

Abstract
Female reproductive tract (FRT) epithelial cells protect against potential pathogens and sexually transmitted infections. The purpose of this study was to determine if epithelial cells from the upper FRT secrete antimicrobials that inhibit reproductive tract pathogens which threaten women's health. Apical secretions from primary cultures of Fallopian tube, uterine, cervical and ectocervical epithelial cells were incubated with Neisseria gonorrhoeae, Candida albicans (yeast and hyphal forms), HIV-1, and Lactobacillus crispatus, prior to being tested for their ability to grow and/or infect target cells. Epithelial cell secretions from the upper FRT inhibit N. gonorrhoeae and both forms of Candida, as well as reduce HIV-1 (R5) infection of target cells. In contrast, none had an inhibitory effect on L. crispatus. Cytokines and chemokines analysis in uterine secretions revealed several molecules that could account for pathogen inhibition. These findings provide definitive evidence for the critical role of epithelial cells in protecting the FRT from infections, without comprising the beneficial presence of L. crispatus, which is part of the normal vaginal microflora of humans.
Keywords: female reproductive tract, endogenous microbicides, antimicrobials, epithelial cells
Introduction
The mucosal immune system in the reproductive tract and at other mucosal surfaces is the first line of defense against pathogenic organisms 1. The female reproductive tract (FRT) has unique requirements for regulation of immune protection since it must deal with sexually-transmitted pathogens, allogeneic spermatozoa, and the immunologically distinct fetus 1,2. To meet these challenges, the FRT has evolved unique immune mechanisms to protect against potential pathogens without compromising fetal survival or maternal health. The task is formidable in that more than twenty pathogens are transmissible through sexual intercourse. Each year there are an estimated 340 million new cases of sexually transmitted infections (STI) from bacteria (group B streptococcus, Neisseria gonorrhoeae, Chlamydia trachomatis, Treponema pallidum), parasites (Trichomonas vaginalis), and viruses (Herpes Simplex, Human Papilloma, Human Immunodeficiency) 3. In addition, the yeast C. albicans is responsible for 85-90% of cases of vulvovaginal candidiasis, which will affect 75% of all women at least once during their lifetime, and others will suffer from recurrent infections 4. C. albicans is described as a commensal microbe in the vagina because of its presence in up to 20% of healthy, asymptomatic women4,5. The recognition that commensals and pathogens, including HIV, traverse the entire FRT is an essential prerequisite to identifying solutions to preventing and controlling the spread of FRT infections which compromise reproductive health and threaten the lives of women and children 6.
Epithelial cells are vital for protection against pathogens in the FRT 7,8. For example, in addition to providing a physical barrier, FRT epithelial cells possess intracellular and extracellular pathogen recognition receptors (TLR, NOD, RIG, MDA-5, etc) 9-11, secrete chemokines and cytokines that initiate, regulate and link innate and adaptive immune responses 12-14, present antigen to T cells 15,16, produce the polymeric immunoglobulin receptor for transporting mucosal IgA antibodies from tissues into luminal secretions 17,18 and produce intracellular and secreted anti-microbial factors that kill invading microbes 19-22. Among the epithelial cell secretions, molecules with known bactericidal effects are defensins, secretory leukocyte protease inhibitor (SLPI), lysozyme and numerous other small peptides (for review, see 23). Human β-defensins 1-4 (HBD1-4) and secretory leukocyte protease inhibitor (SLPI) are effective at killing Gram-positive and Gram-negative bacteria, fungi, and enveloped viruses, including the STIs N. gonorrhoeae, C. trachomatis, Herpes simplex virus-2, and HIV-1, as well as C. albicans 19,24-30. Other factors with antiviral activity, notably against HIV-1, are the chemokines CCL3/MIP-1α, CCL4/MIP-1β, CCL5/RANTES, and CXCL12/SDF-1α 31,32, which inhibit HIV-1 infection of target host cells by interfering with the ability of HIV-1 to bind co-receptors CCR5 and CXCR4 found on host cells. HBD-1 expression has been shown in situ 33 and in cultured epithelial cells 11,21. We showed that TLR3 stimulation of uterine epithelial cells induces the mRNA expression of the antimicrobial peptides HBD1 and HBD2 11. More recently, we demonstrated that human uterine and Fallopian tube epithelial cells produce MIP3α 34 and Trappin-2/Elafin 35, and that these recombinant peptides inhibit HIV infection in a dose-dependent manner. One reason that the endometrium maintains a predominantly sterile environment might be due to the secretion of antimicrobial factors such as defensins, MIP3α and SLPI.
In the lower FRT, commensal microorganisms such as Lactobacillus provide an acid environment and secrete anti-pathogenic factors called bacteriocins 36. Commensals are essential to maintaining healthy tissue; removal of commensals through oral intake of antibiotics can lead to pathogen invasion. Factors in FRT secretions that kill pathogens might also adversely affect commensals. Therefore, as a part of these studies, we tested the effect of FRT epithelial cell secretions on Lactobacillus as well as selected potential pathogens.
The purpose of this study was to determine if primary cultures of normal human epithelial cells from throughout the FRT constitutively secrete antimicrobials that inhibit a variety of types of pathogens (bacterium, virus) as well as two commensals. We demonstrate that epithelial cells secretions from Fallopian tube, uterus, endocervix and ectocervix inhibit the growth and/or infection by N. gonorrheae and HIV-1 as well as both the yeast and hyphae forms of C. albicans without affecting L. crispatus.
Results
Inhibition of Candida albicans (yeast and hyphal forms) Growth by Human FRT Epithelial Cell Secretions in Culture
We have found that human Fallopian tube, uterine and endocervical columnar epithelial cells, isolated from patients as cell sheets and cultured on cell inserts as previously described 12,37, attain high values of TER and are functionally polarized. Previously, we showed that apical secretions from uterine epithelial cells cultured in antibiotic- and serum-free media inhibit both Staphylococcus aureus and Escherichia coli replication 19. To determine if uterine apical secretions are capable of inhibiting Candida, yeast and hyphal forms were co-incubated with an aliquot of conditioned media derived from polarized primary uterine epithelial cells. Figure 1A shows that the apical secretions from these cells inhibited C. albicans CFU by more than 80%. In similar studies using endocervix epithelial cells as well as squamous ectocervical epithelial cells, inhibition of C. albicans was 70% or more with conditioned media from each of these preparations (Figure 1B). These data indicate that FRT epithelial cells secrete a soluble factor(s) that inhibits both the commensal and pathogenic forms of C. albicans.
Figure 1.
