

Abstract
Background
Very few studies have investigated the ”real world” prospective, predictive value of behavioral instruments used in laboratory studies to test decision-making abilities or impulse control. The current study examines the degree to which two commonly used decision-making/impulse control measures prospectively predict (heavy) alcohol use in a sample of college students.
Methods
200 healthy young adults (50% female), performed the Iowa Gambling Task (IGT) and a StopSignal inhibition task in the second college year. At testing and at the end of the fourth college year, heavy alcohol use was assessed.
Results
Disadvantageous performance on the IGT was associated with higher scores on a heavy drinking measure and higher quantity/frequency of alcohol use two years past neurocognitive testing in male students even after controlling for prior drinking. These results were corrected for heavy drinking and alcohol use in the period before neurocognitive testing. Interactions with gender indicated that this general pattern held for male but not female students. Level of response inhibition was not associated with either of the alcohol use measures prospectively.
Conclusion
These findings indicate that a neurocognitive decision-making task is predictive of maladaptive alcohol use. Advantageous decision makers appear to show adaptive real life decision-making, changing their drinking habits to the changing challenges of early adulthood (e.g., finishing college), whereas disadvantageous decision-makers do not, and continue to drink heavily. These findings extend earlier findings of neurocognitive predictors of relapse in clinical substance dependent groups, to subclinical alcohol use and abuse.
Keywords: alcohol use, college students, decision-making, impulsivity, response inhibition
INTRODUCTION
Abstinent alcohol dependent persons display disadvantageous decision making compared to persons without substance dependence (Bechara et al., 2001). Diminished executive functions have been reported in persons with alcohol dependence (for a review, see Giancola & Moss, 1998). Heavy drinkers (i.e. 21 drinks or more per week) without alcohol dependence also display mild deficits on a variety of neurocognitive functions, such as attention, memory, and visuospatial abilities (for a review, see Parsons & Nixon, 1998). Recent neurobiological addiction theories include dysfunctions in cognitive and motivational neural circuitry as central elements in substance dependence (Goldstein & Volkow, 2002). The key cognitive functions related to this circuitry are distorted evaluation and appraisal of positive and negative consequences, functions which play a role in decision making (Krawczyk, 2002), and diminished control over behavior (diminished response inhibition).
Few studies have investigated whether neurocognitive tests of risky decision making and inhibition prospectively predict alcohol use. Recently, several neurocognitive and neuroimaging studies investigated the predictive value of neurocognitive tests for relapse in treatment seeking, substance dependent groups. Some of these studies incorporated self-report measures as well, and found that neurocognitive and brain imaging data predicted unique variance in relapse above and beyond that accounted for by self-report measures. Two pilot studies point to the predictive value of disadvantageous decision making for relapse in alcohol dependent patients and pathological gamblers, respectively (Goudriaan et al., 2008; Bowden-Jones et al., 2005). One of these studies reported predictive value for neurocognitive tests, but no predictive role for self-report measures (Goudriaan et al., 2008), whereas the other study found that both neurocognitive and personality measures were predictors of relapse (Bowden-Jones et al., 2005). Neurocognitive measures of delay discounting and behavioural inhibition predicted non-abstinence in a smoking cessation research study in adolescent smokers (Krishnan-Sarin et al., 2007). A neuroimaging study in a group of methamphetamine dependent patients indicated that neural activation patterns during a simple decision-making task correctly predicted relapse or non-relapse in 92% of the patients included (Paulus, Tapert, & Schuckit, 2005). Thus, evidence is accumulating that neurocognitive measures account for unique variance, over and above self-report measures in predicting drug use in clinical samples.
Notably, findings regarding the relationship between impulsivity (as measured by self-report questionnaires), behavioural inhibition (as measured by stop signal tasks or other behavioural inhibition tasks) and IGT performance have been mixed. One study indicated only a relation between self-report measures and IGT performance, but a lack of association between behavioural inhibition and IGT performance (Crone et al. 2003). Other studies indicated limited or no relation between self-reported impulsivity and IGT performance and other behavioral measures of risk taking (Meda et al., 2009; Reynolds et al., 2006).
The current study investigated the predictive value of neurocognitive measures of decision-making and inhibition in a non-clinical population of college students. Young adulthood is often a period of heavy alcohol use. Epidemiological research indicates that in the United States, 23% of college students are frequent binge drinkers, and 44% engaged in binge drinking in the past two weeks, whereas monthly binge drinking is reported by 39% of the general population (Wechsler et al., 2002; Harrison, Desai, & McKee, 2008). In humans, the prefrontal lobes mature throughout adolescence, and into early adulthood (Casey, Giedd, & Thomas, 2000). Therefore, decision-making skills and inhibition, processes that rely on prefrontal lobe functioning, may be especially vulnerable to the effects of heavy alcohol use during adolescence. Given the findings on the predictive role of decision-making, behavioral inhibition and self-reported impulsivity in a clinical alcohol dependent population, we included a decision making task - the Iowa Gambling Task (IGT; Bechara et al., 1999) - and a response inhibition task - the GoStop task - in our study. In the IGT, participants play a computerized card game in which they attempt to develop a winning strategy by selecting cards from advantageous, as opposed to disadvantageous decks. Disadvantageous performance on the IGT has been found in people with ventromedial prefrontal lobe damage (Bechara et al., 1994; but see Manes et al., 2002), and in individuals with a variety of disinhibited behaviors (Goudriaan et al., 2005; Rotherham-Fuller et al., 2004; van Honk et al., 2002; Whitlow et al., 2004). We also included a GoStop task, which is a stop signal task measuring speed of motor response inhibition (Dougherty et al., 2005).
