

Abstract
Background/purpose
While endoscopic sphincterotomy (EST) is performed worldwide for the removal of common bile duct stones, many biliary endoscopists hesitate to regard endoscopic papillary balloon dilation (EPBD) as a standard procedure for treatment. Therefore, the aim of this review is to re-evaluate the status of EPBD for the treatment of common bile duct stones.
Results
A major benefit of EPBD is preservation of papillary function, which is not complete but may be greater than that after EST. The disadvantages of EPBD compared with EST are that EPBD is difficult to use for the removal of larger stones because of the smaller biliary opening, it requires more frequent use of mechanical lithotripsy, and it is associated with a higher incidence of pancreatitis, although the risks of bleeding and perforation are low. Since the biliary sphincter is easily dilated with a balloon catheter, EPBD may be effective for patients with anatomic anomalies, such as after gastric bypass surgery or in the presence of a periampullary diverticulum. No standard procedure exists to reduce the risk of acute pancreatitis with EPBD.
Conclusion
EPBD is feasible, however, we must pursue less hazardous techniques of papillary balloon dilation. Furthermore, we must understand the benefits and limitations of EPBD and determine whether it could provide clinical benefits for long-term complications.
Keywords: Endoscopic papillary balloon dilation, Endoscopic sphincterotomy, Common bile duct stones
Introduction
Endoscopic sphincterotomy (EST) was developed by Classen and Demling [1], Kawai and colleagues [2], and Sohma and colleagues [3] in 1973 for the non-surgical therapy of common bile duct stones, and has been widely accepted as an effective procedure. Many studies have demonstrated the therapeutic benefits of EST [4–6]. However, EST also has negative aspects, including early dangerous complications such as bleeding, perforation, and permanent loss of sphincter function. Endoscopic papillary balloon dilation (EPBD) has been advocated as an alternative treatment to EST, with possible advantages. EPBD is easier to perform than EST, and does not have the short-term complications of bleeding and perforation. Furthermore, preserving the biliary sphincter may result in a decrease in long-term complications. However, several concerns exist with EPBD, such as the difficulty of removing larger stones because of the smaller biliary opening, the more frequent need for mechanical lithotripsy, and the higher incidence of pancreatitis after the procedure, compared with EST [7–10]. Some endoscopists believe that EPBD will become the standard treatment of choice for bile duct stones; others do not share this point of view.
The aim of this review is to re-evaluate the current status of EPBD for the treatment of common bile duct stones. In addition, less hazardous techniques of papillary balloon dilation which avoid complications such as pancreatitis are discussed.
Historical background of EPBD
EST carries an 8–12% risk of early complications, such as bleeding, duodenal perforation, and pancreatitis [5, 11, 12]. To avoid these complications, EPBD was introduced by Staritz and colleagues in 1983 [13] as a less traumatic procedure. They originally used a special balloon catheter, which was 15 mm in diameter with a banana shape, in 15 patients for the treatment of biliary diseases including common bile duct stones and found that no complications occurred. Although little attention was paid to EPBD due to the high incidence of acute pancreatitis [14, 15], it was subsequently re-evaluated by May and colleagues in 1993 [16], and by MacMathuna and coworkers [17, 18] in 1994 and 1995. These US reports showed that EPBD was a safe and effective alternative to EST for the management of small bile duct stones and that the incidence of post-EPBD pancreatitis was similar to that with EST. Moreover, in 1997 in Europe, Bergman and colleagues assessed the outcome of 101 patients with common bile duct stones treated with EPBD or EST in a prospective randomized controlled trial [19]. They concluded that the success rate of EPBD was similar to that of EST, with no difference in the rate of early complications, including pancreatitis, suggesting that EPBD may be a valuable alternative to EST in patients with common bile duct stones. Komatsu and colleagues [20] also reported preferable outcomes of EPBD in 226 Japanese patients with common bile duct stones in 1998. From these results, it appeared that the use of EPBD had spread broadly throughout the world. However, one international multicenter trial caused hesitation regarding the use of EPBD because of an increased risk of post-procedure pancreatitis [21, 22]. DiSario and coworkers reported in 2004 that the incidence of severe complications, including pancreatitis, was significantly higher in the EPBD group than that in the EST group, and that there were two deaths due to pancreatitis after papillary balloon dilation and none with EST [8]. In addition, multivariate analysis showed balloon dilation to be the only factor significantly associated with morbidity [23]. Thus, EPBD is regarded as a risky procedure, and has largely been abandoned in routine clinical practice by US endoscopists. In contrast, EPBD is still a popular procedure for the removal of common bile duct stones in parts of Europe, Korea, and Japan.
