

Description
We describe a case of three middle-aged women with acute-onset low back pain. Clinical examination was not contributory. Plain radiographs of the pelvis were normal in two patients (figures 1 and 2) and showed signs of sacroiliitis in one patient (figure 3). Subsequently, we performed MRI, which revealed unilateral insufficiency fractures of the sacrum in all patients (figures 4–6).
Figure 1.

Plain radiograph of patient 1.
Figure 2.

Plain radiograph of patient 2.
Figure 3.

Plain radiograph of patient 3 showing signs of sacroiliitis on the right site.
Figure 4.
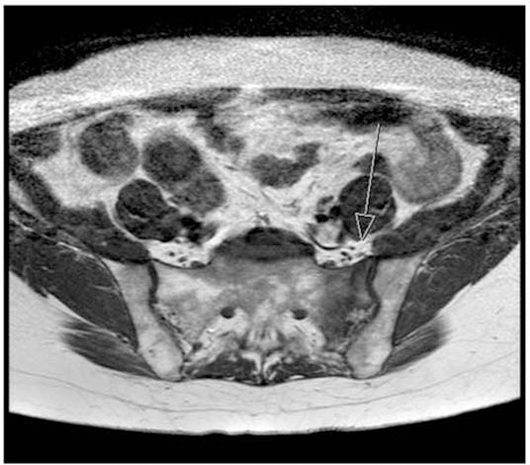
MRI image of patient 1 showing an unilateral (left) insufficiency fracture of the sacrum.
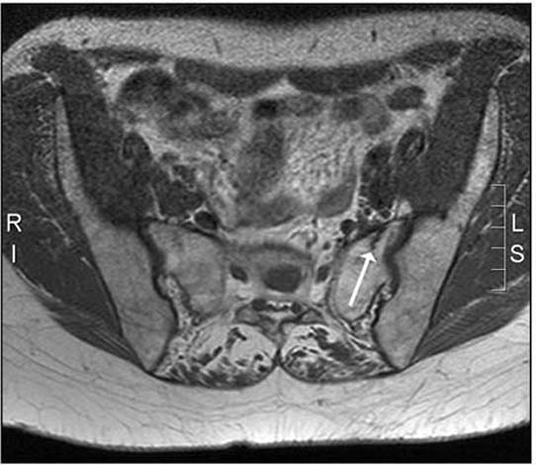
Figure 6.
MRI image of patient 3 showing an unilateral (right) insufficiency fracture of the sacrum.
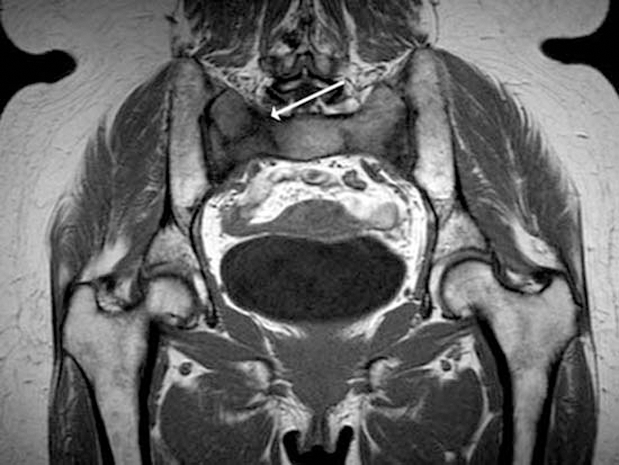
Figure 5.
MRI image of patient 2 showing an unilateral (left) insufficiency fracture of the sacrum.
Insufficiency fractures of the sacrum occur when normal stresses are placed on bones with reduced mineral content and elastic resistance.1 Most fractures occur in older patients, especially women. Predisposing factors include osteoporosis, rheumatoid arthritis, prolonged glucocorticoid treatment, pelvic radiotherapy and metabolic bone diseases. Clinical presentation is not specific and highly variable.1 2
Plain radiographs are usually not diagnostic because sacral lesions are often obscured by bowel gas.2 3 Bone scintigraphy is a sensitive technique, but the classical H-sign, consisting of fractures of both the sacral ala and a horizontal fracture of the sacral body, is present in only 32% of scintigraphies.3 Because of various incomplete patterns, it is difficult to distinguish fractures from sacroiliitis, osteomyelitis or metastatic bone disease. MRI is sensitive to changes in signal from bone marrow oedema that results from sacral fractures.1 2 These changes in signal are, however, not specific and the lesions can be misinterpreted as metastatic disease.2 3 CT may be helpful in confirming the diagnosis and can exclude inflammatory and malignant processes.2 3 In our three patients, diagnosis could be made by MRI.
Footnotes
Competing interests None.
Patient consent Obtained.
References
- 1.Tsiridis E, Upadhyay N, Giannoudis PV. Sacral insufficiency fractures: current concepts of management. Osteoporos Int 2006;17:1716–25 [DOI] [PubMed] [Google Scholar]
- 2.Blake SP, Connors AM. Sacral insufficiency fracture. Br J Radiol 2004;77:891–6 [DOI] [PubMed] [Google Scholar]
- 3.Schindler OS, Watura R, Cobby M. Sacral insufficiency fractures. J Orthop Surg (Hong Kong) 2007;15:339–46 [DOI] [PubMed] [Google Scholar]