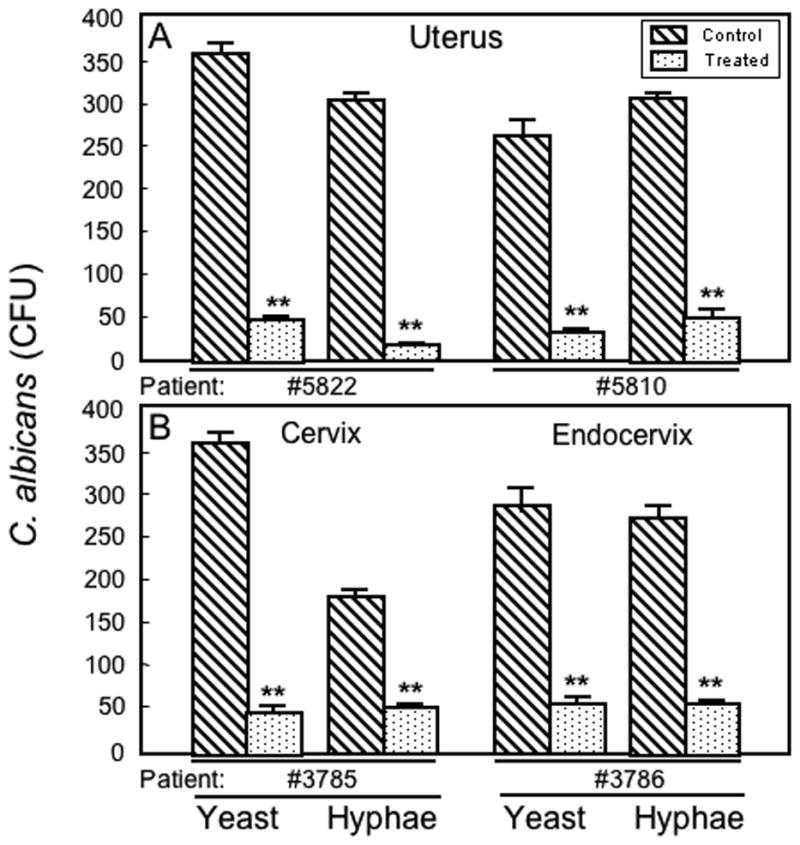
The effect of apical secretions from human primary FRT epithelial cells on growth of yeast and hyphal forms of Candida albicans. Conditioned media from (A) uterine and (B) cervix and ectocervix epithelial cells were diluted 1:1 with fresh media and incubated with either the yeast or hyphal forms of C. albicans for 1.5 hr before spreading the mixture on plates to enumerate colony forming units (CFU) after 24 or 48 hr incubation. Prior to collection of apical secretions or control media, cells were washed 3× and incubated for at least 72 hr in antibiotic- and serum-free media with 2 media changes to ensure elimination of antibiotic and serum. The effect of apical secretions on mean CFU ± SEM is shown. Control refers to media that had been incubated in cell inserts without cells, diluted 1:1 with fresh media, mixed with the appropriate form of C. albicans preparation and plated for CFU. Additional controls were C. albicans mixed directly with fresh media; there was no difference in CFU between either of these controls. Data presented in (A) and (B) are representative of individual tissues (uterus, cervix and ectocervix) from 4 patients (epithelial cells grown on 4-6 inserts per patient). **, P<0.01 compared to control.
Inhibition of Neisseria gonorrhoeae Growth by Human FRT Epithelial Cell Secretions in Culture
To define more fully the antimicrobial potential of epithelial cell secretions, uterine conditioned media were also incubated with N. gonorrhoeae. As shown in Figure 2A, uterine epithelial cell conditioned media inhibited N. gonorrhoeae growth by about 47% relative to controls incubated in media alone. Figure 2B illustrates that the conditioned media from Fallopian tube and endocervical cells also significantly inhibit N. gonorrhoeae.
Figure 2.
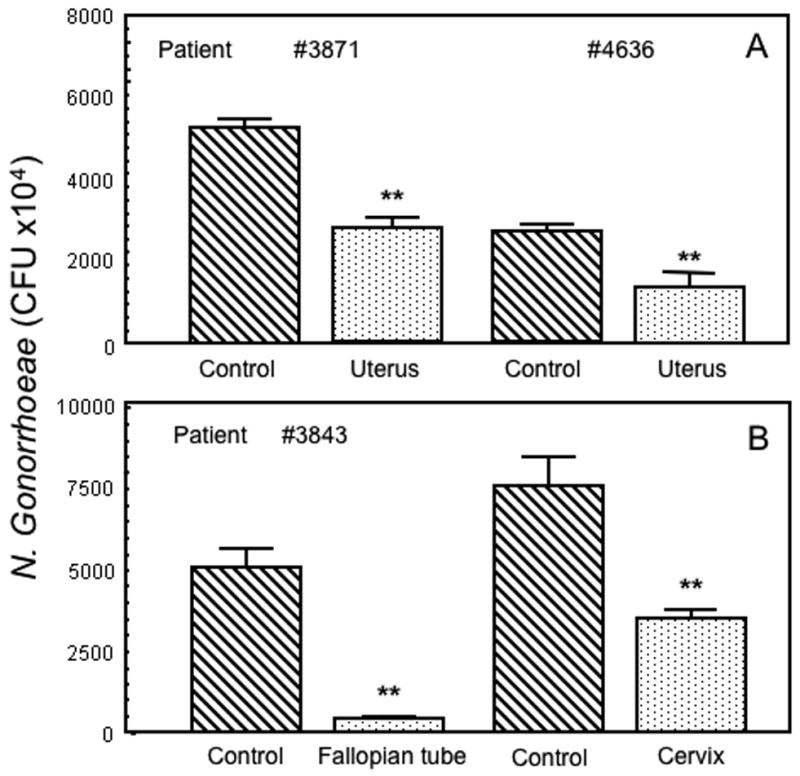
The effect of apical secretions from human primary FRT epithelial cells on growth of Neisseria gonorrheae. Conditioned media from (A) uterine and (B) Fallopian tube and endocervix epithelial cells were diluted 1:1 with fresh media and incubated with N. gonorrheae for 2 hr before spreading the mixture on plates to enumerate colony forming units (CFU) after 20 hr incubation. Prior to collection of apical secretions or control media, cells were washed 3× and incubated for at least 72 hr in antibiotic- and serum-free media with 2 media changes to ensure elimination of antibiotic and serum. The effect of apical secretions on mean CFU ± SEM is shown. Control refers to media that had been incubated in cell inserts without cells, diluted 1:1 with fresh media, mixed with the same N. gonorrheae preparation and plated for CFU. Additional controls were N. gonorrheae mixed directly with fresh media; there was no difference in CFU between either of these controls. Data presented in (A) and (B) are representative of individual tissues (uterus, Fallopian tubes, cervix and ectocervix) from 3-5 patients (4-6 inserts per patient). **, P<0.01 compared to control.
Inhibition of HIV-1 Infection by Secretions from Uterine, and Cervix Epithelial Cells in Culture
To explore the possibility that uterine epithelial cells in culture are capable of inhibiting HIV-1 infection, apical secretions from polarized uterine and cervical epithelial cells were diluted 10-fold and incubated with BaL, an R5/macrophage tropic HIV, respectively. As seen in Figure 3A, diluted uterine apical secretions from epithelial cells from the uteri of 2 patients significantly inhibited BaL (R5) infection of TZM-bl cells. Similarly as shown in Figure 3B, when secretions diluted 1:10 from polarized Fallopian tube and cervical epithelial cells as well as confluent ectocervical epithelial cells from the same patient were analyzed, apical secretions inhibited HIV-1 BaL (R5). Conditioned media had no effect on TZM-bl viability (data not shown). Overall these findings indicate the epithelial cells throughout the human FRT are capable of secreting molecules with anti-HIV activity.
Figure 3.