Advantages and disadvantages of EPBD
One of the major potential advantages of EPBD over EST is the preservation of papillary sphincter function [24–27]. EST permanently destroys the function of the biliary sphincter by cutting it, leading to duodenobiliary reflux which can cause long-term complications, such as cholangitis, recurrent stones [28–31], and the possibility of malignant transformation of the choledochal epithelium [31]. In contrast, EPBD is expected to restore papillary function, because the sphincter of Oddi is dilated by inflation of a balloon, which appears to be less hazardous to the papilla of Vater. MacMathuna and colleagues [32] studied histopathological changes after papillary balloon dilation using a porcine model, and revealed that papillary balloon dilation caused neither smooth muscle disruption nor fibrosis, and no alteration of papillary architecture. Manometric studies indicated at least partial recovery of papillary function 1 month after EPBD [24], although transient papillary dysfunction occurred 1 week after EPBD [24, 27]. Manometric studies also demonstrated that papillary function at 1 year was improved compared with that at 1 week, but still remained significantly lower than function before EPBD, suggesting that although preservation of papillary function after EPBD was not complete, it was greater than that after EST [27]. Interestingly, EPBD does not adversely affect gallbladder motility in the long term (5 years), based on results of a study of gallbladder volumes determined by ultrasonography [25]. In response to these findings, it is necessary to continue to investigate further clinical benefits for long-term complications.
On the basis of preservation of papillary function, EPBD is an attractive option, especially in young patients with common bile duct stones. However, it is not that simple because the rate of post-procedural pancreatitis could be higher with EPBD than with EST. Thus, we must identify the limitations as well as the potential advantages of EPBD.
Several randomized controlled trials have compared the success rates of stone removal and the frequency of early complications of EPBD with EST. Weinberg and coworkers [33] performed a meta-analysis of the results of fifteen randomized clinical trials comparing EPBD and EST for the removal of common bile duct stones by searching the Cochrane Library, MEDLINE, and EMBASE up to January 2004. According to this meta-analysis, EPBD is statistically less successful for stone removal, requires higher rates of mechanical lithotripsy, and carries a higher risk of pancreatitis. Interestingly, the subgroup analysis showed that the pancreatitis risk is higher for patients <60 years of age in the EPBD group. In contrast, while no significant difference was found in the rates of perforation, bleeding occurred significantly less frequently with EPBD, suggesting that EPBD may be preferable in patients with coagulopathy. Furthermore, EPBD causes significantly fewer short-term and long-term infections, suggesting that EPBD should be the preferred strategy in patients who are at risk for infection. Although there was no statistically significant difference between EPBD and EST with regard to overall mortality, the authors concluded that EPBD seemed to play a clinical role, possibly greater in older patients rather than in young people, in the risk of death from pancreatitis.
Since the biliary sphincter is easily dilated with a balloon catheter, EPBD could be a safe and effective technique for the treatment of patients with anatomical anomalies such as those due to gastric bypass surgery or in the presence of a periampullary diverticulum [34–36]. Bergman and colleagues conducted a randomized trial of EPBD and EST for the treatment of common bile duct stones in patients with a prior Billroth II gastrectomy [36]. The study showed that EPBD was easier to perform than EST in these patients, the risk of bleeding was virtually absent, and the risk of pancreatitis was not significantly increased.
Consideration of safer techniques for EPBD
The opening of the bile duct and the pancreatic duct is surrounded by a complex arrangement of smooth muscle collectively called the sphincter of Oddi, which comprises the sphincter choledochus, sphincter pancreaticus, sphincter ampullae, and fasciculus longitudinalis. In most cases, the meshwork of muscle fibers around the ampulla of Vater at the level of the oral protrusion inside the muscle layer of the duodenum and at the level passing through the wall of the duodenum is dense and thick (Fig. 1). However, at the level proximal to the junction with the pancreatic duct outside the duodenal wall, smooth muscle of common bile duct generally becomes rough and thin, and partly disappears (Fig. 2). Balloon dilation seemed theoretically less hazardous. However, it is possible that the inflammatory edema caused