The current study is a follow-up of a neurocognitive study that was part of a longitudinal study on college student health. In the cross-sectional paper from this study, heavy (binge) drinking subgroups performed worse on the IGT than lighter drinking groups, and pre-college drinking was related to worse performance on the IGT (Goudriaan, Grekin, & Sher, 2007). In addition, there was no relation between self-reported impulsivity and IGT performance (Goudriaan et al., 2007. The current study is a follow-up and extension of this investigation, designed to study the predictive value of neurocognitive tasks for heavy alcohol use at the end of college.
In summary, the current study is the first to examine the predictive value of a decision making task and an inhibition task on heavy alcohol use in a follow-up study of 200 college students. Participants, who ranged from very light alcohol drinkers, to heavy alcohol users and abusers, completed neurocognitive tasks, and were assessed on alcohol use before testing and two years later. We hypothesized that disadvantageous decision-making and diminished inhibition would be associated with higher alcohol use at follow-up, i.e., two years after the neurocognitive assessment. Given the association between heavy (binge) drinking, pre-college alcohol use, and disadvantageous decision-making reported in the first analyses of this study (Goudriaan, Grekin, & Sher, 2007), measures of alcohol use were included as covariates.
MATERIALS AND METHODS
Participants
Participants were a subgroup of 200 college students (50% female, mean age 20.4) drawn from an ongoing longitudinal study of college student health (The Intensive Multivariate Prospective Alcohol College-Transitions Study – IMPACTS, N = 3720 (Sher & Rutledge, 2007)). Latent class growth analyses (LCGAs), based on self-reported alcohol use data, were used to place each participant into a binge-drinking group. More specifically, participants were asked the following question, once per semester during their first two years in college (i.e., four times total): “How many times in the past 30 days did you have 5 or more alcoholic drinks on one occasion?” (response options: “never”; “once in the past 30 days”; “2–3 times in the past 30 days”; “1–2 times a week”; “3–4 times a week”, “5–6 times a week”; “nearly every day”; “every day”; or “twice a day or more”). Participants were classified as being binge drinkers if they answered “2–3 times in the past 30 days” or any higher frequency, and as non-binge drinkers if they answered any lower frequency. Based on these data, the four groups produced by the LCGA were: (1) low binge drinkers at all time points (36 % of the sample); (2) moderate binge drinkers at all time points (30%); (3) increasing binge drinkers, with low binge drinking levels at precollege, but increasing in binge drinking in the first and second college year (10%); (4) heavy binge drinkers from precollege throughout the second college year (24%).
For the purposes of this study, 25 male and 25 female participants from each of these four classes were recruited. Participants recruited for this neurocognitive study were comparable in alcohol use to the university population as a whole. A detailed description of participant recruitment can be found in (Goudriaan, Grekin, & Sher, 2007). The institutional review board of the University of Missouri-Columbia approved this study. All participants gave their informed consent before being included in the study.
Procedure
All participants performed the Iowa Gambling Task [IGT; performance division according to (Bechara et al., 1994)] and a StopSignal inhibition task in the second college year. At baseline and 2 years later, heavy alcohol use was assessed. Of the 200 participants, 176 were successfully retained at follow-up. Attrition was similar for male and female students (14 male and 10 female students did not participate at follow-up), and participants who did not participate at follow-up did not differ in (heavy) alcohol use from those who were retained.
Neurocognitive Tasks
Iowa Gambling Task (IGT)
A computerized version of the IGT was used (Bechara et al., 1999). In the IGT, subjects made a total of 100 card selections from four decks of cards. By selecting (i.e., clicking on) cards, participants won and lost imaginary money (i.e, after selecting a card, a message appeared on the screen that said “You won (amount) dollars and you lost (amount) dollars). Two disadvantageous decks (decks A and B) were associated with large rewards, but also with large losses, and choosing these decks resulted in net losses over the course of the task. Two advantageous decks (decks C and D) were associated with small rewards, but also small losses and these decks resulted in a net gain over the course of the task. Participants had to learn which decks were advantageous in the long run by making card selections. The task ended after one hundred card selections were made. Each deck contained 60 cards. Participants were not given any actual money. Instructions included a ‘hint’ that some decks were worse than others. Research has shown that the choice of real vs. fake money does not influence performance on the IGT, when the hint condition is used (Bowman & Turnbull, 2003; Fernie & Tunney, 2006). The dependent measure used to classify decision-making performance was the percentage of cards picked from the advantageous decks.
Thirty nine participants (20% of the total sample) finished all the cards in a deck (predominantly C or D). After finishing all cards in one of the decks, they started sampling cards from the 3 remaining decks again, thus producing an artifact in the data. Therefore, we eliminated analyses of the last stage of the task (Goudriaan et al., 2007). Advantageous decision making was therefore based on more than 50% of advantageous card choices from cards 1–80, instead of cards 1–100.