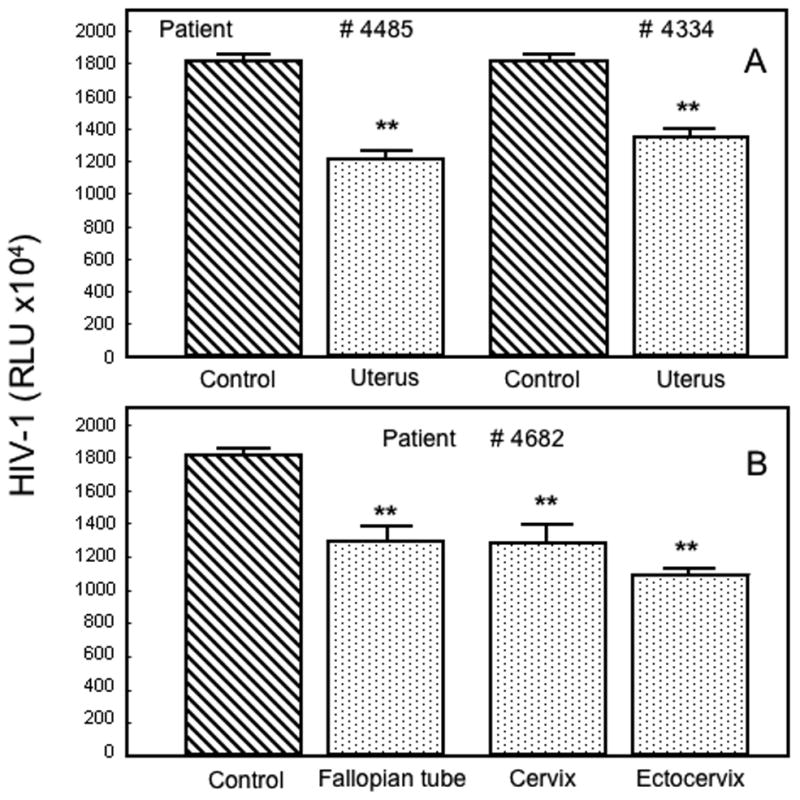
The effect of apical epithelial cell secretions on HIV-1 infection. Conditioned media (48 hr) from polarized (A) uterine and (B) Fallopian tube, cervical and ectocervical epithelial cells were diluted 1:10 with fresh media and incubated with BaL HIV-1 for 1 hr prior to addition to TZM-bl cells to assess infection as reported in Methods. Results are compared with infection data obtained with each virus incubated with media alone. Data presented in (A) and (B) are representative of individual tissues (uterus, Fallopian tubes, cervix and ectocervix) from 3 to 7 patients (4-6 inserts per patient). **, P<0.01 compared to control.
Lack of an Inhibitory Effect of FRT Epithelial Cell Secretions on the Commensal Lactobacillus crispatus
To determine if FRT epithelial cell conditioned media inhibited replication/viability of L. crispatus as they had for C. albicans and N. gonorrhoea (Figures 1 and 2), the L. crispatus was briefly incubated with various 48 hr secretions from FRT epithelial cells. A direct comparison of the same uterine epithelial cell secretion on CFU growth of C. albicans, N. gonorrhoeae and L. crispatus is shown in Figure 4. In contrast to the inhibition of C. albicans and N. gonorrhoeae, we found no evidence of inhibition by conditioned media of L. crispatus. As seen in Figure 5, when apical secretions from epithelial cells isolated from the Fallopian tubes, uterus, endocervix and ectocervix were analyzed, no differences in L. crispatus CFU between any of the secretions and the control were detected.
Figure 4.
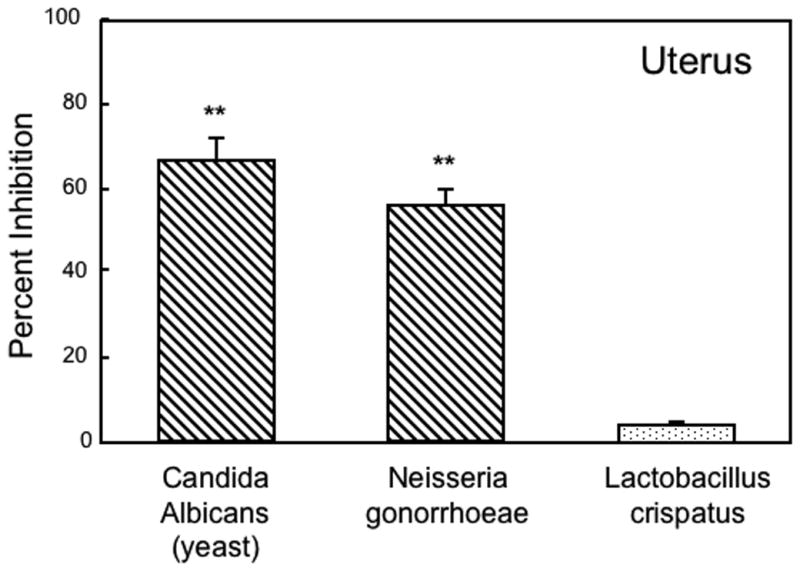
Comparison of anti-microbial activity against Neisseria gonorrhoeae, Candida albicans and Lactobacillus crispatus. Results shown are the percent inhibition obtained with uterine apical conditioned media derived from 4 cell inserts of one patient. For each microorganism, the CFU obtained with conditioned media incubation was compared with 4 controls of the microorganism incubated with media. **, P<0.01 compared to control.
Figure 5.
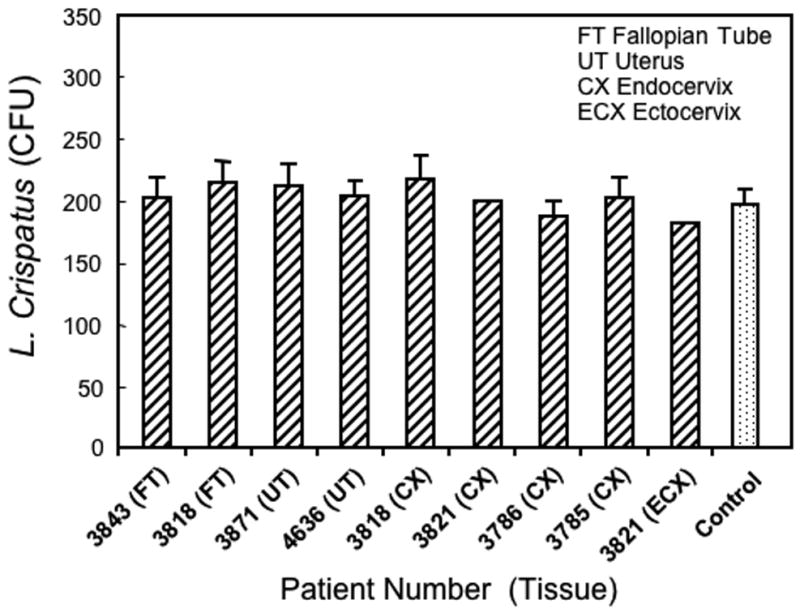
The effect of apical secretions from human primary FRT epithelial cells on growth of Lactobacillus crispatus. Conditioned media from Fallopian tube, uterine, endocervix and ectocervix epithelial cells were diluted 1:1 with fresh media and incubated with L. crispatus for 1 hr as noted in Methods before spreading the mixture on plates to enumerate colony forming units (CFU) after 48 hr incubation. Prior to collection of apical secretions or control media, cells were washed 3× and incubated for at least 72 hr in antibiotic- and serum-free media with 2 media changes to ensure elimination of antibiotic and serum. The effect of apical secretions on mean CFU ± SEM is shown. Control refers to media that had been incubated in cell inserts without cells, diluted 1:1 with fresh media, mixed with the same L. crispatus preparation and plated for CFU. Additional controls were L. crispatus mixed directly with fresh media; there was no difference in CFU between either of these controls. Data shown are the mean CFU +/- SEM from 3-4 cell inserts from epithelial cells (Fallopian tube: FT; uterine: UT; endocervix: CX; ectocervix: ECX) derived from a total of 7 designated patients.