by the inflated balloon compresses the sphincter around the pancreatic duct, inducing obstructive pancreatitis. Alternatively, it is possible that the thin and weak smooth muscle around the common bile duct could tear when the balloon is inflated within the bile duct, leading to the leakage of bile into the parenchyma of the pancreas, which could also cause pancreatitis. We must avoid trauma to the sphincter and pancreatic orifice as much as possible. Therefore, we must pursue safe techniques to reduce the risk of acute pancreatitis with EPBD. Unfortunately, there is no standard technique for EPBD. Table 1 shows the diameters of the dilation balloons, maximum pressure, length of time of balloon inflation, and number of times the balloon was inflated described in various studies of EPBD for the removal of common bile duct stones, sorted in order of the incidence of post-EPBD pancreatitis. EPBD procedures vary, as shown in Table 1, and the relationship between the incidence of pancreatitis and the EPBD maneuvers seems to be extremely indistinct. Tsujino and coworkers showed statistically significant risk factors for post-EPBD pancreatitis using univariate and multivariate analysis [39]. Although age, periampullary diverticulum, pancreatic duct opacification, dilation balloon diameter, dilation pressure and dilation time were statistically significant by univariate analysis, only pancreatic duct opacification was a significant risk factor for post-EPBD pancreatitis by multivariate analysis. Furthermore, they evaluated efficacy and safety of their recent modified dilation methods, in which the balloon was inflated slowly (0.5 atmospheres per approximately 15 s) until disappearance of the balloon waist, and the pressure was then maintained for 15 s, compared with the initial method, in which the balloon was gradually (approximately 1 min) inflated to 8 atmospheres for 2 min. The results showed that the incidence of post-procedural pancreatitis tended to be lower in the modified group than in the initial group, and that the severity of pancreatitis was significantly reduced in the modified group. These findings indicate that lower pressure and shorter duration of dilation is less traumatic to the papilla, resulting in fewer complications. In addition, Nakagawa and colleagues also investigated the risk factors for acute pancreatitis after EPBD [38]. They described two cases of acute pancreatitis after EPBD in whom the inflation pressure needed for disappearance of the notch sign (i.e., the balloon waist) was over 5 atmospheres. The study concluded that poor function of the minor duodenal papilla, high inflation pressure required for disappearance of the notch sign, severe abdominal pain, and a lengthy procedure increased the risk of post-EPBD pancreatitis. If it is true that high pressure of the inflation balloon required for disappearance of the notch sign is associated with the occurrence of acute pancreatitis, we must stop dilating the balloon in the papilla of Vater, and change to papillary sphincterotomy when the notch sign does not disappear at a high inflation pressure, at most over 5 atmospheres. Since the commercially available balloons for EPBD are generally made from polyethylene terephthalate or nylon, they start to dilate rapidly at low pressure, and the size of the balloon reaches more than 90% of the fully inflated balloon diameter, even at a low inflation pressure of 0.5 atmospheres. EPBD with gradual inflation of the balloon may be very important for decreasing the risk of trauma to the sphincter of Oddi, especially during the first 0–2 atmospheres of inflation. The speed of balloon inflation within the sphincter of Oddi may be the most important factor for safe EPBD.
Fig. 1.
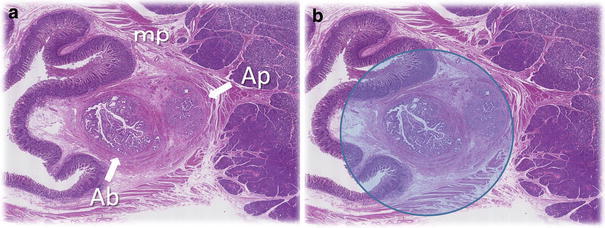
Normal histology of the sphincter of Oddi at the oral protrusion inside the muscle layer of the duodenum. a The bile duct and the pancreatic duct are close together and are surrounded by the dense and thick sphincter of Oddi. Ab portion of the bile duct, Ap portion of the pancreatic duct, mp muscle of the duodenum. b Image of the papillary balloon dilation at the level of the portion of the bile duct inside the muscle layer of the duodenum. A blue and translucent circle, 8 mm in diameter, represents the maximal inflation of the balloon
Fig. 2.
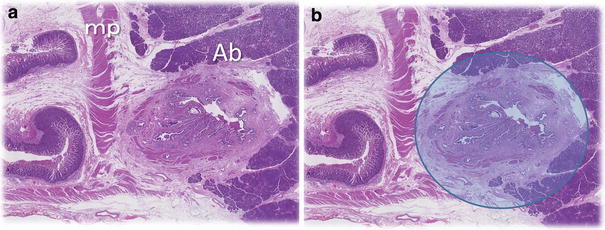
Normal histology of the sphincter of Oddi at the portion of the bile duct outside the duodenal wall. a The bile duct is surrounded by the rough and thin sphincter of Oddi, which has partly disappeared on the side of the parenchyma of the pancreas. Ab portion of the bile duct, mp muscle of the duodenum. b Image of the papillary balloon dilation at the portion of the bile duct outside the duodenal wall. A blue and translucent circle, 8 mm in diameter, represents the maximal inflation of the balloon
Table 1.