GoStop Task (Stop Signal Response Inhibition Task)
This task measures response inhibition on a 2-choice reaction time task. Five-digit numbers are presented in rapid succession (500 msec on, intertrial interval: 1500 msec). Participants are told to press a key on the computer keyboard when two identical five-digit numbers appear consecutively. Fifty percent of the 5-digit numbers are target trials, and 50% are filler trials (random non-matches). In half of the target trials, the second 5-digit number changes color (from black to red). When the number changes color, participants have to try to inhibit their response (i.e., refrain from pressing a key). The change of color takes place at 50–350 msec intervals (stop delay period) after the number appears on the screen, with 50 msec differences between intervals. For each stop delay period, 18–20 target-stop trials are present within the task. For a more elaborate description of this task, see Dougherty Mathias, Marsh, and Jagar (2005). We extracted stop signal reaction times (SSRTs) from the GoStop program (Dougherty et al., 2005), which uses a standard SSRT calculation, as suggested by Logan and colleagues (Logan, 1994). SSRTs were chosen as the dependent variable instead of percentage of correct responses, because the SSRT corrects for differences in mean reaction time between participants. Stop signals of 50, 150, 250, and 350 msec after the Go signal were presented in the GoStop task. For all participants with successful stop rates between 40–60% at the 50–350 msec intervals, the average SSRT from these stop signal intervals was taken. For participants who only had a successful stop rate between 40–60% in the part of the stop signal intervals (e.g. 150–350 msec), these intervals were taken to calculate a mean SSRT. Thus, by calculating SSRTs from stop signal intervals associated with a stop signal rate between 40–60%, we aimed to derive reliable SSRTs from this fixed stop interval GoStop task.
Alcohol use measures
Recently, controversy arose around the definition of binge drinking, since traditional thresholds for binge drinking (5/4 drinks per occasion) may be too low for college students (White, Kraus, & Swartzwelder, 2006). Therefore, both a subjective measure of heavy episodic drinking, including frequency of getting drunk and getting high, and a quantity/frequency measure of alcohol use in this college student sample were included as dependent measures.
We created a heavy drinking measure comprised of the following items; [1] frequency of getting lightheaded or a little high on alcohol, [2] frequency of getting drunk, and [3] frequency of having five or more drinks at one sitting (Sher & Rutledge, 2007). Weekly frequency of [1] getting lightheaded, [2] getting drunk, or [3] having five or more drinks at one sitting, were obtained from items assessing the number of occasions a participant reported feeling high, drunk, or having five or more drinks in one sitting during the previous 30 days. Participants’ responses were based on 8-point Likert scales ranging from 0 (e.g. didn’t get drunk during the past 30 days) to 7 (every day), and their responses were converted to weekly equivalents, with higher numbers indicating higher frequency of drinking. Scores for these questions ranged from zero to seven, and frequency scores were recoded to indicate the relative frequency with which specific behaviors were indulged in. These three questions had excellent reliability, with coefficient alpha ranging from .89 to .94 during the different data collection waves (waves 0–6). Thus, a maximum score of 21 could be obtained (when all the three items would occur during every day of the week). Furthermore, a quantity/frequency measure of alcohol use was included, calculated by multiplying the average quantity of alcohol used per drinking occasion by the average frequency of drinking occasions per week (assessed for each day separately).
Recent heavy drinking and the quantity/frequency measure of alcohol use, as explained above, were also collected at the end of second college year (time period immediately before neurocognitive testing). Therefore we included these two covariates in all analyses, because we wanted to control for the potential important confound of concurrent alcohol use.
Performance groups
For the IGT, an advantageous decision-making group and a disadvantageous decision making group was formed, according to the performance division used by Bechara and colleagues: advantageous decision-makers choose more than 50% of cards from the advantageous decks, whereas the disadvantageous decision-making group choose more than 50% of cards from the disadvantageous decks (Bechara et al., 1994). Thirty nine participants (20% of the total sample) finished all the cards in a deck (predominantly C or D). After finishing all cards in one of the decks, they started sampling cards from the 3 remaining decks again, thus producing an artifact in the data. Therefore, we eliminated analyses of the last stage of the task (Goudriaan, Grekin, Sher, 2007). Advantageous decision making was therefore based on more than 50% card choices from cards 1–80, instead of cards 1–100. For the GoStop task, the mean SSRTs were computed (see GoStop task description) and used for a median split into a low inhibition group and a high inhibition group. As some data were missing for some of the participants, and outliers in IGT or GoStop performance (>3SDs above or below the group average) were excluded from the analyses separately, slightly different subsamples of the total sample were present in the IGT and GoStop analyses.
In Table 1, demographic data and neurocogntive performance data including the mean number of cards chosen from the advantageous decks in the two decision making groups and the stop signal reaction time (SSRT) in the 150 and 250 ms delays for the two GoStop performance groups are displayed. The IGT performance and GoStop performance measures did not correlate significantly (Pearsons r = .06, p <.43).
Table 1.
Demographics and neurocognitive performance for the Iowa Gambling Task performance groups and for the GoStop performance groups.
| % Female | Age (SD) at baseline |
Alcoholic drinks/week baseline (SD) |
% choices advantageous decks IGT |
SSRT 150 ms (SD) |
SSRT 250 ms (SD) |
|
|---|---|---|---|---|---|---|
| Disadvant. IGT Group (n=36) | 54% | 19.9 (.35) | 10.2 (9.6) | 40.2% (12.9) | ||
| Advant. IGT group (n=139) | 51% | 19.9 (.32) | 11.2 (16.3) | 69.8% (11.2) | ||
| Low Inhibition Group (n=87) | 48% | 20.0 (.32) | 10.1 (13.6) | 216.1 (87.3) | 136.9 (41.9) | |
| High Inhibition Group (n=88) | 51% | 19.9 (.37) | 11.9 (16.5) | 161.0 (40.9) | 83.4 (47.6) |
Disadvant. IGT Group = Disadvantageous IGT performance group. Advant. IGT group = Advantageous IGT performance Group. SSRT= Stop Signal Reaction Time
Statistical Analyses
MANCOVAs were used (Performance Group × Gender factorial), to examine whether group differences in IGT and Stop Signal task performance (measured at year two) would influence future alcohol use at the end of year 4. The dependent measures were (1) the heavy drinking measure and (2) the quantity/frequency measure of alcohol use, at the end of year 4 as explained above. Baseline alcohol use (heavy drinking and quantity/frequency of alcohol use assessed at the end of the second college year, around time of neurocognitive testing) was included as a covariate in all analyses. When significant interaction effects were present in the MANCOVA, analyses were followed by univariate analyses (ANCOVAs) testing effects for each of the alcohol use measures separately.