Candidate Antimicrobials in Uterine Epithelial Cell Secretions
Primary uterine apical epithelial cell secretions were analyzed by ELISA and Luminex bead analysis to identify some of the candidate antimicrobial molecules. As seen in Table 1, a number of chemokines, which are often directly antimicrobial to bacteria, were found at concentrations capable of inhibiting microbes. In addition, several molecules that are known to inhibit HIV-1 infection were also present. For example, RANTES, SDF-1, SLPI, MIP3α, MIP1α, MIP1β, HBD2 and Trappin-2/Elafin have all been shown to block HIV-1 infection, either by binding to HIV co-receptors, direct inactivation of the virus or other mechanisms not yet defined. 34,35,38-40. These factors, also found at concentrations capable of inhibiting HIV-1, might act individually or in synergy to inactivate pathogens.
TABLE 1.
Constitutive Production of Cytokines, Chemokines and Antimicrobials in Apical Secretions from Polarized Uterine Epithelial Cells.
| Chemokine/Cytokine | pg/ml | SEM +/- | Number of Patients** |
|---|---|---|---|
|
| |||
| IL-8 (CXCL8) | 65,180 | 26,013 | 6 |
| IL-6 | 23,400 | 5,720 | 6 |
| SLPI | 18,920 | 1,050 | 3 |
| G-CSF | 15,100 | 4,210 | 6 |
| MCP-1 (CCL2) | 7,800 | 890 | 7 |
| RANTES | 5,197 | 128 | 3 |
| MEC (CCL28) | 5,100 | 397 | 3 |
| MIP-3α (CCL20) | 4,461 | 130 | 6 |
| SDF-1 (CXC12) | 4,237 | 248 | 3 |
| MIF | 2,928 | 292 | 10 |
| IP-10 (CXCL10) | 1,970 | 278 | 4 |
| GM-CSF | 860 | 126 | 6 |
| Trappin-2/Elafin | 420 | 56 | 4 |
| TNFα | 235 | 79 | 6 |
| HBD2 | 213 | 93 | 5 |
| MIP-1β (CCL4) | 130 | 13 | 6 |
| IL-17 | 60 | 18 | 6 |
Undectable (<15pg/ml): IL-1b, IL-2, IL-5, IL-10, IL-12p40, IL-12p70, IL-13.
Mean value from 4-6 inserts of 3-10 patients was used to calculate the Mean +/-SEM for each chemokine/cytokine.
Discussion
Mucosal surfaces are the first line of defense against potentially pathogenic microorganisms. Mucosal FRT epithelial cells have the capacity to recognize and respond immediately to pathogens and can rapidly block infection from being established. In a prior study 19, we demonstrated that human uterine epithelial cells in culture produce an anti-bacterial factor(s) that is equally effective in inhibiting the growth of a gram-positive (S. aureus) and a gram-negative bacterium (E. coli). To explore the possibility that secretions from epithelial cells along the entire FRT have antimicrobial activity, cultured epithelial cells from the Fallopian tubes, uterus, endocervix and ectocervix were grown to confluence in cell inserts, and assessed for their ability to secrete a substance(s) into the apical compartment that would inhibit bacterial and fungal growth, as well as HIV-1 infectivity. We found that epithelial cell conditioned media from all FRT sites examined inhibited growth of C. albicans (yeast and hyphae) and N. gonorrhoeae. In addition, FRT epithelial secretions were effective in significantly reducing HIV infection of TZM-bl cells. Just as important, FRT epithelial cell secretions had no effect on the growth of the urogenital commensal L. crispatus. Although vaginal squamous cells were not available owing to the hysterectomy specimens provided, squamous cells from ectocervical tissues were included in this study. As seen in Figures 1, 3 and 5, secretions from these cells had inhibitory activities comparable to that seen with columnar epithelial cells from the upper FRT.
It is well recognized that C. albicans is both a commensal as well as a pathogen in the lower female reproductive tract. As a part of its life cycle C. albicans exists in a nonpathogenic yeast form as well as a potential pathogen during the hyphal stage. Recognized as a common component of the digestive and genital floras, C. albicans has the potential to cause superficial as well as disseminated infections in response to host immune system changes, oral contraceptive use or microflora alterations 4,41. In contrast to the vagina, the upper FRT lacks C. albicans receptors and an appropriate nutritional status that most likely confer vaginal tissue tropism. Our studIes demonstrate that FRT epithelial cells secrete a spectrum of antimicrobials that have anti-C. albicans (yeast and hyphal forms) activity. An unexpected finding in our study was the differential effect of epithelial cell secretions on the commensal form of C. albicans (yeast) and Lactobacillus. Whereas all secretions tested inhibited the commensal form of C. albicans, none had an inhibitory effect on Lactobacillus. What is clear is that factors in epithelial secretions selectively discriminate between these two commensals.
Analysis of conditioned media led to the identification of a spectrum of antimicrobials, chemokines and cytokines secreted by uterine epithelial cells. We have analyzed the conditioned media for biological activity and identified MCP-1, IL-8, GM-CSF and SLPI based on either chemotaxis or antimicrobial assays 13,19,42. Many of these innate immune factors are multi-functional in that they exhibit both chemokine and antimicrobial activity. For example, MIP3α is known to be chemotactic for immature dendritic cells, T cells and B cells 43,44. This chemokine was found to inhibit both gram negative and gram positive bacteria 45. Our recent studies extend these findings by demonstrating that MIP3α as well as Trappin-2/Elafin are potent antiviral molecules capable of blocking HIV-1 infection of target cells 34,35. The extent to which other molecules secreted by epithelial cells throughout the FRT have cytokine and chemokine activity, as well as potent anti-bacterial, anti-fungal and anti-viral activity, remains to be determined.
In other studies in which we identified rElafin and rCCL20/MIP3α as novel antimicrobials against HIV 34,35, we found that neutralization of recombinants was possible with complete reversal of anti-HIV-1 activity. However, using these same antibodies, we did not reverse the anti-HIV-1 activity in uterine apical secretions containing Elafin and MIP3α, present at concentrations that should be completely blocked. We and others have previously shown FRT secretions contain a family of antimicrobials, which have anti-HIV-1 activity 34,35. Since Elafin and MIP3α are two of the many molecules present in these secretions, neutralization would not be measurable as a separate entity.
To the best of our knowledge, this is the first study to demonstrate that epithelial cells from throughout the human FRT, under constitutive conditions, inhibit a wide range of organisms that both compromise women's reproductive health and are potentially life threatening. Others have shown that commensal microorganisms are constitutively present in the lower FRT as part of a genital tract ecosystem that prevents the establishment of infections by pathogens via a variety of mechanisms (adherence, pH, bacteriocins, etc.). Our studies suggest that a dynamic balance exists in the upper FRT between innate immune epithelial cell factors and commensals in maintaining a healthy homeostatic microenvironment in the lower FRT. Unlike antibiotics, which can kill commensal bacteria in the lower FRT and thereby lead to opportunistic infections, endogenous epithelial factors are constitutively produced to provide long-term protection against pathogens. The mechanism(s) by which Lactobacillus is resistant to endogenous antimicrobials remains elusive, and is further complicated by the recent discovery that Lactobacillus stimulates β-defensin secretion by enterocytes 46. Commensals and epithelial cells act separately as well as in conjunction to protect the FRT from infection. This symbiotic relationship is particularly appropriate when one considers that secretions from the upper tract flow to the lower tract, while lower tract secretions, as well as sperm, move into the upper tract 47.
