4 weeks prior to screening visit, those with palmoplantar pustulosis, requiring systemic drugs, pregnant and lactating women were excluded.
Thirty patients were enrolled in the study after detailed consent procedure and randomized to therapy with once daily application of topical tazarotene cream (0.1%) or once daily application of clobetasol propionate cream (0.05%). Study patients were instructed to apply a thin layer of cream once daily at night to the affected area and standard emollient (white soft paraffin) in the morning daily for 12 weeks. The patients were assessed by a blinded observer every 2 weeks during the study period.
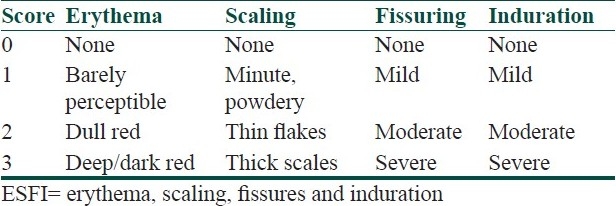
The primary effect of the drug was evaluated by an improvement in ESFI (Erythema, Scaling, Fissures and Induration) score at 2 week intervals up to 12 weeks, as given in Table 1.[4]
Table 1.
ESFI score
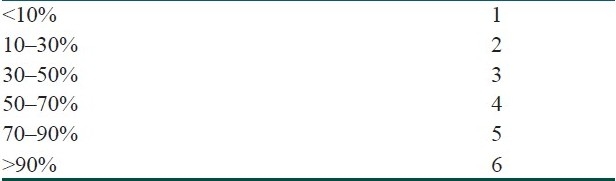
The secondary efficacy was evaluated by percentage reduction in palmoplantar area [Table 2] involvement at 2 weekly intervals.
Table 2.
Percentage reduction in in area involvement
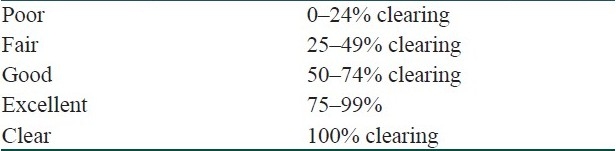
The investigator assessed the response to treatment by means of Physicians global assessment scale (PGAS) as in Table 3.
Table 3.
Physicians Global Assessment Scale (PGAS)
All adverse events were documented. Statistical analysis was performed using student's “t” test for independent variables and paired “t” test to evaluate the efficacy of the drug.
Results
A total of 30 patients were randomized and completed 12 weeks of treatment. Of these, 17 received tazarotene cream and 13 received clobetasol propionate cream. The mean age of tazarotene group was 35.82 years and that of clobetasol group was 40.38 years. The mean duration of disease was 29.53 months in tazarotene group and 28.38 months in clobetasol group. The demographic differences were statistically insignificant.
At baseline visit, mean ESFI score of tazarotene group was 6.65 and mean area affected was 2.65 [Tables 4 and 5]. PGAS was calculated from the first visit in comparison to baseline [Table 6]. At 12 weeks, mean ESFI score reduced to 1.12 and the mean area reduced to 0.94. Reduction in ESFI, area score and PGAS was noted gradually and consistently every 2 weeks during the study period. At end of study, 52.9% showed complete clearance (100% improvement), 17.6% showed excellent response (75–99% improvement), 23.5% showed good response (50–74% improvement) and 5.9% showed less than 50% improvement. Itching and irritation was complained by six patients (35.3%) and four patients (23.5%) at 2 and 4 weeks, respectively. It resolved with continued usage and no side effects were complained by any patient receiving tazarotene from 6th week onward. No patients developed any other side effects like increased erythema or fissuring with use of tazarotene [Table 7].
Table 4.
ESFI score
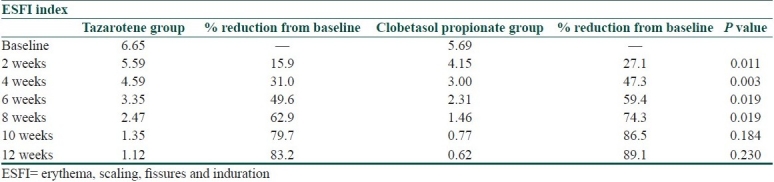
Table 5.