- Additional covariates
A relation was present between IGT performance and ACT scores, and between IGT performance and pre-college heavy drinking in the cross-sectional analyses from this study (Goudriaan et al., 2007). We therefore examined the effects of these potentially important covariates in this prospective study as well. Pre-college heavy drinking was entered as a covariate in all analyses, but did not relate to heavy drinking or to the quantity/frequency measure of alcohol use at Time 2 (end of the fourth college year). Note, however, that concurrent quantity-frequency and concurrent heavy use was included in all analyses. However, for ACT scores a trend was present in some of the MANCOVAs, and therefore, ACT was retained as a covariate in all analyses. When significant effects are present, these are mentioned.
RESULTS
IGT performance and future alcohol use
The MANCOVA showed an overall IGT group effect for the drinking measures: F(2,166)=5.28, p<.01, corrected for concurrent heavy drinking and quantity/frequency. A gender effect was present, F(2,166)=9.88, p<.001, indicating that men scored higher on the alcohol measures than did women. A significant group by gender interaction was found, F(2,166)=6.50, p<.01, indicating that future alcohol use (heavy drinking measure and quantity/frequency measure) differed between men and women in the advantageous and disadvantageous decision making groups.
A separate ANCOVA for the heavy drinking measure revealed a main effect of group on the heavy drinking measure, F(1,168)=8.68, p<.01, indicating that, overall, the disadvantageous group had higher heavy drinking scores at follow-up compared to the advantageous decision making group, when correcting for concurrent heavy drinking and quantity/frequency of alcohol use. A significant gender by IGT performance group interaction was present for the heavy drinking measure, F(1,168)=8.96, p<.01: Therefore effects for men and women were analysed separately using ANCOVAs. A significant IGT effect for future heavy drinking was present for men, F(1,81)=10.35, p<.01, indicating that future heavy drinking was higher in men in the disadvantageous decision-making group compared to men in the advantageous decision-making group (see Figure 1). In female participants, no significant relation between performance group and heavy drinking was present (p=.47).
Figure 1.
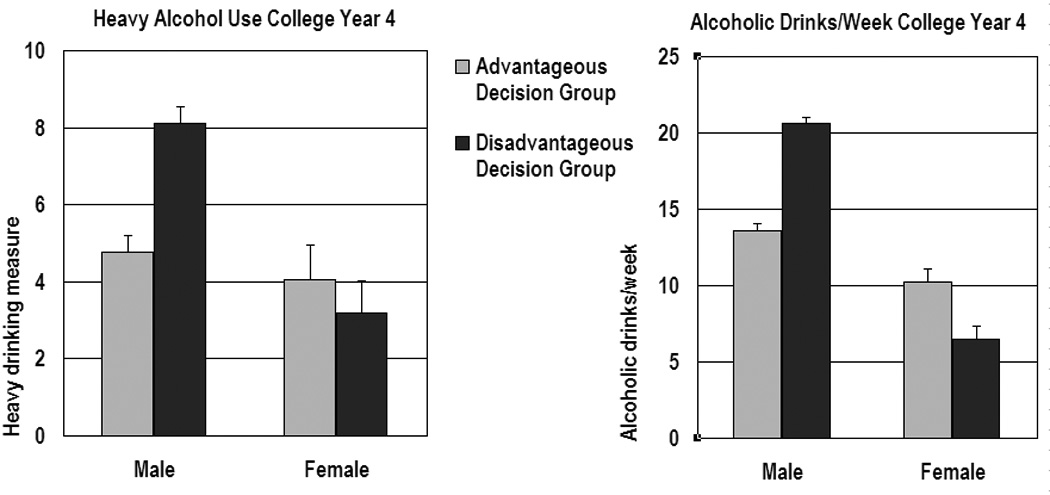
Alcohol measures for the advantageous decision-making group and for the disadvantageous decision-making group at two-year follow-up. Means are adjusted for alcohol use at time of neurocognitive testing (baseline). Error bars are standard errors of the mean. Although effects seem to be present for weekly alcohol use in female students, this effect did not reach significance, due to the significant effects of covariates (heavy alcohol use measure at Time 1 and heavy drinking measure at Time 1).
No significant main effect for the alcohol quantity/frequency measure was present, F(1,168)=2.15, p=.14, indicating that, overall, no differences were present on future alcohol quantity/frequency between the groups. However, a significant gender by IGT performance group interaction was present, F(1,168)=10.93, p<.01: Effects for men and women were therefore analysed separately using ANCOVAs. An effect was present in men for the alcohol quantity/frequency measure, F(1,80)=8.45, p<.01, indicating male disadvantageous decision-makers tended to have higher alcohol quantity/frequency scores 2 years later compared to male advantageous decision-makers. In women, no effect of IGT performance group on the alcohol quantity/frequency measure was present (p=.25), but significant effects of the covariates were present (heavy alcohol use measure at Time 1 and heavy drinking measure at Time 1).