What remains to be determined is how genital tract secretions exert their inhibitory effects on bacterial, fungal and viral pathogens. Antimicrobials in the defensin family have been shown to cause pore formation in bacterial cell walls resulting in death of the bacterium. RANTES blocks HIV-1 infection by binding to the HIV co-receptor CCR5, preventing viral attachment, while Trappin-2/Elafin and MIP3α inhibit HIV-1 infection by interacting with the virus 34,35. SLPI, which inhibits Candida 29,48, HIV 26,30,49,50 and bacteria 51, has multiple mechanisms to protect the FRT. For example, SLPI inhibits HIV-1 infection by binding to annexin-1 on the cell surface, and by inhibiting NFkB stimulation for immune activation that promotes HIV infection. CCL28 inhibits bacteria and Candida 52 and possibly HIV infection by binding to CCR3, which has been shown to be an alternative coreceptor for HIV-1 53. Regardless of mechanism, it is clear that epithelial cells secrete a spectrum of antimicrobials that are protective against microbial pathogens.
Recognizing that sexual transmission is almost exclusively initiated by HIV-1 variants with tropism for the CCR5 co-receptor (R5 viruses) 54, we tested epithelial secretions and found that Fallopian tube, uterine, cervix and ectocervix epithelial secretions inhibited BaL (R5) virus. To the best of our knowledge, this is the first demonstration that secretions from epithelial cells throughout the human female reproductive tract have anti-HIV activity. Further studies are needed to identify the antimicrobial(s) responsible for inhibition of HIV and whether the antimicrobials secreted are cell and site specific, or produced by epithelial cells independent of their anatomical location (upper vs. lower FRT). In other studies, we have recently found that cervical vaginal secretions from both HIV (-) women and HIV (+) women who are healthy and not on anti-retrovirals (ARV) have anti-HIV activity against R5 HIV-1 55. These findings suggest that antimicrobials produced by epithelial cells from throughout the reproductive tract play an important protective role in vivo against the transmission of HIV from men to women.
In conclusion, these studies demonstrate that normal female reproductive tract epithelial cells secrete a spectrum of antimicrobials in culture that have broad-spectrum activity against bacterial, fungal and viral pathogens. These results emphasize the central role of uterine epithelial cells in protecting the female reproductive tract from sexually transmitted diseases and opportunistic infections.
Methods
Source of FRT Tissues
FRT mucosal tissues were obtained immediately following surgery from women who had undergone hysterectomies at Dartmouth-Hitchcock Medical Center. Tissues used in this study were distal to the sites of pathology and were determined to be unaffected with disease upon inspection by a trained pathologist. Pathologists also determined the menstrual status, as well as the stage in the cycle of pre-menopausal patients by examining the endometrial glands for secretory changes. Written informed consent was obtained from patients prior to surgery. Approval to use tissues was previously obtained from the Committee for the Protection of Human Subjects, in accordance with the human experimentation guidelines of the US Department of Health and Human Services. For cell culture studies, 17 FRT tissues were obtained from 11 women (age range 28 to 77). This patient population is detailed in Table 2. Of those patients included in the study, 2 had a post-operative diagnosis of malignant FRT disease. Single 0.75 to 3 gm samples of tissue were dissected out from equivalent sites of the FRT, distal to any gross pathology.
TABLE 2.
Patient profile
| PATIENT # | AGE | MENSTRUAL STATUS | SURGERY | TISSUE |
|---|---|---|---|---|
| 3729 | 50 | N/A | Fibroids | EM |
| 3785 | 45 | N/A | Fibroids | CX, ECX |
| 3786 | 59 | Cystic atrophy | Prolapse | CX, ECX |
| 3818 | 49 | Inactive | Fibroids | FT, CX, ECX |
| 3821 | 50 | N/A | Pelvic mass | CX, ECX |
| 3843 | 77 | N/A | Endometrial CA | FT |
| 3871 | 46 | Secretory | Prolapse | EM |
| 4334 | 61 | Inactive | Adnexal mass | EM |
| 4485 | 66 | Inactive | PMP bleeding | EM |
| 4636 | 28 | Proliferative | Prolapse | EM |
| 4682 | 30 | Secretory | Endometrial CA | FT, CX, ECX |
| 5810 | 34 | N/A | Mennorrhagia | EM |
| 5822 | 48 | N/A | Fibroids | EM |
Isolation of FRT Epithelial Cells
Epithelial cells were isolated as previously described 12,37. Briefly, tissues were minced under sterile conditions into 1-2 mm fragments and subjected to enzymatic digestion using a “PHC” enzyme mixture that contained final concentrations of 3.4 mg/ml pancreatin (Invitrogen, Grand Island, NY), 0.1 mg/ml hyaluronidase (Worthington Biochemical Corporation, Freehold, NJ), 1.6 mg/ml collagenase (Worthington), and 2 mg/ml D-glucose, in 1× Hanks' Balanced Salt Solution (HBSS, Invitrogen). Enzymes were chosen to maximize digestion of the extracellular matrix while minimizing digestion of cell surface antigens. After incubating for 1 hr at 37°C, cells were dispersed through a 250 micron mesh screen, washed and resuspended in DMEM/F12 complete medium. Epithelial cell sheets were separated from stromal cells by serial filtration through 40 and 20 micron nylon mesh filters (Small Parts Inc., Miami Lakes, FL). Epithelial sheets were collected, centrifuged at 500 ×g, and resuspended in complete medium supplemented with 20 mM HEPES, 2 mM L-glutamine (both from Life Technologies), Primocin (50 μg/ml, Invivogen, San Diego, CA) and 10% heat-inactivated defined fetal bovine serum (Hyclone, Logan, UT). Using this procedure, we have isolated epithelial cells that stain positive with antibodies for the epithelial antigens Ber-EP4 and cytokeratin and negative for CD4, CD45 and vimentin (Calbiochem, San Diego). The antibody studies and the attainment of high transepithelial resistance (TER) for cells derived from the upper reproductive tract indicate that cultures contain purified epithelial cells. Ectocervical epithelial cells, which do not develop TER, were also isolated in this manner and grown out to confluence on the cell inserts.
Cell Culture
To establish cell cultures of polarized human Fallopian tube, uterine and endocervical (cervix) epithelial cells with both apical and basolateral compartments, cells were cultured on Human Extracellular Matrix (BD Biosciences, San Jose, CA) coated Falcon cell culture inserts (Fisher Scientific, Pittsburgh, PA). Apical and basolateral compartments had 300 and 850 μl of complete medium, respectively. As an indicator of tight junction formation in upper FRT epithelial cell monolayers, transepithelial resistance (TER) was assessed daily using an EVOM electrode and Voltohmmeter (World Precision Instruments, Inc., Sarasota, FL), as described previously 12,37. Once high TER (700-2000 ohms/well) for upper tract epithelial cells or confluence for squamous ectocervical epithelial cells was attained, cells were washed and incubated for at least 4 days in serum- and antibiotic-free media with media changes every 48 hrs. Removal of serum, which might contain complement and pathogen-specific antibodies, and antibiotics was essential for measuring microorganism growth. Following media changes, cells were cultured in fresh serum- and antibiotic-free media for an additional 48 hr, prior to collection of conditioned media from apical and basolateral chambers. Conditioned medium was centrifuged at 500 ×g for 5 min and frozen at -80°C until assayed.
