

Abstract
Purpose of review
Health professionals are presented with the challenge of prescribing physical activity that is likely to be sustained by the sedentary majority. Walking is eminently suited to physical activity prescription for inactive individuals as it is accessible to men and women of all age and social groups and poses little risk of injury. This paper reviews recent evidence of the health benefits of walking and promotion of walking behavior.
Recent Findings
Large observational studies consistently show associations between walking and cardiovascular disease (CVD) endpoints over long periods of follow-up. Intervention studies further support the health benefits of walking, showing improvements in clinical biomarkers and measures after shorter periods of follow-up. Walking appears to have CVD-related health benefits in younger, middle, and older men and women, in both healthy and patient populations. Pedometer-, mobile phone- and computer-based programs are effective in increasing walking levels. Neighborhood and workplace amenities and programs may be important supports for walking behaviors.
Summary
Walking has the potential to play a key role in the primary and secondary prevention of cardiovascular disease. Clinicians can prescribe walking to assist patients meet physical activity recommendations and help identify supports available to the patient.
Keywords: walking, physical activity, cardiovascular disease, disease prevention, health promotion, review
Introduction
Despite the documented benefits of physical activity (PA) and published activity guidelines [1], a large proportion of the population does not perform sufficient exercise to maintain optimal health [2]. Health professionals are faced with the challenge of prescribing PA that will be sustained by the sedentary majority. Walking is eminently suited to PA prescription as it requires no special skills or facilities and is achievable by virtually all age groups with little risk of injury [3]. It may more easily circumvent frequently cited barriers to exercise, such as “lack of time” and the belief that one is “not the sporty type” [4], than other forms of activity; it has been found to promote better adherence than more intense exercise [5]. Walking is the most commonly reported PA among adults [6-7] and is frequently cited as an example of moderate intensity exercise that adults can accumulate throughout the day in order to reach the goal of 150 minutes per week [1]. It is often the activity of choice when adults are counseled to incorporate additional PA into their lives (for e.g. [8]), and can be used as a means of active commuting, which may be more likely to be adopted and sustained than traditional exercise programs [9]. Walking has been described as the nearest activity to perfect exercise [10].
Building on several previous reviews [10-15], this paper reviews recent evidence of the health benefits of walking and promotion of walking behavior, with a particular focus on studies published since 2008. Section 1 summarizes the evidence that walking improves cardiovascular health. Section 2 reviews strategies to promote walking and provides evidence regarding the optimal manner by which walking might be encouraged in various settings.
Section 1: Current Evidence that walking improves cardiovascular health
The importance of walking in improving cardiovascular health is supported by both observational studies, which examine associations between walking and CVD endpoints, and intervention studies, which show changes in range of clinical markers of CVD.
Observational Studies
Observational studies suggest that walking for longer duration or distance may confer incremental protection against CVD (see Figure 1). A recent systematic review [15] of longitudinal studies examining CVD risk with leisure or total walking duration, distance, frequency, energy expenditure, and pace found broadly dose-dependent reductions in CVD risk with increasing walking levels. Based on a meta-analysis, Zheng and colleagues [16] estimate that 8 MET hours/week of walking (approximately 30 minutes/day, 5 days/week, consistent with PA recommendations [1] is associated with a 19% reduction in coronary heart disease (CHD) risk. Evidence that CVD risk declines with increasing walking pace is strong and consistent, although this may be confounded by the possibility that walking pace is an indicator of fitness [15, 17].
Figure 1.
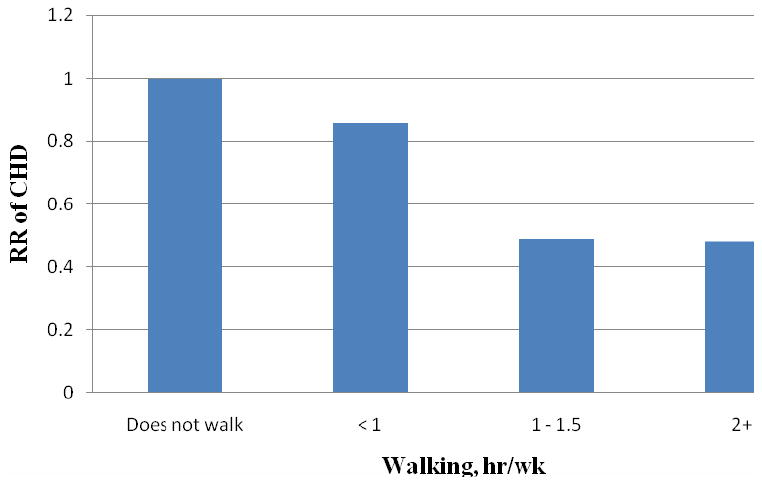
Dose-response relationship between walking hr/wk and risk of Coronoy Heart Disease in women, adjusted for age, smoking, alcohol, menopause, hormone therapy, family history.
Adapted from Lee et al, JAMA 2001; 285: 1447-1454
Associations between higher walking volume and intensity and reduced CVD risk are similar in men and women across a broad age spectrum. These comparisons of walking-CVD associations are confirmed by formal tests of heterogeneity by walking measure, sex, and age in two meta-analyses [16, 18]. Additionally, associations appear to be stronger for reducing the rates of ischemic stroke when compared to other CVD outcomes such as CHD or hemorrhagic stroke.
Special populations
The favorable relationships between walking and CVD risk observed among adults who did not report undertaking previous vigorous PA [15] suggest that walking is a promising strategy for yielding cardiovascular health benefit in the obese, who are less likely to perform vigorous PA [19], as well as for general, sedentary patient populations.