EPBD procedures associated with post-EPBD pancreatitis
| References | Pancreatitis (%) | Balloon diameter (mm) | Maximum pressure of inflation balloon (atm) | Length of time (process) of balloon inflation | Number of times balloon inflated |
|---|---|---|---|---|---|
| Ochi et al. [37] | 0.0 | 8 | 8 | Inflated for 60 s and reinflated a further two times at 60 s intervals | 3 |
| Nakagawa and Ohara [38] | 1.0 | 8 | Notch | Gradually inflated in a period 2 min and immediately deflated | 1 |
| Tsujino et al. [39] | 4.0 | 8, 6, 4 | Notch | Slowly inflated at 0.5 atm per 15 s and maintained for 15 s | 1 |
| Vlavianos et al. [40] | 4.8 | 10 | 12 | Inflated to a pressure of 12 atm for 30 s | Repeated until satisfactory |
| Natsui et al. [41] | 5.7 | 8 | 8 | Inflated at a pressure of 8 atm for 2 min | 1 |
| Yasuda et al. [27] | 5.7 | 8 | 6 | Inflated twice and each inflation lasted for 1 min at 6 atm | 2 |
| Sugiyama et al. [42] | 6.0 | 8 | nd | Inflated to a diameter of 8 mm for 2 min | 1 |
| Bergman et al. [19] | 6.9 | 8 | Notch | Inflated over 1–2 min and maintained for 45–60 s | 1 |
| Tsujino et al. [39] | 7.4 | 8, 6, 4 | 8 | Gradually (approximately 1 min) inflated with 8 atm for 2 min | 1 |
| Minami et al. [43] | 10.0 | 8 | nd | Inflated within 3 min to 15–20 psi | 1 |
| Fujita et al. [44] | 10.9 | 8, 6, 4 | Notch | Expanded slowly over a period of nearly 3 min and kept for 15 s | 1 |
| DiSario et al. [8] | 15.4 | 8 or less | nd | Dilated to 8 mm or the maximum size of the duct and inflated for 1 min | 1 |
| Watanabe et al. [10] | 16.7 | 8 | 7 | Inflated up to 8 mm in diameter at a pressure of 7 atm for 2 min | 1 |
| Tanaka et al. [45] | 18.7 | 8 | 8 | Inflated to 8 atm for 2 min | 1 |
| Arnold et al. [46] | 20.0 | 8 | 10 | Inflated to a diameter of 8 mm for 60 s and repeated for additional 60 s | 2 |
EPBD endoscopic papillary balloon dilation, Ref references, nd not described, Notch pressure needed for disappearance of the notch sign
Furthermore, we should note that the inflation pressure required for disappearance of the notch sign is not always equal to the maximum pressure of the inflation balloon which yields the maximum diameter of the balloon. The diameter of the inflation balloon is usually maximal at 8–12 atmospheres, dependent on the manufacturer and type. The balloon must be inflated to the maximum pressure to obtain its maximum diameter. Unfortunately, it is not known how long the maximum pressure should be maintained within the sphincter or the number of times balloon dilation should be repeated for safe and efficient EPBD.
In addition, another way to avoid pancreatitis may be to select the optimal balloon diameter, which should be smaller than the diameter of the common bile duct to prevent trauma to the sphincter and pancreatic orifice. In addition to the key roles of balloon dilation, concerns still exist about the size and number of stones in EPBD. Although patients with large common bile duct stones, of a size exceeding the diameter of the papillary orifice after EPBD, frequently require additional treatment, such as mechanical lithotripsy, to achieve ductal clearance, EPBD appears to be an appropriate treatment for small bile duct stones. In patients with 3 or less bile duct stones <10 mm, EPBD of the biliary sphincter to a diameter of 8 mm is nearly always successful without the need for additional EST or mechanical lithotripsy and without a significant difference in the incidence of post-procedure pancreatitis from that after EST [47]. Randomized controlled trials comparing EPBD with EST suggest that EPBD is at least as effective as EST in patients with small-to-moderate-sized bile duct stones [48]. Based on the results of the JESED study group, patients with common bile duct stones 14 mm or less in maximum shorter diameter on radiographic images can be treated with either EST or EPBD with the same success rate for stone clearance and frequency of complications [44].
Recent issues in EPBD
One of the major limitations of EPBD, unlike EST, is the difficulty of removing larger stones because the biliary opening is not enlarged sufficiently. In comparative studies, mechanical lithotripsy was used more frequently in the EPBD group than in the EST group [33, 48]. An additional EST after EPBD was also required in 10–19% of patients who underwent papillary balloon dilation [33]. In 2003, Ersoz and coworkers reported that EST followed by sequential EPBD using a 12– 20-mm diameter balloon may be effective for difficult removal of large bile duct stones (more than 15 mm) and/or barrel-shaped stones, or in patients with tapering of the distal common bile duct; the rate of early complications, such as mild cholangitis (3%), mild pancreatitis (3%), and mild-to-moderate bleeding (9%), was acceptable [49]. After that report, the efficacy and safety of large size balloon dilation of the biliary orifice after biliary sphincterotomy by another endoscopist was evaluated in the management of difficult-to-extract bile duct stones in several studies (Table 2). Although the extent of sphincterotomy varies among these studies, ranging from limited to extended, success rates and complication rates after EST combined with EPBD may be acceptable [49–57]. Interestingly, it is likely that complete stone removal in the first session would be accomplished at higher rates with EST plus EPBD with a large size balloon than with EST alone. The degree of sphincterotomy before EPBD remains to be determined. We need to establish whether small sphincterotomy with large size balloon dilation could lead to late complications, such as stricture of the biliary orifice.
Table 2.