Serial dilutions of conditioned media were carried out that ranged from 1:1 to 1:100. We found that dilutions of 1:1 had no effect on inhibiting Lactobacillus, 1:4 was the highest dilution that significantly inhibited Candida, 1:8 was the highest for N. Gonorrhea, and 1:10 the highest dilution for HIV. Because secretions from epithelial cells contain a number of antimicrobials, studies were carried at the same dilution (1:1) for Lactobacillus, Candida, and N. Gonorrhea to compare inhibition between FRT cells. Only HIV analysis was carried out at a 1:10 dilution at a time different from the Lactobacillus, Candida, and N. Gonorrhea studies.
Measurement of anti-HIV activity: TZM-bl assay for HIV-1 Infection
The TZM-bl indicator cell line is a HeLa cell derivative that expresses high levels of CD4 and CCR5 and CXCR4 56. TZM-bl cells were maintained in TZM media consisting of DMEM supplemented with 10% defined FBS, 2 mM L-glutamine, and 50 μg/ml Primocin. TZM-bl cells were seeded at 2 × 104 cells per well in a 96-well microtiter plate and allowed to adhere overnight at 37°C. Apical secretions from were diluted 1:10 and incubated with BaL (R5 tropic) (Provided by Dr. Phalguni Gupta, Univ. Pittsburgh, Pittsburgh, PA) at multiplicity of infection (MOI) of 1 for 1 hr at 37°C in a final volume of 100 μl. Following incubation, the media was aspirated from TZM-bl cells and the virus plus secretion mixture added to the cells along with 100 μl of TZM-bl media. Briefly, the supernatants were aspirated at 48 hrs, and the cells were lysed with a beta-Glo luciferase assay substrate (Promega, Madison, WI). Uninfected cells were used to determine background luminescence. All infectivity assays were performed in quadruplicate.
Analysis of Neisseria gonorrhoeae inhibition
N. gonorrhoeae (ATCC 31426) was streaked on a chocolate agar plate (Remel, Lenexa, KS) and incubated 18-20 hrs at 37°C in 5% CO2 in a humidified incubator. From this plate, a N. gonorrhoeae colony was inoculated into pre-warmed GC broth and incubated 4 hrs at 37°C, after which, absorbance at 600 nm was measured. Cultures were adjusted with sterile PBS to approximately 1×106 CFU/ml. Ten μl of culture were added to 100 μl media or FRT epithelial cell secretions serially diluted in sterile PBS. After 2 hrs at 37°C, suspensions were serially diluted in sterile PBS, plated to chocolate agar, and incubated overnight for 20 hrs. CFU were counted and percent inhibition calculated.
Assay for effect of secretions on yeast and hyphal Candida albicans growth
One colony of the clinical/virulent strain V9:0327:TK of C. albicans was used to inoculate synthetic dextrose minimal medium and incubated for 48 hr to reach stationary phase with shaking at 250 rpm. Cells were washed twice in sterile phosphate buffered saline (PBS) and suspended at a concentration of 2500 cells/ml based on hemacytometer counting. The washed yeast suspension (40 μl) was incubated for 1.5 hr with an equal volume of undiluted conditioned media from human epithelial cells in 0.5 ml microcentrifuge tubes at 30°C to test the effect on yeast growth. Contents were transferred to yeast peptone dextrose agar plates, spread over the surface using a sterile microbiological spreader and incubated overnight at 30°C. Colony forming units (CFU) were counted at 24 hrs. The assay was performed in triplicate. Conditions were similar for assessing the effect of conditioned media on hyphal growth except that cells were resuspended in M199 prewarmed at 37°C and the conditioned media was also prewarmed to 37°C. Growth in yeast or hyphal morphology was verified microscopically using controls at a concentration of 4×106 cells/ml at 30°C or 37°C, respectively.
Assay for measuring the effect of FRT secretions on Lactobacillus crispatus
Lactobacillus crispatus (ATCC 33197) was inoculated from a glycerol stock into 4 ml of Mann Rogosa Sharpe (MRS) broth and cultured overnight at 37°C under anaerobic conditions without supplemental CO2. The culture was centrifuged, and the bacterial pellet resuspended in 3 ml of PBS to an O.D.600=0.2. The bacteria were then serially diluted 10-fold to a final concentration of approximately 1 × 104 CFU/ml. Twenty μl of the bacterial suspension were added to an equal volume of culture supernatants from the FRT cells, or media controls. The mixture was incubated for 1 hr at 37°C. PBS (60 μl) was then added to each tube, and the bacteria plated immediately on MRS agar plates. The plates were incubated overnight at 37°C in an anaerobic chamber and the number of bacterial colonies enumerated. Data are expressed as the mean ± S.D. of bacterial colonies on replicate plates.
Analysis of antimicrobials in epithelial cell secretions
Epithelial cell secretions were assayed for 30 different antimicrobials, chemokines and cytokines by either ELISA (R&D, Minneapolis, MN and Peprotech, Rocky Hill, NJ) or Luminex bead analysis (BioRad, Hercules, CA), as previously described 12. A minimum of 4 cell inserts was used from each epithelial cell source.
Statistical analysis
A two-tailed paired t test or a one-way ANOVA with Bonferonni's post-test was performed using GraphPad InStat version 3.0a (GraphPad Software, San Diego, CA, USA). A p value of <0.05 was taken as indicative of statistical significance.
Acknowledgments
The authors thank Richard Rossoll, M.S., Dartmouth Medical School, Deena Ratner, B.S., University of Pittsburgh, for excellent technical assistance in the preparation of samples, cells and virus stocks. Additionally, the authors thank Vincent Memoli, M.D., Section Chief of Anatomical Pathology, for procuring tissues; other members of the Department of Pathology for inspecting and dissecting tissue specimens: Jorge Gonzalez, M.D., Alan Schned, M.D., Peter Seery, Shannon Schutz, Elizabeth Rizzo, Richard Merrill, Charles-Robert Moultry, Patricia Larkin, Aimee Larson, Jennifer Simonton and Dawn Maddaline; for clinical support and scheduling: Laura Wolfe, Linda Hallock, Kathleen Pilchman, Karen Carter, Kris Ramsey, Tamara Krivit, and Joanne Lavin; surgeons: Barry Smith, Joan Barthold, Jackson Beecham, John Currie, Leslie Demars, Paul Hanissian, John Ketterer, Benjamin Mahlab, Paul Manganiello, Misty Porter, Karen George, William Young, Kris Strohbehn, Roger Young, Stephen Andrews, and Eric Sailer; OR nurses: Jeanette Sawyer, Tracy Stokes, Fran Reinfrank, and Jaclyn Logan. This work was supported by AI51877 and AI071761 (awarded to Dr. Charles Wira) from NIH.
Footnotes
Disclosure: The authors declare no conflict of interest.