Walking as a component of secondary prevention for patients diagnosed with CVD is supported by the existing recommendations to incorporate exercise into cardiac rehabilitation [20] and to promote gradual progression of exercise intensity to prevent acute cardiovascular events in individuals with low fitness [21]. Recently, Hamer and Stamatakis [22] found that walking was associated with reduced risk of CVD mortality in Scottish men and women with diagnosed CVD; this finding was consistent with a prior study in a larger study population [23]. Walking may be particularly appropriate, and accessible to Type 2 diabetics who may be less able to perform vigorous PA than healthy individuals. Increased walking volume is associated with reduced CVD mortality [24] and events [25] among those diagnosed with diabetes, with some evidence that the cardioprotective effects of walking may be stronger in diabetics than those with normal glucose tolerance [26].
Active transportation
Walking or cycling for transportation is one way to accumulate PA as part of a daily routine and has become the focus of an emerging body of research. In a meta-analysis of prospective or case control studies examining CVD endpoints, walking and cycling for transportation was associated with an 11% reduction in CVD risk [27]. A case-control study suggests that the association between active commuting and incident myocardial infarction is partially mediated by changes in traditional CVD and inflammatory markers [28]. Recent cross-sectional investigations support beneficial relationships between active commuting and dyslipidemia [29], triglycerides [30-31], HDL [31-32], diastolic blood pressure [30], and fasting insulin levels [30], although such findings are variable across studies and population subgroups.
Most studies examine any (versus no) active transportation, which prohibits assessment of dose response and may contribute to inconsistencies across countries (e.g., Scandinavian populations typically exhibit more frequent active transportation relative to U.S. citizens) or gender [30]. Walking- and active-transit research is limited by potential bias due to pre-existing or subclinical illness and residual confounding by unmeasured CVD-related health behaviors, which are of critical concern in observational studies [15]. Experimental walking trials discussed in the next section can help to address these issues.
Experimental Studies
Fourteen intervention studies published in 2009 or early 2010 were identified in which walking was used as an intervention for one or more CVD-related health outcomes measured before and after intervention [33-46]. Due to the relatively short time frame of intervention trials, health outcomes are based on clinical biomarkers and measurements (e.g., lipids, blood pressure) rather than CVD endpoints (e.g., myocardial infarction, CHD). These interventions involved walking programs requiring subjects to walk 20-60 minutes per day on 2 to 5 days per week for a period of 3 weeks to 12 months. Five of these studies employed a randomized controlled trial design [33-37] with most others using quasi-experimental approaches.
Several studies examined cardiovascular fitness – an independent risk factor for cardiovascular disease [47] – as an outcome measure. In these studies, walking interventions resulted in consistent increases in fitness [37-40] or an improvement in ability to undertake exercise [41-43] post intervention. The only study where no alterations in fitness were observed was underpowered to detect such changes [36]. Recent evidence [38] confirms that walking needs to be of moderate intensity (e.g. increased breathing rate, turning red and perspiration) to increase aerobic fitness [48] and walking at a vigorous intensity confers greater fitness improvements [40]. In earlier work, instructing apparently healthy adults to walk “briskly” evoked intensity above the “moderate intensity” threshold [49-50]. Walking also produces an adequate training stimulus in older adults [51] and adults with CHD [52].
Resting blood pressure was used as an outcome measure in four of the interventions included in this review. In two studies, walking resulted in small but significant decreases in systolic and/or diastolic blood pressure among participants who had mild hypertension [34] or post-menopausal women with some indicators of metabolic syndrome [39]. Although the antihypertensive effect of aerobic exercise has been reported previously it has generally been in response to exercise which is at least moderate intensity [53]. The study by Hua and colleagues is the first to report lowered resting blood pressure as a result of a low intensity walking program in mild hypertensives [34]. Recent experimental studies also report favorable effects of walking programs on body mass [39-40], adiposity [37, 39] and lipid profiles [39, 44].
Three intervention studies were designed to improve intermittent claudication in patients with peripheral vascular disease [41, 43, 45]. Although all relatively small studies, they report consistent increases in the distance that patients can walk before the appearance of leg pain following short walking interventions.
Section 2: Supports for walking
Walking supports include programs and tools for individuals and community-level supports. Clinicians can help identify useful tools and recognize environmental barriers and supports to walking for their patients; they may also become advocates for community changes which make active lifestyles and active transportation more feasible.
Walking supports aimed at individuals
Pedometers
Pedometers are affordable, user-friendly tools which count the wearer's steps and provide readily available visual feedback [54] on levels of physical activity. They may be helpful in promoting increased activity in daily living by stimulating progressively increasing daily step totals [11]. A meta-analysis of 32 pedometer based PA interventions [55] reported that the use of pedometers achieved moderate increases in PA. Studies with an intervention strategy of 10,000 steps per day had the highest effect size compared to interventions with individualized goals or those which required participants to log daily steps.
Six studies published in the review period utilized pedometers to promote walking. A combination of setting step goals and using pedometers for self-monitoring is effective for increasing walking levels in overweight and obese women [56], older adults living in a community care facility [57], community dwelling adults [35] and patients in primary care [58]. For cardiac patients not attending cardiac rehabilitation, a telephone intervention incorporating pedometer use increased walking levels [59]. Lending pedometers through libraries is an effective, low-cost approach to enhance walking among community members [60].
Collectively these studies indicate that pedometers can be effective tools to promote walking in both patient and non-patient populations. To meet current PA guidelines [1] individuals should be encouraged to incrementally increase their walking levels to achieve the goal of walking a minimum of 3000 steps in 30 minutes on 5 days each week [61]. Expected baseline values for steps per day in special populations, e.g. heart and vascular diseases, have been published [62].