GoStop task performance and future alcohol use
No group effect was present for the future alcohol use measures, F(2,164)=1.17, p<.31 (see Figure 2). A trend for a gender effect was present, F(2,164)=3.05, p=.05, indicating higher scores on the future alcohol use measures for men compared to women (Small differences in gender effects between the GoStop analysis and IGT analyses are due to the fact that slightly different subsamples were used for both analyses, due to exclusion of outliers, and missing data). No gender by group effect was present.
Figure 2.
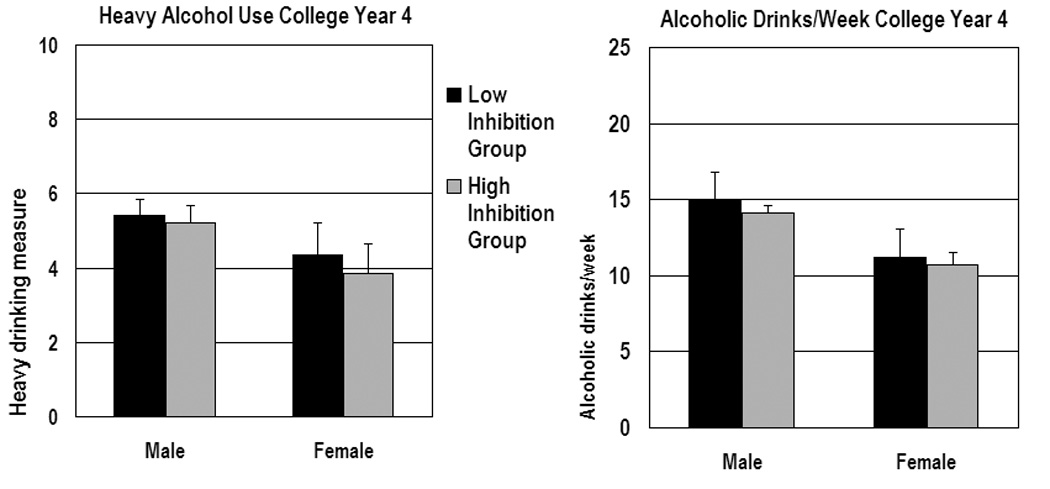
Alcohol measures for the low inhibition group and high inhibition group at two-year follow-up. Means are adjusted for alcohol use at time of neurocognitive testing (baseline). Error bars are standard errors of the mean.
Posthoc analyses
DSM-IV Alcohol Dependence proxy
In order to further assess the clinical significance of our findings, we examined whether disadvantageous decision making was related to a proxy measure of DSM-IV alcohol dependence. This proxy measure (published in Grekin & Sher, 2006) was comprised of IMPACTs survey items that were related to each of the seven DSM-IV alcohol dependence criteria Analyses with this measure indicated that the disadvantageous IGT performance group endorsed more alcohol dependence criteria at the end of the fourth college year than the advantageous IGT performance group, F(1,168)=4.70, p<.05. A trend for a group by gender interaction indicating that this effect tended to be stronger in male students than in female students did not reach significance F(1,168)= 2.00, p=.15.
DISCUSSION
This study examined whether neurocognitive tasks can predict future alcohol use beyond the predictive role of concurrent and earlier alcohol use, in a group of college students with different drinking patterns. Disadvantageous decision making on the IGT, a task relying on ventromedial prefrontal lobe functioning (Bechara et al., 1999; Bechara et al., 1994), was predictive of higher future alcohol use and heavy drinking in male students, whereas this relation was not present in female students. Diminished response inhibition did not predict future alcohol use, when concurrent alcohol use was accounted for. These findings extend our previous, mainly cross-sectional study on the association between binge drinking patterns and decision making performance (Goudriaan, Grekin, & Sher, 2007), and suggest that neurocognitive performance patterns prospectively predict heavy alcohol use in college students.
Disadvantageous decision making on the IGT, as defined by an objective performance of less than 50% of choices from advantageous decks, indicates risky choice patterns resulting in long-term losses and reflects a diminished ability to learn from negative consequences, a diminished sensitivity to rewards, or a combination of both (Bechara, Dolan, & Hindes, 2002; Bechara & Damasio, 2002; Goudriaan et al., 2005). In light of our current findings, we can tentatively conclude that this experimental decision-making task is associated with a real-life risky behavior that has potential long-term negative consequences: heavy drinking. Disadvantageous performance on the IGT can be defined by an objective, quantitative limit, and therefore, similar performance categorizations can be applied in future studies that use disadvantageous IGT performance as a risk indicator for future heavy drinking.
Studies in clinical substance dependent patients and pathological gamblers show that neural and behavioral markers of disadvantageous decision making and behavioural disinhibition are risk factors for relapse (Bowden-Jones et al., 2005; Durazzo et al., 2008; Goudriaan et al., 2008; Paulus et al., 2005). This study is one of the first to indicate that neurocognitive measures can predict disadvantageous alcohol use also in non-clinical populations, such as this college-student population. Studies in adolescents show that diminished performance on neurocognitive inhibition tasks and tasks involving evaluation of rewards and losses over time, are predictive of later development of substance abuse or addictive behaviors like problem gambling (Tarter et al., 2004; Vitaro, Arseneault, & Tremblay, 1999; Kirisci et al., 2004). Thus, neurocognitive functions can play an important role in different stages of substance use, abuse, and dependence.