Outcome of EST followed by EPBD for treatment of choledocholithiasis
| References | Country | n | Extent of EST | Balloon diameter (mm) | Overall success rate (%) | Success rate in the first session (%) | Complications (%) |
|---|---|---|---|---|---|---|---|
| Ersoz et al. [49] | Turkey | 58 | Large | 12–20 | 100 | 82.9 | 15.5 |
| Bang et al. [50] | Korea | 22 | Limited | 10–15 | 100 | 72.7 | 4.5 |
| Minami et al. [51] | Japan | 88 | Small | 20 | 98.9 | 98.9 | 4.5 |
| Heo et al. [52] | Korea | 100 | Minor (1/3) | 12–20 | 97.0 | 83.0 | 5.0 |
| Attasaranya et al. [53] | USA | 103 | Initial or extended | 12–18 | nd | 95.0 | 5.4 |
| Kochhar et al. [54] | India | 74 | Limited | 10, 12, 15, 18 | 91.9 | 83.8 | 21.6 |
| Itoi et al. [55] | Japan | 53 | 2/3≤ | 15, 18, 20 | 100 | 96.0 | 4.0 |
EST endoscopic sphincterotomy, EPBD endoscopic papillary balloon dilation, Ref references, nd not described
Conclusions
EPBD has been performed in many patients for the treatment of common bile duct stones all over the world, especially in parts of Asia and Europe, and most patients have benefitted from it. Unfortunately, no standard procedure for safe EPBD has been established. Thus, we must work to understand the benefits and limitations of EPBD, and to determine the theoretical and practical safe procedures of EPBD in order to make it an alternative to EST.
References
- 1.Classen M, Demling L. Endoskopishe shinkterotomie der papilla Vateri und Stein extraction aus dem Duktus Choledochus [German] Dtsch Med Wochenschr. 1974;99:496–497. doi: 10.1055/s-0028-1107790. [DOI] [PubMed] [Google Scholar]
- 2.Kawai K, Akasaka Y, Murakami K. Endoscopic sphincterotomy of the ampulla of Vater. Gastrointest Endosc. 1974;20:148–151. doi: 10.1016/S0016-5107(74)73914-1. [DOI] [PubMed] [Google Scholar]
- 3.Sohma S, Takekawa I, Okamoto Y, Matsuda T, Ono M, Aoyagi T, et al. Endoscopic papillotomy: a new approach for extraction of residual stones. Gastroenterol Endosc. 1974;16:446–452. [Google Scholar]
- 4.Ikeda S, Tanaka M, Matsumoto S, Yoshimoto H, Itoh H. Endoscopic sphincterotomy: Long-term results in 408 patients with complete follow-up. Endoscopy. 1988;20:13–17. doi: 10.1055/s-2007-1018117. [DOI] [PubMed] [Google Scholar]
- 5.Cotton PB, Lehman G, Vennes J, Geenen JE, Russell RCG, Meyers WC, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc. 1991;37:383–393. doi: 10.1016/S0016-5107(91)70740-2. [DOI] [PubMed] [Google Scholar]
- 6.Rabenstein T, Schneider TH, Hahn EG, Ell C. 25 years of endoscopic sphincterotomy in Erlangen: assessment of experience in 3,498 patients. Endoscopy. 1998;30:A194–A201. doi: 10.1055/s-2007-1001439. [DOI] [PubMed] [Google Scholar]
- 7.Gerke H, Baillie J. To cut or stretch? Am J Gastroenterol. 2004;99:1461–1463. doi: 10.1111/j.1572-0241.2004.40358.x. [DOI] [PubMed] [Google Scholar]
- 8.DiSario JA, Freeman ML, Bjorkman DJ, MacMathuna P, Petersen BT, Jaffe PE, et al. Endoscopic balloon dilation compared with sphincterotomy for extraction of bile duct stones. Gastroenterology. 2004;127:1291–1299. doi: 10.1053/j.gastro.2004.07.017. [DOI] [PubMed] [Google Scholar]
- 9.Tsujino T, Isayama H, Komatsu Y, Ito Y, Toda M, Minagawa N, et al. Risk factors for pancreatitis in patients with common bile duct stones managed by endoscopic papillary balloon dilation. Am J Gastroenterol. 2005;100:38–42. doi: 10.1111/j.1572-0241.2005.40638.x. [DOI] [PubMed] [Google Scholar]
- 10.Watanabe H, Yoneda M, Tominaga K, Monma T, Kanke K, Shimada T, et al. Comparison between endoscopic papillary balloon dilation and endoscopic sphincterotomy for the treatment of common bile duct stones. J Gastroenterol. 2007;42:56–62. doi: 10.1007/s00535-006-1969-9. [DOI] [PubMed] [Google Scholar]
- 11.Freeman ML, Nelson DB, Sherman S, Haber GB, Herman ME, et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med. 1996;335:909–918. doi: 10.1056/NEJM199609263351301. [DOI] [PubMed] [Google Scholar]