Internet/Email/Text message
While there is limited data on the effect of electronic/computer interventions to promote PA, current results are encouraging and it appears that response to an internet-based intervention is similar to responses to other more established interventions [63]. Increases in walking levels have been demonstrated following: an email-delivered program with employees [64]; e-mail messages sent on a cellular phone to men and women aged 30-49 years [65]; and, text message reminders sent to University students [66]. Repeat interventions or booster strategies in the format of mail, phone, internet, group sessions or combinations, may be needed to maintain increased levels of PA over the long term [67].
Active transport
Public transit users accumulate greater total walking distance across income groups than nontransit users, participate in more multimodal trips that involve walking, and often walk greater distances between destinations [68]. In the UK, a survey of approximately 4000 adults showed that more than two thirds of those who reported any active transport were sufficiently active through active transport alone to meet government recommendations for PA [69].
A systematic review of interventions to promote walking included 18 studies which used transportation walking; in general walking increased as a result of the intervention[13]. Recent evidence from interventions to promote walking for transport is scarce, with only one study published in 2009. In this Swedish study, middle-aged, abdominally obese women assigned to a moderate-intensity program with PA prescriptions focused on increased cycling and walking between work and home (with physician and group components), or a low-intensity group support, pedometer-based walking program, exhibited similar increases in walking commuting after 18 months [70]. In contrast with cycling, walking levels remained stable after the initial increase, suggesting that walking for transportation may be an effective long-term strategy for increased PA in abdominally obese women. Of note however is that 80% of subjects were public transport users at baseline and therefore this approach may have limited applicability to individuals who not do already use public transportation.
Environmental Influences
The low-cost and facility-free nature of walking makes it suitable for PA promotion in a range of settings including residential neigborhoods, worksites, and community settings.
Neighborhood Environment
The accessibility and ease of walking [6-7] may be enhanced by engaging in walking for exercise or transportation close to home. A rapidly growing body of built-environment research [71-74] provides some evidence as to how neighborhood amenities and design features may support or hinder neighborhood walking. Walking for transportation (as opposed to total walking or exercise walking) is generally more common in neighborhoods with lower levels of various urban sprawl measures [75] (or high “walkability” [76]) such as mixed land use (e.g., residences intermixed with businesses or recreation areas), proximity to retail (e.g., shops and restaurants), high housing density, and well-connected streets, which provide more direct walking routes. These relationships are variably evident in communities of middle- to older-age adults [77-81] and inconsistent for exercise walking [77, 81-83]. There is evidence that other built environment features such as parks, recreation facilities, and trails or bike lanes are also associated with higher walking levels [84-87].
However, the vast majority of built environment research is cross-sectional, and recent longitudinal findings are mixed. Lee and colleagues [88] found that lower total walking was related to higher urban sprawl in cross-sectional but not longitudinal analysis, suggesting that associations between sprawl and walking are due to residential self-selection. That is, already active households may select neighborhoods supportive of PA [89-90]. In contrast, results from a longitudinal study of African American women [82] which estimated changes in walking among women who moved to neighborhoods of higher or lower density supported causal influences of housing density on transportation walking.
Evidence from intervention studies is also mixed, although few focus specifically on walking and most examine multiple components such as walking programs, education, and pedestrian safety features (e.g., [91-94]), making it difficult to isolate the influence of modifications to the built environment. Large-scale community interventions to promote “active living” (e.g. [95-96]) have been implemented, but post-intervention walking levels have not yet been reported [97]. In an emerging line of research, objective measures of street-level pedestrian supports such as crossing aids or quality of sidewalks are related to higher walking levels [98-99]. Bus and transit availability may also support transportation walking, particularly in dense housing areas [82].
Worksite
Several studies have evaluated changes in walking behavior as a result of health promotion interventions in a range of settings. In most cases the interventions are multilevel and not walking specific but steps per day or self-reported minutes of walking per day or week are used as outcomes. In a recent review of PA promotion initiatives in the workplace, Pronk concluded that such programs have the potential to increase PA and improve the health of workers and reduce absenteeism and sick leave thereby generating positive financial return for employers [100].
Several studies measure walking outcomes following interventions designed to increase PA and/or alter diet at a regional community or workplace setting [57, 64, 101] with all reporting positive effects on walking levels. Gilson et al is the only study included in this review which specifically aimed to increase the volume of walking undertaken by staff in a workplace setting [102]. University employees, encouraged to use their break times to undertake brisk walks of at least 10 minutes or encouraged to stand and walk more as part of their normal working day, added 6-10 minutes of walking per day as a result of the intervention. Although these increases in workplace walking are small, when combined with other activity performed outside the workplace setting they may contribute to an overall volume of PA which results in health benefit.
Conclusion
Physicians and public health professionals are in a key position to recommend that their patients increase levels of daily walking. Evidence from epidemiological studies suggest that even small improvements in the amount of daily walking is better than no walking, and greater increases confer larger cardiovascular health benefits. Patients may accrue short-terms gains such as improved fitness, body composition, blood pressure and lipid profiles. Longer term benefits include reduced risk of CHD, coronary events and mortality. Patients should gradually raise their walking levels, with the public health recommendation of 150 minutes per week as a minimum goal. Clinicians can assure their patients that the risk of injury with this form of exercise is minimal.
Clinicians can also inform their patients of the vast array of community, workplace, and individual supports for walking. Pedometers are affordable and easy to use, and 10,000 steps per day goals appear to be effective in a wide range of populations. Use of public transit or walking for transportation also appear to help individuals increase overall walking levels. Patients may also wish to seek out opportunities at the workplace, such as using work breaks for brief, brisk walks. Clinicians should be aware that patients may live in neighborhoods more or less supportive of walking and that innovative mobile phone- and computer-based programs are becoming available. Methods for improving walking levels and sustaining them in the long term will be identified and developed in research still underway.