Disadvantageous decision-making on the IGT was predictive of future heavy alcohol use in men but not in women. This gender interaction could be due to the heavier alcohol use patterns reported by men as compared to women, in this study. A review on neurocognitive functions in alcohol users indicates that diminished neurocognitive performance is more consistently found in studies that include alcohol users who drink more than 21 units of alcohol per week, compared to those studies that include alcohol users who drink less than 21 units per week (Parsons & Nixon, 1998). Still, it can be argued that, in women compared to men, relatively lower amounts of alcohol are reflective of heavier alcohol use, due to a lower body mass index and a lower metabolism for alcohol. In our study, women had lower scores both on the quantity/frequency measure of alcohol use, and on the heavy drinking measure that reflects subjective experiences of alcohol use (e.g., feeling drunk, feeling lightheaded). Because women score lower on both subjective and objective alcohol use measures, female students in this study may have a different drinking pattern than the male students in this study, experiencing less occasions of being drunken, or lightheaded, or of binge drinking. Preclinical studies show that binge drinking has detrimental effects on the rat brain (Obernier, Bouldin, & Crews, 2002). Thus, the lower scores of women on the (prospective) heavy alcohol use measure could relate to a less neurotoxic drinking pattern in women compared to men, resulting in a relation between disadvantageous decision making and future heavy alcohol use for men, but not for women.* Recent studies on brain development in adolescents and young adults indicate that brain maturation is finished earlier in female as opposed to male, young adults. Therefore, different interactions between the effects of alcohol on the maturing brain and decision-making skills, may be present in males and females. Future studies employing multiple neurocognitive test sessions over time, and including neuroimaging measures of brain maturation, could shed light on this issue. The interactions between decision-making performance and gender, in predicting future alcohol use measures, are in contrast to the cross-sectional findings from this study: no gender effects for the relationship between IGT performance and concurrent (heavy) binge drinking were present (Goudriaan, Grekin, & Sher).
Some limitations should be noted: This study did not encompass a broad neurocognitive battery. Thus, other cognitive and motivational processes that could have influenced future alcohol use were not included. In particular, increased attentional bias for drug cues and cue reactivity have also been found to predict relapse and treatment outcome (Cox, Pothos, & Hosier, 2007; Cox et al., 2002; Kosten et al., 2006; Kosten et al., 2006; Marissen et al., 2006). Future studies should therefore include tasks tapping these motivational factors. This study sample, which consisted primarily of Caucasian college students, aged 21 to 23, was representative of the larger student population at this large, midwestern, public university. Replication with other age groups and non-college students is clearly needed, and caution is required in generalizing to other populations.
Conclusions
Disadvantageous decision-making is a predictor of heavy drinking in male college students, but not in female college students at a two-year follow-up, when alcohol use at baseline is accounted for. These findings imply that neurocognitive measures can be used to test vulnerability for future heavy alcohol use.
Table 2.
Alcohol use measures at Time 1 (start of 3rd college year) and Time 2 (end of 4th college year)
| Heavy Drinking Measure Time 1 (baseline) |
Heavy Drinking Measure Time 2 |
Alcoholic drinks/week Time 1 (baseline) |
Alcoholic drinks/week Time 2 |
|
|---|---|---|---|---|
| Total sample | 4.25 (4.28) | 4.75 (4.45) | 12.24 (14.28) | 12.66 (13.54) |
| Female students | 4.07 (3.89) | 3.80 (3.14) | 10.20 (8.93) | 9.41 (9.53) |
| Male students | 4.49 (4.85) | 5.50 (4.97) | 14.21 (17.84) | 16.07 (16.11) |
Acknowledgements
The National Institute on Alcohol Abuse and Alcoholism grants R37AA7231, K05AA017242 and T32AA13526 (PI: Kenneth J. Sher) and P60 AA11990 (PI:Andrew C. Heath) supported this study. The Netherlands Organisation for Scientific Research (NWO) – Health Research and Development (ZonMw) supported this study by a grant to A. E. Goudriaan (VENI: #91676084, 2007–2011).
Footnotes
This study was carried out at the Department of Psychological Sciences, University of Missouri-Columbia
To investigate this possible explanation of this gender by decision-making interaction, we ran posthoc analyses to see whether disadvantageous decision-making was linked to future heavy alcohol use in the subgroup of female students who scored above the median for female participants on the heavy drinking measure at Time 1. Analysis of this female, heavier drinking, subgroup showed a trend, indicating that the female disadvantageous decision-making group scored higher on the quantity/frequency of alcohol use at Time 2, compared to the female advantageous decision-making group: F(1,44)=3.46, p=.07. No relation for this heavier drinking female subgroup was present between decision making and the heavy alcohol use measure at Time 2: F<1, p=.43. These analyses, although very preliminary, indicate that in female students with a higher alcohol use, a relation between decision-making and future (quantity/frequency) alcohol use may be present, and that the lack of effect in the entire female student group may be partly explained by the lower levels of alcohol use in female students.