- 12.Boender J, Nix GA, Ridder MA, Blankenstein M, Schütte HE, Dees J, et al. Endoscopic papillotomy for common bile duct stones: factors influencing the complication rate. Endoscopy. 1994;26:209–216. doi: 10.1055/s-2007-1008945. [DOI] [PubMed] [Google Scholar]
- 13.Staritz M, Ewe K, Meyer KH. Endoscopic papillary dilation (EPD) for the treatment of common bile duct stones and papillary stenosis. Endoscopy. 1983;15:197–198. doi: 10.1055/s-2007-1021507. [DOI] [PubMed] [Google Scholar]
- 14.Bader M, Geenen JE, Hogan WJ, Dodds WJ, Venu R, Johnson GK. Endoscopic balloon dilatation of the sphincter of Oddi in patients with suspected biliary dyskinesia; results of a prospective randomized trial. Gastrointest Endosc. 1986;32:AB158. [Google Scholar]
- 15.Kozarek RA. Balloon dilation of the sphincter of Oddi. Endoscopy. 1988;20:207–210. doi: 10.1055/s-2007-1018177. [DOI] [PubMed] [Google Scholar]
- 16.May GR, Cotton PB, Edmunds SE, Chong W. Removal of stones from the bile duct at ERCP without sphincterotomy. Gastrointest Endosc. 1993;39:749–754. doi: 10.1016/S0016-5107(93)70258-8. [DOI] [PubMed] [Google Scholar]
- 17.MacMathuna P, White P, Clarke E, Lennon J, Crowe J. Endoscopic sphincteroplasty: a novel and safe alternative to papillotomy in the management of bile duct stones. Gut. 1994;35:127–129. doi: 10.1136/gut.35.1.127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.MacMathuna P, White P, Clarke E, Merriman R, Lennon JR, Crowe J. Endoscopic balloon sphincteroplasty (papillary dilation) for bile duct stones: efficacy, safety, and follow-up in 100 patients. Gastrointest Endosc. 1995;42:468–474. doi: 10.1016/S0016-5107(95)70052-8. [DOI] [PubMed] [Google Scholar]
- 19.Bergman JJGH, Rauws EAJ, Fockens P, Berkel A-M, Bossuyt PM, Tijssen JGP, et al. Randomised trial of endoscopic balloon dilation versus endoscopic sphincterotomy for removal of bile duct stones. Lancet. 1997;349:1124–1129. doi: 10.1016/S0140-6736(96)11026-6. [DOI] [PubMed] [Google Scholar]
- 20.Komatsu Y, Kawabe T, Toda N, Ohashi M, Isayama H, Tateishi K, et al. Endoscopic papillary balloon dilation for the management of common bile duct stones: experience of 226 cases. Endoscopy. 1998;30:12–17. doi: 10.1055/s-2007-993721. [DOI] [PubMed] [Google Scholar]
- 21.DiSario JA, Freeman JL, Bjorkman DJ, MacMathuna P, Peterson B, Sherman S, et al. Endoscopic balloon dilation compared to sphincterotomy (EDES) for extraction of bile duct stones: preliminary results. Gastrointest Endosc. 1997;45:AB129. doi: 10.1016/S0016-5107(97)80418-X. [DOI] [Google Scholar]
- 22.DiSario JA, Freeman JL, Bjorkman DJ, MacMathuna P, Peterson B, Sherman S, et al. Endoscopic balloon dilation vs sphincterotomy (EDES) bile duct stone removal. Digestion. 1999;59(Suppl 3):26. [Google Scholar]
- 23.DiSario JA. Endoscopic balloon dilation of the sphincter of Oddi for stone extraction in the elderly: is the juice worth the squeeze? Gastrointest Endosc. 2008;68:483–486. doi: 10.1016/j.gie.2008.03.1074. [DOI] [PubMed] [Google Scholar]
- 24.Sato H, Kodama J, Takaaki J, Tatsumi Y, Maeda T, Fijita Y, et al. Endoscopic papillary balloon dilatation may preserve sphincter of Oddi function after common bile duct stone management: evaluation from the viewpoint of endoscopic manometry. Gut. 1997;41:541–544. doi: 10.1136/gut.41.4.541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Sugiyama M, Atomi Y. Long-term effects of endoscopic papillary balloon dilation on gallbladder motility. Dig Dis Sci. 2004;49:1803–1807. doi: 10.1007/s10620-004-9574-3. [DOI] [PubMed] [Google Scholar]
- 26.Isayama H, Komatsu Y, Inoue Y, Toda N, Shiratori Y, Tsujino T, et al. Preserved function of the Oddi sphincter after endoscopic papillary balloon dilation. Hepatogastroenterology. 2003;50:1787–1791. [PubMed] [Google Scholar]
- 27.Yasuda I, Tomita E, Enya M, Kato T, Moriwaki H. Can endoscopic papillary balloon dilation really preserve sphincter of Oddi function? Gut. 2001;49:686–691. doi: 10.1136/gut.49.5.686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Gregg JA, Girolami P, Carr Locke DL. Effects of sphincteroplasty and endoscopic sphincterotomy on the bacteriologic characteristics of the common bile duct. Am J Surg. 1985;149:668–671. doi: 10.1016/S0002-9610(85)80152-5. [DOI] [PubMed] [Google Scholar]