Acknowledgments
Funding: NIH Interdisciplinary Obesity Training Postdoctoral Fellowship, T32MH075854-04
Footnotes
Elaine M Murtagh. Conflicts of interest: none
Marie H Murphy. Conflicts of interest: none
Janne Boone-Heinonen. Conflicts of interest: none
Contributor Information
Elaine M Murtagh, Department of Arts Education & Physical Education, Mary Immaculate College, University of Limerick, Ireland.
Marie H Murphy, Sport & Exercise Sciences Research Institute, University of Ulster, Northern Ireland.
Janne Boone-Heinonen, Department of Nutrition, School of Public Health, University of North Carolina at Chapel Hill, NC, USA.
References
- 1.U.S. Department of Health and Human Services. 2008 Physical Activity Guidelines for Americans. 2008 [cited 2009 22nd June]; Available from: http://www.health.gov/paguidelines/pdf/paguide.pdf.
- 2.Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance System: Prevalence and Trends Data. [24th September 2009]; Available from: http://apps.nccd.cdc.gov/brfss/
- 3.Davison RCR, Grant S. Is Walking Sufficient Exercise for Health? Sports Medicine. 1993;16:369–73. doi: 10.2165/00007256-199316060-00002. [DOI] [PubMed] [Google Scholar]
- 4.Zunft HF, Friebe D, Seppelt B, et al. Perceived benefits and barriers to physical activity in a nationally representative sample in the European Union. Public Health Nutrition. 1999;2:153–60. doi: 10.1017/s1368980099000208. [DOI] [PubMed] [Google Scholar]
- 5.Dishman RK. Advances in Exercise Adherence. Champaign, IL: Human Kinetics; 1994. [Google Scholar]
- 6.Siegel PZ, Brackbill RM, Heath GW. The epidemiology of walking for exercise: implications for promoting activity among sedentary groups. Am J Public Health. 1995;85:706–10. doi: 10.2105/ajph.85.5.706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Eyler AA, Brownson RC, Bacak SJ, Housemann RA. The epidemiology of walking for physical activity in the United States. Med Sci Sports Exerc. 2003;35:1529–36. doi: 10.1249/01.MSS.0000084622.39122.0C. [DOI] [PubMed] [Google Scholar]
- 8.Dunn AL, Garcia ME, Marcus BH, et al. Six-month physical activity and fitness changes in Project Active, a randomized trial. Medicine and Science in Sports and Exercise. 1998;30:1076–83. doi: 10.1097/00005768-199807000-00009. [DOI] [PubMed] [Google Scholar]
- 9.Tin S, Woodward A, Thornley S, Ameratunga S. Cycling and walking to work in New Zealand, 1991-2006: regional and individual differences, and pointers to effective interventions. The International Journal of Behavioral Nutrition and Physical Activity. 2009;6 doi: 10.1186/1479-5868-6-64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Morris JN, Hardman AE. Walking to health. Sports Medicine. 1997;23:306–32. doi: 10.2165/00007256-199723050-00004. [DOI] [PubMed] [Google Scholar]
- 11.Franklin B. Walking: the undervalued prescription. Preventive Cardiology. 2006;9:56. doi: 10.1111/j.1520-037x.2006.4995.x. [DOI] [PubMed] [Google Scholar]
- 12.Murphy MH, Nevill AM, Murtagh EM, Holder RL. The effect of walking on fitness, fatness and resting blood pressure: A meta-analysis of randomised, controlled trials. Preventive Medicine. 2007;44:377–85. doi: 10.1016/j.ypmed.2006.12.008. [DOI] [PubMed] [Google Scholar]
- 13.Ogilvie D, Foster CE, Rothnie H, et al. Interventions to promote walking: systematic review. British Medical Journal. 2007;334:1204–7. doi: 10.1136/bmj.39198.722720.BE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Williams D, Matthews C, Rutt C, et al. Interventions to increase walking behavior. Medicine and Science in Sports and Exercise. 2008;40:S567. doi: 10.1249/MSS.0b013e31817c7006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *15.Boone-Heinonen J, Evenson KR, Taber DR, Gordon-Larsen P. Walking for prevention of cardiovascular disease in men and women: a systematic review of observational studies. Obes Rev. 2009;10:204–17. doi: 10.1111/j.1467-789X.2008.00533.x. [DOI] [PMC free article] [PubMed] [Google Scholar]; This systematic review of observational studies which assess the relationship between walking and CVD endpoints considers variation in study findings in relation to various study design and methodological considerations. It includes a wide range of CVD outcomes.
- *16.Zheng H, Orsini N, Amin J, et al. Quantifying the dose-response of walking in reducing coronary heart disease risk: meta-analysis. Eur J Epidemiol. 2009;24:181–92. doi: 10.1007/s10654-009-9328-9. [DOI] [PubMed] [Google Scholar]; This meta-analysis of observational studies which assess the relationship between walking and CHD specifically examines dose-response and provides pooled effect size and formal tests of heterogeneity by population subgroup and study design features.