References
- Bechara A, Damasio AR, Damasio H, Anderson SW. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition. 1994;50:7–15. doi: 10.1016/0010-0277(94)90018-3. [DOI] [PubMed] [Google Scholar]
- Bechara A, Damasio H. Decision-making and addiction (part I): impaired activation of somatic states in substance dependent individuals when pondering decisions with negative future consequences. Neuropsychologia. 2002;40:1675–1689. doi: 10.1016/s0028-3932(02)00015-5. [DOI] [PubMed] [Google Scholar]
- Bechara A, Damasio H, Damasio AR, Lee GP. Different contributions of the human amygdala and ventromedial prefrontal cortex to decision-making. Journal of Neuroscience. 1999;19:5473–5481. doi: 10.1523/JNEUROSCI.19-13-05473.1999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bechara A, Dolan S, Denburg N, Hindes A, Anderson SW, Nathan PE. Decision-making deficits, linked to a dysfunctional ventromedial prefrontal cortex, revealed in alcohol and stimulant abusers. Neuropsychologia. 2001;39:376–389. doi: 10.1016/s0028-3932(00)00136-6. [DOI] [PubMed] [Google Scholar]
- Bechara A, Dolan S, Hindes A. Decision-making and addiction (part II): myopia for the future or hypersensitivity to reward? Neuropsychologia. 2002;40:1690–1705. doi: 10.1016/s0028-3932(02)00016-7. [DOI] [PubMed] [Google Scholar]
- Bowden-Jones H, McPhillips M, Rogers R, Hutton S, Joyce E. Risk-taking on tests sensitive to ventromedial prefrontal cortex dysfunction predicts early relapse in alcohol dependency: a pilot study. J Neuropsychiatry Clin Neurosci. 2005;17:417–420. doi: 10.1176/jnp.17.3.417. [DOI] [PubMed] [Google Scholar]
- Bowman CH, Turnbull OH. Real versus facsimile reinforcers on the Iowa Gambling Task. Brain and Cognition. 2003;53:207–210. doi: 10.1016/s0278-2626(03)00111-8. [DOI] [PubMed] [Google Scholar]
- Casey BJ, Giedd JN, Thomas KM. Structural and functional brain development and its relation to cognitive development. Biol Psychol. 2000;54:241–257. doi: 10.1016/s0301-0511(00)00058-2. [DOI] [PubMed] [Google Scholar]
- Cox WM, Hogan LM, Kristian MR, Race JH. Alcohol attentional bias as a predictor of alcohol abusers' treatment outcome. Drug Alcohol Depend. 2002;68:237–243. doi: 10.1016/s0376-8716(02)00219-3. [DOI] [PubMed] [Google Scholar]
- Cox WM, Pothos EM, Hosier SG. Cognitive-motivational predictors of excessive drinkers' success in changing. Psychopharmacology (Berlin) 2007;192:499–510. doi: 10.1007/s00213-007-0736-9. [DOI] [PubMed] [Google Scholar]
- Dougherty DM, Mathias CW, Marsh DM, Jagar AA. Laboratory behavioral measures of impulsivity. Behav Res Methods. 2005;37:82–90. doi: 10.3758/bf03206401. [DOI] [PubMed] [Google Scholar]
- Durazzo TC, Gazdzinski S, Yeh PH, Meyerhoff DJ. Combined neuroimaging, neurocognitive and psychiatric factors to predict alcohol consumption following treatment for alcohol dependence. Alcohol and Alcoholism. 2008;43:683–691. doi: 10.1093/alcalc/agn078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fernie G, Tunney RJ. Some decks are better than others: the effect of reinforcer type and task instructions on learning in the Iowa Gambling Task. Brain and Cognition. 2006;60:94–102. doi: 10.1016/j.bandc.2005.09.011. [DOI] [PubMed] [Google Scholar]
- Giancola PR, Moss HB. Executive cognitive functioning in alcohol use disorders. Recent Developments in Alcohol Research. 1998;14:227–251. doi: 10.1007/0-306-47148-5_10. [DOI] [PubMed] [Google Scholar]
- Goldstein RZ, Volkow ND. Drug addiction and its underlying neurobiological basis: neuroimaging evidence for the involvement of the frontal cortex. American Journal of Psychiatry. 2002;159:1642–1652. doi: 10.1176/appi.ajp.159.10.1642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goudriaan AE, Grekin ER, Sher KJ. Decision making and binge drinking: a longitudinal study. Alcoholism, Clinical and Experimental Research. 2007;31:928–938. doi: 10.1111/j.1530-0277.2007.00378.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goudriaan AE, Oosterlaan J, de Beurs E, van den Brink W. Decision making in pathological gambling: A comparison between pathological gamblers, alcohol dependents, persons with Tourette syndrome, and normal controls. Cognitive Brain Research. 2005;23:137–151. doi: 10.1016/j.cogbrainres.2005.01.017. [DOI] [PubMed] [Google Scholar]
- Goudriaan AE, Oosterlaan J, de Beurs E, van den Brink W. The role of self-reported impulsivity and reward sensitivity versus neurocognitive measures of disinhibition and decision-making in the prediction of relapse in pathological gamblers. Psychol Med. 2008;38:41–50. doi: 10.1017/S0033291707000694. [DOI] [PubMed] [Google Scholar]
- Grekin ER, Sher KJ. Alcohol dependence symptoms among college freshmen: prevalence, stability, and person-environment interactions. Exp Clin Psychopharmacol. 2006;14:329–338. doi: 10.1037/1064-1297.14.3.329. [DOI] [PubMed] [Google Scholar]
- Harrison EL, Desai RA, McKee SA. Nondaily smoking and alcohol use, hazardous drinking, and alcohol diagnoses among young adults: findings from the NESARC. Alcohol Clin Exp Res. 2008;32:2081–2087. doi: 10.1111/j.1530-0277.2008.00796.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kirisci L, Tarter RE, Vanyukov M, Reynolds M, Habeych M. Relation between cognitive distortions and neurobehavior disinhibition on the development of substance use during adolescence and substance use disorder by young adulthood: a prospective study. Drug and Alcohol Dependence. 2004;76:125–133. doi: 10.1016/j.drugalcdep.2004.04.015. [DOI] [PubMed] [Google Scholar]