Mean area involvement
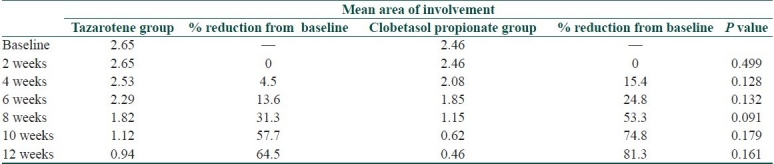
Table 6.
Physicians global assessment scale
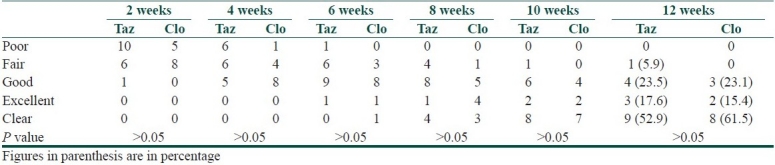
Table 7.
Side effects of tazarotene cream

At baseline visit, mean ESFI score of clobetasol group was 5.69 and mean area was 2.46 [Tables 4 and 5]. At 12 weeks, mean ESFI score reduced to 0.62 and the mean area reduced to 0.46. The scores showed a sharp decrease at 2, 4, 6 and 8 weeks, and then gradually stabilized at 10 and 12 weeks. At the end of study, 61.5% showed complete clearance (100% improvement), 15.4% showed excellent response (75–99% improvement) and 23.1% showed good response (50–74% improvement). Hypopigmentation developed in one of the patients as early as 4 weeks; 53.8% developed hypopigmentation as side effect at the end of the study. No other side effects like atrophy or telengiectasias were noted [Table 8].
Table 8.
Side effects of clobetasol propionate cream

The difference in ESFI in clobetasol group at 2, 4, 6 and 8 weeks was statistically significant compared to tazarotene group. The reduction in ESFI at 10 and 12 weeks in both the groups showed no statistically significant difference. At the end of study (12 weeks), tazarotene group showed 83.2% reduction while clobetasol group showed 89.1% reduction from the baseline mean ESFI score. Results of our study therefore showed that clobetasol acts faster with more rapid response in the first 8 weeks; however, at 12 weeks, both tazarotene and clobetasol appeared to be equally efficacious. Tazarotene application causes initial irritation which subsides within 2–4 weeks, while clobetasol application may result in hypopigmentation as early as 4 weeks [Tables 7 and 8].
With reference to individual parameters, we noted that there was complete subsidence of erythema in all patients receiving clobetasol propionate at 10 weeks (P = 0.01). Clobetasol propionate caused faster resolution of scaling in the initial phase, but at 12 weeks, resolution of scaling in both the groups was statistically insignificant. The steroid cream also led to significant reduction of fissuring at 2 and 4 weeks with complete resolution at 6 weeks (P = 0.006), whereas tazarotene caused resolution of fissuring at 10 weeks. Reduction in induration was seen to be equivalent in both the groups.
Discussion
The decline in ESFI scores and marked improvement in involved surface area supports the conclusion that tazarotene is as efficacious in the treatment of patients with palmoplantar psoriasis as the standard therapy with topical superpotent steroid. No controlled data are available till date comparing topical tazarotene and clobetasol propionate cream in palmoplantar psoriasis.
Angelo et al.[3] compared the effect of tazarotene cream versus clobetasol propionate cream in chronic plaque psoriasis in a left-right randomized double blind controlled study. In this study, clobetasol cream produced higher success rates as compared to tazarotene cream over a 12-week treatment period. The treatment success rates were 100 and 88% for clobetasol propionate cream and tazarotene cream, respectively. In our study, the treatment success rate (>50% ESFI improvement) was 100 and 94.1% for clobetasol propionate cream and tazarotene cream, respectively.
In the study by Angelo et al., adverse effects were seen in 7 patients (19.4%) with tazarotene and 10 patients (27.8%) with clobetasol. The common side effect was local irritation in six patients (16.7%) treated with tazarotene. Irritation was mild except in two patients. With clobetasol, the common side effect was hypopigmentation which was seen in seven patients (19.4%). Skin atrophy was seen in three patients (8.3%) treated with clobetasol. In our study, six patients (23.5%) receiving tazarotene experienced increased itching at 2 weeks which subsided with continued treatment. None of this group developed serious irritation or increase in fissuring. Seven patients (53.8) receiving clobetasol propionate developed hypopigmentation; however, no atrophy was noted.