- 17.Bertoni AG, Whitt-Glover MC, Chung H, et al. The association between physical activity and subclinical atherosclerosis: the Multi-Ethnic Study of Atherosclerosis. Am J Epidemiol. 2009;169:444–54. doi: 10.1093/aje/kwn350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hamer M, Chida Y. Walking and primary prevention: a meta-analysis of prospective cohort studies. Br J Sports Med. 2008;42:238–43. doi: 10.1136/bjsm.2007.039974. [DOI] [PubMed] [Google Scholar]
- 19.Erlichman J, Kerbey AL, James WP. Physical activity and its impact on health outcomes. Paper 2: Prevention of unhealthy weight gain and obesity by physical activity: an analysis of the evidence. Obes Rev. 2002;3:273–87. doi: 10.1046/j.1467-789x.2002.00078.x. [DOI] [PubMed] [Google Scholar]
- 20.Leon AS, Franklin BA, Costa F, et al. Cardiac rehabilitation and secondary prevention of coronary heart disease: an American Heart Association scientific statement from the Council on Clinical Cardiology (Subcommittee on Exercise, Cardiac Rehabilitation, and Prevention) and the Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity), in collaboration with the American association of Cardiovascular and Pulmonary Rehabilitation. Circulation. 2005;111:369–76. doi: 10.1161/01.CIR.0000151788.08740.5C. [DOI] [PubMed] [Google Scholar]
- 21.Thompson PD, Franklin BA, Balady GJ, et al. Exercise and acute cardiovascular events placing the risks into perspective: a scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism and the Council on Clinical Cardiology. Circulation. 2007;115:2358–68. doi: 10.1161/CIRCULATIONAHA.107.181485. [DOI] [PubMed] [Google Scholar]
- 22.Hamer M, Stamatakis E. Physical activity and mortality in men and women with diagnosed cardiovascular disease. Eur J Cardiovasc Prev Rehabil. 2009;16:156–60. doi: 10.1097/HJR.0b013e32831f1b77. [DOI] [PubMed] [Google Scholar]
- 23.Wannamethee SG, Shaper AG, Walker M. Physical activity and mortality in older men with diagnosed coronary heart disease. Circulation. 2000;102:1358–63. doi: 10.1161/01.cir.102.12.1358. [DOI] [PubMed] [Google Scholar]
- 24.Gregg EW, Gerzoff RB, Caspersen CJ, et al. Relationship of walking to mortality among US adults with diabetes. Arch Intern Med. 2003;163:1440–7. doi: 10.1001/archinte.163.12.1440. [DOI] [PubMed] [Google Scholar]
- 25.Hu FB, Stampfer MJ, Solomon C, et al. Physical activity and risk for cardiovascular events in diabetic women. Ann Intern Med. 2001;134:96–105. doi: 10.7326/0003-4819-134-2-200101160-00009. [DOI] [PubMed] [Google Scholar]
- 26.Smith TC, Wingard DL, Smith B, et al. Walking decreased risk of cardiovascular disease mortality in older adults with diabetes. J Clin Epidemiol. 2007;60:309–17. doi: 10.1016/j.jclinepi.2006.06.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hamer M, Chida Y. Active commuting and cardiovascular risk: a meta-analytic review. Prev Med. 2008;46:9–13. doi: 10.1016/j.ypmed.2007.03.006. [DOI] [PubMed] [Google Scholar]
- 28.Wennberg P, Wensley F, Johansson L, et al. Reduced risk of myocardial infarction related to active commuting: inflammatory and haemostatic effects are potential major mediating mechanisms. Eur J Cardiovasc Prev Rehabil. 2010;17:56–62. doi: 10.1097/HJR.0b013e32832f3b11. [DOI] [PubMed] [Google Scholar]
- 29.Guo X, Jia Z, Zhang P, et al. Impact of mode of transportation on dyslipidaemia in working people in Beijing. Br J Sports Med. 2009;43:928–31. doi: 10.1136/bjsm.2008.049171. [DOI] [PubMed] [Google Scholar]
- 30.Gordon-Larsen P, Boone-Heinonen J, Sidney S, et al. Active commuting and cardiovascular disease risk: the CARDIA study. Arch Intern Med. 2009;169:1216–23. doi: 10.1001/archinternmed.2009.163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.von Huth Smith L, Borch-Johnsen K, Jorgensen T. Commuting physical activity is favourably associated with biological risk factors for cardiovascular disease. Eur J Epidemiol. 2007;22:771–9. doi: 10.1007/s10654-007-9177-3. [DOI] [PubMed] [Google Scholar]
- 32.Barengo NC, Kastarinen M, Lakka T, et al. Different forms of physical activity and cardiovascular risk factors among 24-64-year-old men and women in Finland. Eur J Cardiovasc Prev Rehabil. 2006;13:51–9. doi: 10.1097/00149831-200602000-00008. [DOI] [PubMed] [Google Scholar]
- 33.Griffith K, Wenzel J, Shang J, et al. Impact of a walking intervention on cardiorespiratory fitness, self-reported physical function, and pain in patients undergoing treatment for solid tumors. Cancer. 2009;115:4874–84. doi: 10.1002/cncr.24551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Hua L, Brown C, Hains S, et al. Effects of Low-Intensity Exercise Conditioning on Blood Pressure, Heart Rate, and Autonomic Modulation of Heart Rate in Men and Women with Hypertension. Biological Research For Nursing. 2009;11:129. doi: 10.1177/1099800408324853. [DOI] [PubMed] [Google Scholar]
- 35.Gray S, Baker G, Wright A, et al. The effect of a 12 week walking intervention on markers of insulin resistance and systemic inflammation. Preventive Medicine. 2009;48:39–44. doi: 10.1016/j.ypmed.2008.10.013. [DOI] [PubMed] [Google Scholar]
- 36.Costello E, Raivel K, Wilson R. The Effects of a Twelve-Week Home Walking Program on Cardiovascular Parameters and Fatigue Perception of Individuals with Multiple Sclerosis: A Pilot Study. Cardiopulmonary Physical Therapy Journal. 2009;20:5. [PMC free article] [PubMed] [Google Scholar]
- 37.Morton R, West D, Stephens J. Heart rate prescribed walking training improves cardiorespiratory fitness but not glycaemic control in people with type 2 diabetes. Journal of Sports Sciences. 2010;28:93–9. doi: 10.1080/02640410903365685. [DOI] [PubMed] [Google Scholar]
- 38.van Uffelen J, Chinapaw M, Hopman-Rock M, van Mechelen W. Feasibility and effectiveness of a walking program for community-dwelling older adults with mild cognitive impairment. Journal of aging and physical activity. 2009;17:398. doi: 10.1123/japa.17.4.398. [DOI] [PubMed] [Google Scholar]
- 39.Roussel M, Garnier S, Lemoine S, et al. Influence of a walking program on the metabolic risk profile of obese postmenopausal women. Menopause. 2009;16:566. doi: 10.1097/gme.0b013e31818d4137. [DOI] [PubMed] [Google Scholar]
- *40.Nicklas B, Wang X, You T, et al. Effect of exercise intensity on abdominal fat loss during calorie restriction in overweight and obese postmenopausal women: a randomized, controlled trial. American Journal of Clinical Nutrition. 2009;89:1043. doi: 10.3945/ajcn.2008.26938. [DOI] [PMC free article] [PubMed] [Google Scholar]; This study compared three 20 week interventions (diet, diet and moderate intensity walking, diet and vigorous intensity walking) which produced equal energy deficits in all three groups. All three groups lost similar amounts of weight, the diet only group lost more lean mass, and individuals who walked at a vigorous intensity achieved greater increases in aerobic fitness.