- 29.Sand J, Airo I, Hiltunen KM, Mattila J, Nordback I. Changes in biliary bacteria after endoscopic cholangiography and sphincterotomy. Am Surg. 1992;58:324–328. [PubMed] [Google Scholar]
- 30.Greenfield C, Cleland P, Dick R, Masters S, Summerfield JA, Sherlock S. Biliary sequelae of endoscopic sphincterotomy. Postgrad Med J. 1985;61:213–215. doi: 10.1136/pgmj.61.713.213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kurumado K, Nagai T, Kondo Y, Abe H. Long-term observations on morphological changes of choledochal epithelium after choledochoenterostomy in rats. Dig Dis Sci. 1994;39:809–820. doi: 10.1007/BF02087428. [DOI] [PubMed] [Google Scholar]
- 32.MacMathuna P, Siegenberg D, Gibbons D, Gorin D, O’Brien M, Afdehal NA, et al. The acute and long-term effect of balloon sphincteroplasty on papillary structure in pigs. Gastrointest Endosc. 1996;44:650–655. doi: 10.1016/S0016-5107(96)70046-9. [DOI] [PubMed] [Google Scholar]
- 33.Weinberg BM, Shindy W, Lo S. Endoscopic balloon sphincter dilation (sphincteroplasty) versus sphincterotomy for common bile duct stones. Cochrane Database Syst Rev. 2006;4:CD004890. doi: 10.1002/14651858.CD004890.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Ito Y, Tsujino T, Togawa O, Yamamoto N, Isayama H, Nakata R, et al. Endoscopic papillary balloon dilation for the management of bile duct stones in patients 85 years of age and older. Gastrointest Endosc. 2008;68:477–482. doi: 10.1016/j.gie.2007.10.066. [DOI] [PubMed] [Google Scholar]
- 35.Toda N, Saito K, Wada R, Kawabe T, Shiratori Y, Mitsushima T, Omata M. Endoscopic sphincterotomy and papillary balloon dilation for bile duct stones. Hepatogastroenterology. 2005;52:700–704. [PubMed] [Google Scholar]
- 36.Bergman JJGHM, Berkel A-M, Bruno MJ, Fockens P, Rauws EAJ, Tijssen JGP, et al. A randomized trial of endoscopic balloon dilation and endoscopic sphincterotomy for removal of bile duct stones in patients with a prior Billroth II gastrectomy. Gastrointest Endosc. 2001;53:19–26. doi: 10.1067/mge.2001.110454. [DOI] [PubMed] [Google Scholar]
- 37.Ochi Y, Mukawa K, Kiyosawa K, Akamatsu T. Comparing the treatment outcomes of endoscopic papillary dilation and endoscopic sphincterotomy for removal of bile duct stones. J Gastroenterol Hepatol. 1999;14:90–96. doi: 10.1046/j.1440-1746.1999.01798.x. [DOI] [PubMed] [Google Scholar]
- 38.Nakagawa H, Ohara K. Safeguards against acute pancreatitis associated with endoscopic papillary balloon dilation. J Hepatobiliary Pancreat Surg. 2006;13:75–79. doi: 10.1007/s00534-005-1061-5. [DOI] [PubMed] [Google Scholar]
- 39.Tsujino T, Kawabe T, Isayama H, Sasaki T, Kogure H, Togawa O, Arisumi T, et al. Efficacy and safety of low-pressured and short-term dilation in endoscopic papillary balloon dilation for bile duct stone removal. J Gastroenterol Hepatol. 2008;23:867–871. doi: 10.1111/j.1440-1746.2007.05267.x. [DOI] [PubMed] [Google Scholar]
- 40.Vlavianos P, Chopra K, Mandalia S, Anderson M, Thompson J, Westaby D. Endoscopic balloon dilatation versus endoscopic sphincterotomy for the removal of bile duct stones: a prospective randomised trial. Gut. 2003;52:1165–1169. doi: 10.1136/gut.52.8.1165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Natsui M, Narisawa R, Motoyama H, Hayashi S, Seki K, Wakabayashi H, et al. What is an appropriate indication for endoscopic papillary balloon dilation? Eur J Gastroenterol Hepatol. 2002;14:635–640. doi: 10.1097/00042737-200206000-00008. [DOI] [PubMed] [Google Scholar]
- 42.Sugiyama M, Abe N, Izumisato Y, Masaki T, Mori T, Atomi Y. Risk factors for acute pancreatitis after endoscopic papillary balloon dilation. Hepatogastroenterology. 2003;50:1796–1798. [PubMed] [Google Scholar]
- 43.Minami A, Nakatsu T, Uchida N, Hirabayashi S, Fukuma H, Morshed SA. Papillary dilation vs sphincterotomy in endoscopic removal of bile duct stones. Dig Dis Sci. 1995;40:2550–2554. doi: 10.1007/BF02220440. [DOI] [PubMed] [Google Scholar]