So far, the efficacy of tazarotene has been compared with moderately potent steroids like mometasone furoate. It has been shown that efficacy of tazarotene plus moderate potent steroid like mometasone furoate is greater than tazarotene monotherapy.[2] Treatment of stable plaque psoriasis with tazarotene 0.1% gel plus mometasone furoate 0.1% cream promotes greater and more rapid efficacy, and a more prolonged therapeutic benefit after treatment than twice-daily treatment with mometasone furoate 0.1% cream alone. Also, studies have shown that use of tazarotene along with superpotent steroid application helps in gradual weaning of the steroid and maintaining remission with application of tazarotene cream three to five times a week.[1] Tazarotene has an anti atrophogenic effect when used along with superpotent steroids.[1] Tazarotene has also been combined with various other modalities like NB UVB phototherapy, PUVA therapy and compared with topical calcipotriol in various studies, with results showing greater efficacy with combination treatment.[5–7]
Conclusion
Tazarotene is efficacious and well tolerated in the treatment of palmoplantar psoriasis. However, clobetasol propionate has a faster onset of action than tazarotene. Tazarotene is a good alternative drug for the treatment of palmoplantar psoriasis where hypopigmentation limits the prolonged use of clobetasol propionate. Palmoplantar psoriasis should respond well to a combination therapy with both, withdrawing clobetasol propionate after the initial phase and continuing tazarotene till remission.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil.
References
- 1.Lebwohl M. Strategies to optimize efficacy, duration of remission, and safety in the treatment of plaque psoriasis by using tazarotene in combination with a corticosteroid. J Am Acad Dermatol. 2000;43:S43–6. doi: 10.1067/mjd.2000.108319. [DOI] [PubMed] [Google Scholar]
- 2.Koo JY, Martin D. Investigator-masked comparison of tazarotene gel q.d. plus mometasone furoate cream q.d. vs. mometasone furoate cream b.i.d. in the treatment of plaque psoriasis. Int J Dermatol. 2000;40:210–2. doi: 10.1046/j.1365-4362.2001.01167.x. [DOI] [PubMed] [Google Scholar]
- 3.Angelo JS, Kar BR, Thomas J. Comparison of clinical efficacy of topical tazarotene 0.1% cream with topical clobetasol propionate 0.05% cream in chronic plaque psoriasis: A doubleblind, randomized, right-left comparison study. Indian J Dermatol Venereol Leprol. 2007;73:65. doi: 10.4103/0378-6323.30663. [DOI] [PubMed] [Google Scholar]
- 4.Kumar B, Sandhu K, Kaur I. Topical 0.25% methotrexate gel in a hydrogel base for palmoplantar psoriasis. J Dermatol. 2004;31:798–801. doi: 10.1111/j.1346-8138.2004.tb00602.x. [DOI] [PubMed] [Google Scholar]
- 5.Behrens S, Kollmann MG, Schiener R, Peter RU, Kerscher M. Combination phototherapy of psoriasis with narrow-band UVB irradiation and topical tazarotene gel. J Am Acad Dermatol. 2000;42:493–5. doi: 10.1016/s0190-9622(00)90225-1. [DOI] [PubMed] [Google Scholar]
- 6.Lowe NJ. Optimising therapy: tazarotene in combination with phototherapy. Br J Dermatol. 1999;140 S54:8–11. doi: 10.1046/j.1365-2133.1999.140s54008.x. [DOI] [PubMed] [Google Scholar]
- 7.Schiener R, Williams SCB, Pillekamp H, Kaskel P, Peter RU, Kerscher M. Calcipotriol versus tazarotene as combination therapy with narrow band ultraviolet B(311nm): efficacy in patients with severe psoriasis. Br J Dermatol. 2000;143:1275–8. doi: 10.1046/j.1365-2133.2000.03900.x. [DOI] [PubMed] [Google Scholar]