- 41.Barak S, Stopka C, Archer Martinez C, Carmeli E. Benefits of Low-Intensity Pain-Free Treadmill Exercise on Functional Capacity of Individuals Presenting With Intermittent Claudication Due to Peripheral Arterial Disease. Angiology. 2009;60:477. doi: 10.1177/0003319708322388. [DOI] [PubMed] [Google Scholar]
- 42.Lam T, Luttmann K, Houldin A, Chan C. Treadmill-Based Locomotor Training with Leg Weights to Enhance Functional Ambulation in People with Chronic Stroke: A Pilot Study. Journal of Neurologic Physical Therapy. 2009;33:129. doi: 10.1097/NPT.0b013e3181b57de5. [DOI] [PubMed] [Google Scholar]
- 43.Leone A, Laudani R, Definite G, et al. Unbalanced risk factors, could compromise the effectiveness of physical training in patients with intermittent claudication? Minerva cardioangiologica. 2009;57:165. [PubMed] [Google Scholar]
- 44.Morrison K, Braham R, Dawson B, Guelfi K. Effect of a sand or firm-surface walking program on health, strength, and fitness in women 60-75 years old. Journal of aging and physical activity. 2009;17:196. doi: 10.1123/japa.17.2.196. [DOI] [PubMed] [Google Scholar]
- 45.Mouser M, Zlabek J, Ford C, Mathiason M. Community trial of home-based exercise therapy for intermittent claudication. Vasc Med. 2009;14:103. doi: 10.1177/1358863X08098596. [DOI] [PubMed] [Google Scholar]
- 46.Chiang C, Sun F. The Effects of a Walking Program on Older Chinese American Immigrants With Hypertension: A Pretest and Posttest Quasi-Experimental Design. Public Health Nursing. 2009;26:240–8. doi: 10.1111/j.1525-1446.2009.00776.x. [DOI] [PubMed] [Google Scholar]
- 47.Blair SN, Cheng Y, Holder JS. Is physical activity or physical fitness more important in defining health benefits? Medicine and Science in Sports and Exercise. 2001;33:S379–S99. doi: 10.1097/00005768-200106001-00007. [DOI] [PubMed] [Google Scholar]
- 48.Swain DP, Franklin BA. VO2 reserve and the minimal intensity for improving cardiorespiratory fitness. Medicine and Science in Sports and Exercise. 2002;34:152–7. doi: 10.1097/00005768-200201000-00023. [DOI] [PubMed] [Google Scholar]
- 49.Murtagh EM, Boreham CAG, Murphy MH. Speed and exercise intensity of recreational walkers. Preventive Medicine. 2002;35:397–400. doi: 10.1006/pmed.2002.1090. [DOI] [PubMed] [Google Scholar]
- 50.Hardman AE, Jones PRM, Norgan NG, Hudson A. Brisk Walking Improves Endurance Fitness without Changing Body Fatness in Previously Sedentary Women. Eur J Appl Physiol Occup Physiol. 1992;65:354–9. doi: 10.1007/BF00868140. [DOI] [PubMed] [Google Scholar]
- 51.Porcari J, McCarron R, Kline G, et al. Is Fast Walking an Adequate Aerobic Training Stimulus for 30- to 69-Year-Old Men and Women? The Physician and Sports Medicine. 1987;15:119–29. doi: 10.1080/00913847.1987.11709285. [DOI] [PubMed] [Google Scholar]
- 52.Quell KJ, Porcari JP, Franklin BA, et al. Is brisk walking an adequate aerobic training stimulus for cardiac patients? Chest. 2002;122:1852–6. doi: 10.1378/chest.122.5.1852. [DOI] [PubMed] [Google Scholar]
- 53.Fagard R, Cornelissen V. Effect of exercise on blood pressure control in hypertensive patients. European Journal of Cardiovascular Prevention & Rehabilitation. 2007;14:12. doi: 10.1097/HJR.0b013e3280128bbb. [DOI] [PubMed] [Google Scholar]
- 54.Tudor-Locke C. Promoting Lifestyle Physical Activity: Experiences With the First Step Program. American Journal of Lifestyle Medicine. 2009;3:50S. doi: 10.1177/1559827609331710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Kang M, Marshall S, Barreira T, Lee J. Effect of pedometerbased physical activity interventions: a meta-analysis. Res Q Exerc Sport. 2009;80:648–55. doi: 10.1080/02701367.2009.10599604. [DOI] [PubMed] [Google Scholar]
- 56.Pal S, Cheng C, Egger G, et al. Using pedometers to increase physical activity in overweight and obese women: a pilot study. BMC Public Health. 2009;9:309. doi: 10.1186/1471-2458-9-309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Rosenberg D, Kerr J, Sallis J, et al. Feasibility and outcomes of a multilevel place-based walking intervention for seniors: A pilot study. Health and Place. 2009;15:173–9. doi: 10.1016/j.healthplace.2008.03.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *58.McKay J, Wright A, Lowry R, et al. Walking on prescription: The utility of a pedometer pack for increasing physical activity in primary care. Patient Education and Counseling. 2009;76:71–6. doi: 10.1016/j.pec.2008.11.004. [DOI] [PubMed] [Google Scholar]; This pedometer intervention provides evidence for increasing walking through primary care settings.