- Kosten TR, Scanley BE, Tucker KA, Oliveto A, Prince C, Sinha R, Potenza MN, Skudlarski P, Wexler BE. Cue-induced brain activity changes and relapse in cocaine-dependent patients. Neuropsychopharmacology. 2006;31:644–650. doi: 10.1038/sj.npp.1300851. [DOI] [PubMed] [Google Scholar]
- Krawczyk DC. Contributions of the prefrontal cortex to the neural basis of human decision making. Neuroscience and Biobehavioral Reviews. 2002;26:631–664. doi: 10.1016/s0149-7634(02)00021-0. [DOI] [PubMed] [Google Scholar]
- Krishnan-Sarin S, Reynolds B, Duhig AM, Smith A, Liss T, McFetridge A, Cavallo DA, Carroll KM, Potenza MN. Behavioral impulsivity predicts treatment outcome in a smoking cessation program for adolescent smokers. Drug Alcohol Depend. 2007;88:79–82. doi: 10.1016/j.drugalcdep.2006.09.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Logan GD. On the ability to inhibit thought and action. A users' guide to the stop signal paradigm. In: Dagenbach D, Carr TH, editors. Inhibitory processes in attention, memory and language. San Diego, CA: Academic Press; 1994. pp. 189–236. [Google Scholar]
- Manes F, Sahakian B, Clark L, Rogers R, Antoun N, Aitken M, Robbins T. Decision-making processes following damage to the prefrontal cortex. Brain. 2002;125:624–639. doi: 10.1093/brain/awf049. [DOI] [PubMed] [Google Scholar]
- Marissen MA, Franken IH, Waters AJ, Blanken P, van den BW, Hendriks VM. Attentional bias predicts heroin relapse following treatment. Addiction. 2006;101:1306–1312. doi: 10.1111/j.1360-0443.2006.01498.x. [DOI] [PubMed] [Google Scholar]
- Meda SA, Stevens MC, Potenza MN, Pittman B, Gueorguieva R, Andrews MM, Thomas AD, Muska C, Hylton JL, Pearlson GD. Investigating the behavioral and self-report constructs of impulsivity domains using principal component analysis. Behav Pharmacol. 2009;20:390–399. doi: 10.1097/FBP.0b013e32833113a3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Obernier JA, Bouldin TW, Crews FT. Binge ethanol exposure in adult rats causes necrotic cell death. Alcohol Clin Exp Res. 2002;26:547–557. [PubMed] [Google Scholar]
- Parsons OA, Nixon SJ. Cognitive functioning in sober social drinkers: a review of the research since 1986. Journal of Studies on Alcohol. 1998;59:180–190. doi: 10.15288/jsa.1998.59.180. [DOI] [PubMed] [Google Scholar]
- Paulus MP, Tapert SF, Schuckit MA. Neural activation patterns of methamphetamine-dependent subjects during decision making predict relapse. Archives of General Psychiatry. 2005;62:761–768. doi: 10.1001/archpsyc.62.7.761. [DOI] [PubMed] [Google Scholar]
- Reynolds B, Ortengren A, Richards JB, de Wit H. Dimensions of impulsive behavior: Personality and behavioral measures. Personality and Individual Differences. 2006;40:305–315. [Google Scholar]
- Rotherham-Fuller E, Shoptaw S, Berman SM, London ED. Impaired performance in a test of decision-making by opiate-dependent tobacco smokers. Drug and Alcohol Dependence. 2004;73:79–86. doi: 10.1016/j.drugalcdep.2003.10.003. [DOI] [PubMed] [Google Scholar]
- Sher KJ, Rutledge PC. Heavy drinking across the transition to college: predicting first-semester heavy drinking from precollege variables. Addictive Behaviors. 2007;32:819–835. doi: 10.1016/j.addbeh.2006.06.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tarter RE, Kirisci L, Habeych M, Reynolds M, Vanyukov M. Neurobehavior disinhibition in childhood predisposes boys to substance use disorder by young adulthood: direct and mediated etiologic pathways. Drug and Alcohol Dependence. 2004;73:121–132. doi: 10.1016/j.drugalcdep.2003.07.004. [DOI] [PubMed] [Google Scholar]
- van Honk J, Hermans EJ, Putman P, Montagne B, Schutter DJ. Defective somatic markers in sub-clinical psychopathy. Neuroreport. 2002;13:1025–1027. doi: 10.1097/00001756-200206120-00009. [DOI] [PubMed] [Google Scholar]
- Vitaro F, Arseneault L, Tremblay RE. Impulsivity predicts problem gambling in low SES adolescent males. Addiction. 1999;94:565–575. doi: 10.1046/j.1360-0443.1999.94456511.x. [DOI] [PubMed] [Google Scholar]
- Wechsler H, Lee JE, Kuo M, Seibring M, Nelson TF, Lee H. Trends in college binge drinking during a period of increased prevention efforts. Findings from 4 Harvard School of Public Health College Alcohol Study surveys: 1993–2001. J Am Coll Health. 2002;50:203–217. doi: 10.1080/07448480209595713. [DOI] [PubMed] [Google Scholar]
- White AM, Kraus CL, Swartzwelder H. Many college freshmen drink at levels far beyond the binge threshold. Alcohol Clin Exp Res. 2006;30:1006–1010. doi: 10.1111/j.1530-0277.2006.00122.x. [DOI] [PubMed] [Google Scholar]
- Whitlow CT, Liguori A, Livengood LB, Hart SL, Mussat-Whitlow BJ, Lamborn CM, Laurienti PJ, Porrini LJ. Long-term heavy marijuana users make costly decisions on a gambling task. Drug and Alcohol Dependence. 2004;76:107–111. doi: 10.1016/j.drugalcdep.2004.04.009. [DOI] [PubMed] [Google Scholar]