References
- 1.Wira CR, Fahey JV, Sentman CL, Pioli PA, Shen L. Innate and adaptive immunity in female genital tract: cellular responses and interactions. Immunol Rev. 2005;206:306–335. doi: 10.1111/j.0105-2896.2005.00287.x. [DOI] [PubMed] [Google Scholar]
- 2.Kutteh WH, Mestecky J, Wira CR. Mucosal immunity in the human female reproductive tract. In: Mestecky J, et al., editors. Mucosal Immunology. Academic Press; New York: 2005. pp. 1631–1647. [Google Scholar]
- 3.WHO. Global prevalence and incidence of selected curable sexually transmitted infections: Overviwew and estimates. Geneva, Switzerland: 2005. [Google Scholar]
- 4.Fidel PL., Jr History and update on host defense against vaginal candidiasis. Am J Reprod Immunol. 2007;57:2–12. doi: 10.1111/j.1600-0897.2006.00450.x. [DOI] [PubMed] [Google Scholar]
- 5.Marot-Leblond A, et al. Efficient diagnosis of vulvovaginal candidiasis by use of a new rapid immunochromatography test. J Clin Microbiol. 2009;47:3821–3825. doi: 10.1128/JCM.01168-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wira CR, Fahey JV. A new strategy to understand how HIV infects women: identification of a window of vulnerability during the menstrual cycle. Aids. 2008;22:1909–1917. doi: 10.1097/QAD.0b013e3283060ea4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wira CR, Fahey JV. The innate immune system: gatekeeper to the female reproductive tract. Immunology. 2004;111:13–15. doi: 10.1111/j.1365-2567.2003.01796.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wira CR, Grant-Tschudy KS, Crane-Godreau MA. Epithelial cells in the female reproductive tract: a central role as sentinels of immune protection. Am J Reprod Immunol. 2005;53:65–76. doi: 10.1111/j.1600-0897.2004.00248.x. [DOI] [PubMed] [Google Scholar]
- 9.Pioli PA, et al. Differential expression of Toll-like receptors 2 and 4 in tissues of the human female reproductive tract. Infect Immun. 2004;72:5799–5806. doi: 10.1128/IAI.72.10.5799-5806.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Schaefer TM, Desouza K, Fahey JV, Beagley KW, Wira CR. Toll-like receptor (TLR) expression and TLR-mediated cytokine/chemokine production by human uterine epithelial cells. Immunology. 2004;112:428–436. doi: 10.1111/j.1365-2567.2004.01898.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Schaefer TM, Fahey JV, Wright JA, Wira CR. Innate immunity in the human female reproductive tract: antiviral response of uterine epithelial cells to the TLR3 agonist poly(I:C) J Immunol. 2005;174:992–1002. doi: 10.4049/jimmunol.174.2.992. [DOI] [PubMed] [Google Scholar]
- 12.Fahey JV, Schaefer TM, Channon JY, Wira CR. Secretion of cytokines and chemokines by polarized human epithelial cells from the female reproductive tract. Hum Reprod. 2005;20:1439–1446. doi: 10.1093/humrep/deh806. [DOI] [PubMed] [Google Scholar]
- 13.Meter RA, Wira CR, Fahey JV. Secretion of monocyte chemotactic protein-1 by human uterine epithelium directs monocyte migration in culture. Fertil Steril. 2005;84:191–201. doi: 10.1016/j.fertnstert.2005.01.104. [DOI] [PubMed] [Google Scholar]
- 14.Schaefer TM, Fahey JV, Wright JA, Wira CR. Migration inhibitory factor secretion by polarized uterine epithelial cells is enhanced in response to the TLR3 agonist poly (I:C) Am J Reprod Immunol. 2005;54:193–202. doi: 10.1111/j.1600-0897.2005.00298.x. [DOI] [PubMed] [Google Scholar]
- 15.Fahey JV, Wallace PK, Johnson K, Guyre PM, Wira CR. Antigen presentation by human uterine epithelial cells to autologous T cells. Am J Reprod Immunol. 2006;55:1–11. doi: 10.1111/j.1600-0897.2005.00343.x. [DOI] [PubMed] [Google Scholar]
- 16.Wallace PK, et al. MHC class II expression and antigen presentation by human endometrial cells. J Steroid Biochem Mol Biol. 2001;76:203–211. doi: 10.1016/s0960-0760(00)00149-7. [DOI] [PubMed] [Google Scholar]
- 17.Fahey JV, Humphrey SL, Stern JE, Wira CR. Secretory component production by polarized epithelial cells from the human female reproductive tract. Immunol Invest. 1998;27:167–180. doi: 10.3109/08820139809089454. [DOI] [PubMed] [Google Scholar]
- 18.Wira C, Fahey J, Wallace P, Yeaman G. Effect of the menstrual cycle on immunological parameters in the human female reproductive tract. J Acquir Immune Defic Syndr. 2005;38(1):S34–36. doi: 10.1097/01.qai.0000167040.58181.d5. [DOI] [PubMed] [Google Scholar]
- 19.Fahey JV, Wira CR. Effect of menstrual status on antibacterial activity and secretory leukocyte protease inhibitor production by human uterine epithelial cells in culture. J Infect Dis. 2002;185:1606–1613. doi: 10.1086/340512. [DOI] [PubMed] [Google Scholar]
- 20.King AE, Critchley HO, Kelly RW. Presence of secretory leukocyte protease inhibitor in human endometrium and first trimester decidua suggests an antibacterial protective role. Mol Hum Reprod. 2000;6:191–196. doi: 10.1093/molehr/6.2.191. [DOI] [PubMed] [Google Scholar]
- 21.King AE, Fleming DC, Critchley HO, Kelly RW. Regulation of natural antibiotic expression by inflammatory mediators and mimics of infection in human endometrial epithelial cells. Mol Hum Reprod. 2002;8:341–349. doi: 10.1093/molehr/8.4.341. [DOI] [PubMed] [Google Scholar]
- 22.King AE, Fleming DC, Critchley HO, Kelly RW. Differential expression of the natural antimicrobials, beta-defensins 3 and 4, in human endometrium. J Reprod Immunol. 2003;59:1–16. doi: 10.1016/s0165-0378(02)00083-9. [DOI] [PubMed] [Google Scholar]
- 23.Ganz T, Lehrer RI. Defensins. Pharmacol Ther. 1995;66:191–205. doi: 10.1016/0163-7258(94)00076-f. [DOI] [PubMed] [Google Scholar]
- 24.Duits LA, et al. Rhinovirus increases human beta-defensin-2 and -3 mRNA expression in cultured bronchial epithelial cells. FEMS Immunol Med Microbiol. 2003;38:59–64. doi: 10.1016/S0928-8244(03)00106-8. [DOI] [PubMed] [Google Scholar]
- 25.Ganz T. Defensins: antimicrobial peptides of innate immunity. Nat Rev Immunol. 2003;3:710–720. doi: 10.1038/nri1180. [DOI] [PubMed] [Google Scholar]
- 26.Hocini H, et al. Secretory leukocyte protease inhibitor inhibits infection of monocytes and lymphocytes with human immunodeficiency virus type 1 but does not interfere with transcytosis of cell-associated virus across tight epithelial barriers. Clin Diagn Lab Immunol. 2000;7:515–518. doi: 10.1128/cdli.7.3.515-518.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Porter E, et al. Distinct defensin profiles in Neisseria gonorrhoeae and Chlamydia trachomatis urethritis reveal novel epithelial cell-neutrophil interactions. Infect Immun. 2005;73:4823–4833. doi: 10.1128/IAI.73.8.4823-4833.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Quinones-Mateu ME, et al. Human epithelial beta-defensins 2 and 3 inhibit HIV-1 replication. Aids. 2003;17:F39–48. doi: 10.1097/00002030-200311070-00001. [DOI] [PubMed] [Google Scholar]