- 59.Furber S, Butler L, Phongsavan P, et al. Randomised controlled trial of a pedometerbased telephone intervention to increase physical activity among cardiac patients not attending cardiac rehabilitation. Patient Education and Counseling. 2009 doi: 10.1016/j.pec.2009.11.012. [DOI] [PubMed] [Google Scholar]
- 60.Ryder H, Faloon K, Levesque L, McDonald D. Partnering With Libraries to Promote Walking Among Community-Dwelling Adults: A Kingston Gets Active Pilot Pedometer-Lending Project. Health Promotion Practice. 2009;10:588. doi: 10.1177/1524839907311049. [DOI] [PubMed] [Google Scholar]
- 61.Marshall S, Levy S, Tudor-Locke C, et al. Translating Physical Activity Recommendations into a Pedometer-Based Step Goal 3000 Steps in 30 Minutes. American Journal of Preventive Medicine. 2009;36:410–5. doi: 10.1016/j.amepre.2009.01.021. [DOI] [PubMed] [Google Scholar]
- 62.Tudor-Locke C, Washington T, Hart T. Expected values for steps/day in special populations. Preventive Medicine. 2009;49:3–11. doi: 10.1016/j.ypmed.2009.04.012. [DOI] [PubMed] [Google Scholar]
- 63.Marcus B, Ciccolo J, Sciamanna C. Using electronic/computer interventions to promote physical activity. British Medical Journal. 2009;43:102. doi: 10.1136/bjsm.2008.053744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Sternfeld B, Block C, Quesenberry C, et al. Improving Diet and Physical Activity with ALIVE A Worksite Randomized Trial. American Journal of Preventive Medicine. 2009;36:475–83. doi: 10.1016/j.amepre.2009.01.036. [DOI] [PubMed] [Google Scholar]
- 65.Yamawaki K, Oka K, Nakamura Y. Effect of a Walking Program with the E-mail Function of Cellular Phone. International Journal of Sport and Health Science. 2009 1001130042. [Google Scholar]
- 66.Prestwich A, Perugini M, Hurling R. Can implementation intentions and text messages promote brisk walking? A randomized trial. Health psychology: official journal of the Division of Health Psychology, American Psychological Association. 2010;29:40. doi: 10.1037/a0016993. [DOI] [PubMed] [Google Scholar]
- 67.Müller-Riemenschneider F, Reinhold T, Nocon M, Willich S. Long-term effectiveness of interventions promoting physical activity: A systematic review. Preventive Medicine. 2008;47:354–68. doi: 10.1016/j.ypmed.2008.07.006. [DOI] [PubMed] [Google Scholar]
- 68.Lachapelle U, Frank L. Transit and Health: Mode of Transport, Employer-Sponsored Public Transit Pass Programs and Physical Activity. Journal of Public Health Policy. 2009:S73–S94. doi: 10.1057/jphp.2008.52. [DOI] [PubMed] [Google Scholar]
- 69.Adams J. Prevalence and socio-demographic correlates of “active transport” in the UK: Analysis of the UK Time Use Survey 2005. Preventive Medicine. 2010 doi: 10.1016/j.ypmed.2010.01.006. In press. [DOI] [PubMed] [Google Scholar]
- 70.Hemmingsson E, Uddén J, Neovius M, et al. Increased physical activity in abdominally obese women through support for changed commuting habits: a randomized clinical trial. International Journal of Obesity. 2009;33:645–52. doi: 10.1038/ijo.2009.77. [DOI] [PubMed] [Google Scholar]
- 71.Saelens BE, Handy SL. Built environment correlates of walking: a review. Med Sci Sports Exerc. 2008;40:S550–66. doi: 10.1249/MSS.0b013e31817c67a4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Saelens BE, Sallis JF, Frank LD. Environmental correlates of walking and cycling: findings from the transportation, urban design, and planning literatures. Ann Behav Med. 2003;25:80–91. doi: 10.1207/S15324796ABM2502_03. [DOI] [PubMed] [Google Scholar]
- 73.Wendel-Vos W, Droomers M, Kremers S, et al. Potential environmental determinants of physical activity in adults: a systematic review. Obes Rev. 2007;8:425–40. doi: 10.1111/j.1467-789X.2007.00370.x. [DOI] [PubMed] [Google Scholar]
- 74.Papas MA, Alberg AJ, Ewing R, et al. The built environment and obesity. Epidemiol Rev. 2007;29:129–43. doi: 10.1093/epirev/mxm009. [DOI] [PubMed] [Google Scholar]
- 75.Ewing R, Schmid T, Killingsworth R, et al. Relationship between urban sprawl and physical activity, obesity, and morbidity. Am J Health Promot. 2003;18:47–57. doi: 10.4278/0890-1171-18.1.47. [DOI] [PubMed] [Google Scholar]
- 76.Frank LD, Schmid TL, Sallis JF, et al. Linking objectively measured physical activity with objectively measured urban form: findings from SMARTRAQ. Am J Prev Med. 2005;28:117–25. doi: 10.1016/j.amepre.2004.11.001. [DOI] [PubMed] [Google Scholar]
- 77.Rodriguez DA, Evenson KR, Diez Roux AV, Brines SJ. Land use, residential density, and walking. The multi-ethnic study of atherosclerosis. Am J Prev Med. 2009;37:397–404. doi: 10.1016/j.amepre.2009.07.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Nagel CL, Carlson NE, Bosworth M, Michael YL. The relation between neighborhood built environment and walking activity among older adults. Am J Epidemiol. 2008;168:461–8. doi: 10.1093/aje/kwn158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Yen IH, Michael YL, Perdue L. Neighborhood environment in studies of health of older adults: a systematic review. Am J Prev Med. 2009;37:455–63. doi: 10.1016/j.amepre.2009.06.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Li F, Harmer PA, Cardinal BJ, et al. Built environment, adiposity, and physical activity in adults aged 50-75. Am J Prev Med. 2008;35:38–46. doi: 10.1016/j.amepre.2008.03.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Shigematsu R, Sallis JF, Conway TL, et al. Age Differences in the Relation of Perceived Neighborhood Environment to Walking. Medicine and Science in Sports and Exercise. 2009;41:314–21. doi: 10.1249/MSS.0b013e318185496c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *82.Coogan PF, White LF, Adler TJ, et al. Prospective study of urban form and physical activity in the Black Women's Health Study. Am J Epidemiol. 2009;170:1105–17. doi: 10.1093/aje/kwp264. [DOI] [PMC free article] [PubMed] [Google Scholar]; This recent longitudinal study examines several neighborhood features in relation to walking for exercise and transportation. Housing density was related to walking for transportation in longitudinal analysis.