- 44.Fujita N, Maguchi H, Komatsu Y, Yasuda I, Hasebe O, Igarashi Y, et al. Endoscopic sphincterotomy and endoscopic papillary balloon dilatation for bile duct stones: a prospective randomized controlled multicenter trial. Gastrointest Endosc. 2003;57:151–155. doi: 10.1067/mge.2003.56. [DOI] [PubMed] [Google Scholar]
- 45.Tanaka S, Sawayama T, Yoshioka T. Endoscopic papillary balloon dilation and endoscopic sphincterotomy for bile duct stones: long-term outcomes in a prospective randomized controlled trial. Gastrointest Endosc. 2004;59:614–618. doi: 10.1016/S0016-5107(04)00157-9. [DOI] [PubMed] [Google Scholar]
- 46.Arnold JC, Benz C, Martin WR, Adamek HE, Riemann JF. Endoscopic papillary balloon dilation vs sphincterotomy for removal of common bile duct stones: a prospective randomized pilot study. Endoscopy. 2001;33:563–567. doi: 10.1055/s-2001-15307. [DOI] [PubMed] [Google Scholar]
- 47.Bergman JJ, Tytgat GN, Huibregtse K. Endoscopic dilatation of the biliary sphincter for removal of bile duct stones: an overview of current indication and limitations. Scand J Gastroenterol Suppl. 1998;225:59–65. doi: 10.1080/003655298750027245. [DOI] [PubMed] [Google Scholar]
- 48.Baron TH, Harewood GC. Endoscopic balloon dilation of the biliary sphincter compared to endoscopic biliary sphincterotomy for removal of common bile duct stones during ERCP: a meta analysis of randomized, controlled trials. Am J Gastroenterol. 2004;99:1455–1460. doi: 10.1111/j.1572-0241.2004.30151.x. [DOI] [PubMed] [Google Scholar]
- 49.Ersoz G, Tekesin O, Ozutemiz AO, Gunsar F. Biliary sphincterotomy plus dilation with a large balloon for bile duct stones that are difficult to extract. Gastrointest Endosc. 2003;57:156–159. doi: 10.1067/mge.2003.52. [DOI] [PubMed] [Google Scholar]
- 50.Bang S, Kim MH, Park JY, Park SW, Song SY, Chung JB. Endoscopic papillary balloon dilation with large balloon after limited sphincterotomy for retrieval of choledocholithiasis. Yonsei Med J. 2006;47:805–810. doi: 10.3349/ymj.2006.47.6.805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Minami A, Hirose S, Nomoto T, Hayakawa S. Small sphincterotomy combined with papillary dilation with large balloon permits retrieval of large stones without mechanical lithotripsy. World J Gastroenterol. 2007;13:2179–2182. doi: 10.3748/wjg.v13.i15.2179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Heo JH, Kang DH, Jung HJ, Kwon DS, An JK, Kim BS, et al. Endoscopic sphincterotomy plus large-balloon dilation versus endoscopic sphincterotomy for removal of bile-duct stones. Gastrointest Endosc. 2007;66:720–726. doi: 10.1016/j.gie.2007.02.033. [DOI] [PubMed] [Google Scholar]
- 53.Attasaranya S, Cheon YK, Vittal H, Howell DA, Wakelin DE, Cunningham JT, et al. Large-diameter biliary orifice balloon dilation to aid in endoscopic bile duct stone removal: a multicenter series. Gastrointest Endosc. 2008;67:1046–1052. doi: 10.1016/j.gie.2007.08.047. [DOI] [PubMed] [Google Scholar]
- 54.Kochhar R, Dutta U, Shukla R, Nagi B, Singh K, Wig JD. Sequential endoscopic papillary balloon dilatation following limited sphincterotomy for common bile duct stones. Dig Dis Sci. 2009;54:1578–1581. doi: 10.1007/s10620-008-0534-1. [DOI] [PubMed] [Google Scholar]
- 55.Itoi T, Itokawa F, Sofuni A, Kurihara T, Tsuchiya T, Ishii K, et al. Endoscopic sphincterotomy combined with large balloon dilation can reduce the procedure time and fluoroscopy time for removal of large bile duct stones. Am J Gastroenterol. 2009;104:560–565. doi: 10.1038/ajg.2008.67. [DOI] [PubMed] [Google Scholar]
- 56.Misra SP, Dwivedi M. Large-diameter balloon after endoscopic sphincterotomy for removal of difficult bile duct stones. Endoscopy. 2008;40:209–213. doi: 10.1055/s-2007-967040. [DOI] [PubMed] [Google Scholar]
- 57.Maydeo A, Bhandari S. Balloon sphincteroplasty for removing difficult bile duct stones. Endoscopy. 2007;39:958–961. doi: 10.1055/s-2007-966784. [DOI] [PubMed] [Google Scholar]