- 29.Tomee JF, Hiemstra PS, Heinzel-Wieland R, Kauffman HF. Antileukoprotease: an endogenous protein in the innate mucosal defense against fungi. J Infect Dis. 1997;176:740–747. doi: 10.1086/514098. [DOI] [PubMed] [Google Scholar]
- 30.Wahl S, et al. Secretory leukocyte protease inhibitor (SLPI) in mucosal fluids inhibits HIV-1. Oral Dis. 1997;3(1):S64–69. doi: 10.1111/j.1601-0825.1997.tb00377.x. [DOI] [PubMed] [Google Scholar]
- 31.Bleul CC, et al. The lymphocyte chemoattractant SDF-1 is a ligand for LESTR/fusin and blocks HIV-1 entry. Nature. 1996;382:829–833. doi: 10.1038/382829a0. [DOI] [PubMed] [Google Scholar]
- 32.Cocchi F, et al. Identification of RANTES, MIP-1 alpha, and MIP-1 beta as the major HIV-suppressive factors produced by CD8+ T cells. Science. 1995;270:1811–1815. doi: 10.1126/science.270.5243.1811. [DOI] [PubMed] [Google Scholar]
- 33.Valore EV, et al. Human beta-defensin-1: an antimicrobial peptide of urogenital tissues. J Clin Invest. 1998;101:1633–1642. doi: 10.1172/JCI1861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Ghosh M, et al. CCL20/MIP3alpha is a novel anti-HIV-1 molecule of the human female reproductive tract. Am J Reprod Immunol. 2009;62:60–71. doi: 10.1111/j.1600-0897.2009.00713.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Ghosh M, et al. Trappin-2/Elafin: a novel innate anti-HIV-1 molecule of the human female reproductive tract. Immunology. 2009 doi: 10.1111/j.1365-2567.2009.03165.x. In Press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Martin R, et al. Characterization of indigenous vaginal lactobacilli from healthy women as probiotic candidates. Int Microbiol. 2008;11:261–266. doi: 10.2436/20.1501.01.70. [DOI] [PubMed] [Google Scholar]
- 37.Fahey JV, Kaushic C, Wira CR. Human uterine epithelial cells: Influence of culture conditions and stromal cells on epithelial cell transepithelial cell resistance. In: Gupta SK, editor. Reproductive Immunology. Narosa Publishing House; New Delhi: 1999. pp. 366–378. [Google Scholar]
- 38.Bingle CD, Vyakarnam A. Novel innate immune functions of the whey acidic protein family. Trends Immunol. 2008;29:444–453. doi: 10.1016/j.it.2008.07.001. [DOI] [PubMed] [Google Scholar]
- 39.Garzino-Demo A. Chemokines and defensins as HIV suppressive factors: an evolving story. Curr Pharm Des. 2007;13:163–172. doi: 10.2174/138161207779313696. [DOI] [PubMed] [Google Scholar]
- 40.Schols D. HIV co-receptors as targets for antiviral therapy. Curr Top Med Chem. 2004;4:883–893. doi: 10.2174/1568026043388501. [DOI] [PubMed] [Google Scholar]
- 41.Calderone R. Taxonomy and biology of Candida. In: Calderone R, editor. Candida and Candidiasis. ASM Press; Washington, DC: 2002. pp. 307–325. [Google Scholar]
- 42.Shen L, et al. Synergy between IL-8 and GM-CSF in reproductive tract epithelial cell secretions promotes enhanced neutrophil chemotaxis. Cell Immunol. 2004;230:23–32. doi: 10.1016/j.cellimm.2004.08.004. [DOI] [PubMed] [Google Scholar]
- 43.Thomachot MC, et al. Breast carcinoma cells promote the differentiation of CD34+ progenitors towards 2 different subpopulations of dendritic cells with CD1a(high)CD86(-)Langerin- and CD1a(+)CD86(+)Langerin+ phenotypes. Int J Cancer. 2004;110:710–720. doi: 10.1002/ijc.20146. [DOI] [PubMed] [Google Scholar]
- 44.Perez OD, Mitchell D, Nolan GP. Differential role of ICAM ligands in determination of human memory T cell differentiation. BMC Immunol. 2007;8:2. doi: 10.1186/1471-2172-8-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Crane-Godreau MA, Wira CR. Effects of estradiol on lipopolysaccharide and Pam3Cys stimulation of CCL20/macrophage inflammatory protein 3 alpha and tumor necrosis factor alpha production by uterine epithelial cells in culture. Infect Immun. 2005;73:4231–4237. doi: 10.1128/IAI.73.7.4231-4237.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Schlee M, et al. Probiotic lactobacilli and VSL#3 induce enterocyte beta-defensin 2. Clin Exp Immunol. 2008;151:528–535. doi: 10.1111/j.1365-2249.2007.03587.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Zervomanolakis I, et al. Physiology of upward transport in the human female genital tract. Ann N Y Acad Sci. 2007;1101:1–20. doi: 10.1196/annals.1389.032. [DOI] [PubMed] [Google Scholar]
- 48.Chattopadhyay A, et al. Salivary secretory leukocyte protease inhibitor and oral candidiasis in human immunodeficiency virus type 1-infected persons. Infect Immun. 2004;72:1956–1963. doi: 10.1128/IAI.72.4.1956-1963.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Py B, et al. The phospholipid scramblases 1 and 4 are cellular receptors for the secretory leukocyte protease inhibitor and interact with CD4 at the plasma membrane. PLoS One. 2009;4:e5006. doi: 10.1371/journal.pone.0005006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Shugars D. Endogenous mucosal antiviral factors of the oral cavity. J Infect Dis. 1999;179(3):S431–435. doi: 10.1086/314799. [DOI] [PubMed] [Google Scholar]
- 51.Hiemstra PS, et al. Antibacterial activity of antileukoprotease. Infection and Immunity. 1996;64:4520–4524. doi: 10.1128/iai.64.11.4520-4524.1996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Hieshima K, et al. CCL28 has dual roles in mucosal immunity as a chemokine with broad-spectrum antimicrobial activity. J Immunol. 2003;170:1452–1461. doi: 10.4049/jimmunol.170.3.1452. [DOI] [PubMed] [Google Scholar]
- 53.Aasa-Chapman MM, Seymour CR, Williams I, McKnight A. Novel envelope determinants for CCR3 use by human immunodeficiency virus. J Virol. 2006;80:10884–10889. doi: 10.1128/JVI.01030-06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Margolis L, Shattock R. Selective transmission of CCR5-utilizing HIV-1: the ‘gatekeeper’ problem resolved? Nat Rev Microbiol. 2006;4:312–317. doi: 10.1038/nrmicro1387. [DOI] [PubMed] [Google Scholar]
- 55.Ghosh M, et al. Anti-HIV activity in cervical-vaginal secretions from HIV-positive and -negative women correlate with innate antimicrobial levels with IgA and IgG antibodies. PLoS ONE. 2010;5(6):e11366. doi: 10.1371/journal.pone.0011366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Steele C, Fidel PL., Jr Cytokine and chemokine production by human oral and vaginal epithelial cells in response to Candida albicans. Infect Immun. 2002;70:577–583. doi: 10.1128/IAI.70.2.577-583.2002. [DOI] [PMC free article] [PubMed] [Google Scholar]