- 83.Ball K, Timperio A, Salmon J, et al. Personal, social and environmental determinants of educational inequalities in walking: a multilevel study. J Epidemiol Community Health. 2007;61:108–14. doi: 10.1136/jech.2006.048520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Michael YL, Perdue LA, Orwoll ES, et al. Physical Activity Resources and Changes in Walking in a Cohort of Older Men. Am J Public Health. 2010;100:654–60. doi: 10.2105/AJPH.2009.172031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Kaczynski AT, Henderson KA. Environmental correlates of physical activity: a review of evidence about parks and recreation. Leisure Sciences. 2007;29:315–54. [Google Scholar]
- 86.Kaczynski AT, Johnson AJ, Saelens BE. Neighborhood land use diversity and physical activity in adjacent parks. Health Place. 2010;16:413–5. doi: 10.1016/j.healthplace.2009.11.004. [DOI] [PubMed] [Google Scholar]
- 87.Giles-Corti B, Broomhall MH, Knuiman M, et al. Increasing walking: how important is distance to, attractiveness, and size of public open space? Am J Prev Med. 2005;28:169–76. doi: 10.1016/j.amepre.2004.10.018. [DOI] [PubMed] [Google Scholar]
- *88.Lee IM, Ewing R, Sesso HD. The built environment and physical activity levels: the Harvard Alumni Health Study. Am J Prev Med. 2009;37:293–8. doi: 10.1016/j.amepre.2009.06.007. [DOI] [PMC free article] [PubMed] [Google Scholar]; This recent longitudinal study examines an urban sprawl index in relation to walking as well as overall physical activity and several obesity and CVD-related outcomes. After comparing longitudinal and cross-sectional results, the authors conclude that sprawl-health associations are due to self-selection of neighborhoods.
- 89.Mokhtarian PL, Cao X. Examining the impacts of residential selection on travel behavior: a focus on methodologies. Trans Research Part B. 2008;42:204–28. [Google Scholar]
- 90.Boone-Heinonen J, Gordon-Larsen P, Guilkey D, et al. Environment and physical activity dynamics: the role of residential self-selection. Psychology of Sport and Exercise. 2010 doi: 10.1016/j.psychsport.2009.09.003. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Krieger J, Rabkin J, Sharify D, Song L. High point walking for health: creating built and social environments that support walking in a public housing community. Am J Public Health. 2009;99 3:S593–9. doi: 10.2105/AJPH.2009.164384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Tester J, Baker R. Making the Playfields Even: Evaluating the impact of an environmental intervention on park use and physical activity. Prev Med. 2009 doi: 10.1016/j.ypmed.2009.01.010. [DOI] [PubMed] [Google Scholar]
- 93.Cohen DA, Golinelli D, Williamson S, et al. Effects of park improvements on park use and physical activity: policy and programming implications. Am J Prev Med. 2009;37:475–80. doi: 10.1016/j.amepre.2009.07.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Cohen DA, Sehgal A, Williamson S, et al. New recreational facilities for the young and the old in Los Angeles: policy and programming implications. J Public Health Policy. 2009;30 1:S248–63. doi: 10.1057/jphp.2008.45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Deehr R, Shumann A. Active Seattle: Achieving Walkability in Diverse Neighborhoods. American Journal of Preventive Medicine. 2009;37:S403–S11. doi: 10.1016/j.amepre.2009.09.026. [DOI] [PubMed] [Google Scholar]
- 96.Schasberger M, Hussa C, Polgar M, et al. Promoting and developing a trail network across suburban, rural, and urban communities. American Journal of Preventive Medicine. 2009;37:S336–S44. doi: 10.1016/j.amepre.2009.09.012. [DOI] [PubMed] [Google Scholar]
- 97.Bussel J, Leviton L, Orleans C. Active living by design: perspectives from the Robert Wood Johnson Foundation. Am J Prev Med. 2009;37:S309–12. doi: 10.1016/j.amepre.2009.09.019. [DOI] [PubMed] [Google Scholar]
- 98.Shay E, Rodriguez DA, Cho G, et al. Comparing objective measures of environmental supports for pedestrian travel in adults. Int J Health Geogr. 2009;8:62. doi: 10.1186/1476-072X-8-62. [DOI] [PMC free article] [PubMed] [Google Scholar]