

A number of reports have indicated that liver damage is a significant complication in recipients of renal homografts [2, 3, 6–8, 11]. Studies of patients treated at the University of Colorado Medical Center and the Denver Veterans Administration Hospital show that the incidence of posttransplantation liver injury may be even higher than has been generally believed.
Case Material
Renal homotransplantation was performed in 185 patients between March 1962 and April 1968. None of the recipients, who were aged 3 to 55 years, had known liver disease prior to transplantation, although in 39 of the earlier cases adequate biochemical tests were not obtained preoperatively to establish this fact. In the other 146, hepatic function was studied before operation and at frequent intervals afterward. With the growing realization of the high incidence of liver disease in this kind of patient, a standard profile of laboratory determinations was routinely used. The tests performed included total serum proteins, protein electrophoresis, serum bilirubin, alkaline phosphatase, serum glutamic-oxaloacetic transaminase (SGOT), serum glutamicpyruvic transaminase (SGPT), and prothrombin time. Bromsulphalein (BSP) was determined in a number of cases.
Although histopathologic specimens from the entire group will be included, the major portion of this report will be concerned with the 146 cases in which liver function was assessed before and after transplantation. Of the latter patients, 104 received kidneys from related living donors, 24 from unrelated living donors, and 18 from cadavers. All were treated with prednisone and azathioprine, and the last 66 were also given horse antihuman-lymphocyte globulin (ALG). Rejection crises were treated with increased doses of prednisone and with actinomycin C or local radiotherapy to the transplant. More than 95 % of the patients underwent bilateral nephrectomy and splenectomy at the same time as the transplantation; 30 patients also had thymectomy at some time earlier.
There were a number of other factors which were examined because of their possible role in the genesis of posttransplantation liver disease. All but 2 of the recipients were prepared for operation with hemodialysis. Blood transfusions were given at some time to every patient either before or during operation; after transplantation transfusions were rarely required. A note was also made of the type of anesthesia used, any incidence of intraoperative hypoxia or hypotension, and the many nonimmunosuppressive agents administered postoperatively. These included antihypertensive, chemotherapeutic, antibiotic, antacid, analgesic, narcotic, diuretic, laxative, and antihistaminc drugs.
Results
The Incidence and Timing of Liver Malfunction
Eighty-eight (60%) of the 146 patients completely studied with liver chemistries developed abnormalities in one or more of the tests mentioned earlier. The liver dysfunction appeared within the first 6 months after transplantation in the majority of these recipients (Fig. 1A). In most instances the changes were transient and mild, but in some they were marked and persistent.
Fig. 1.

Time of onset of liver damage.
There were 20 cases in which the hepatic disease was classified as severe as judged by the liver chemistries to be discussed below. In more than two-thirds of these patients a diagnosis of a liver complication was established within the very early postoperative period, but in a minority the evidence of hepatic damage appeared much later (Fig. 1B). Four of the 20 patients died as the direct consequence of acute hepatic failure from 5 to 18 months after transplantation; in 6 other cases a less fulminant kind of hepatic disease was an important contributory cause of death.
The Hepatic Function Abnormalities
The derangements in liver function were highly variable from case to case and were accompanied by clinical symptoms in only a small minority. For example, it was extremely common to have elevations in the serum transaminases (Fig. 2) at a time of apparent good health and in the absence of jaundice or other alarming findings. Even the appearance of hyperbilirubinemia was not necessarily a bad prognostic sign since 52 patients had icterus (Fig. 3) of 1.5 mg/100 ml or greater, but in most cases this was transient. The increased bilirubin concentration was usually a combination of the conjugated and unconjugated forms and was almost invariably accompanied by increases in alkaline phosphatase (Fig. 4).
Fig. 2.
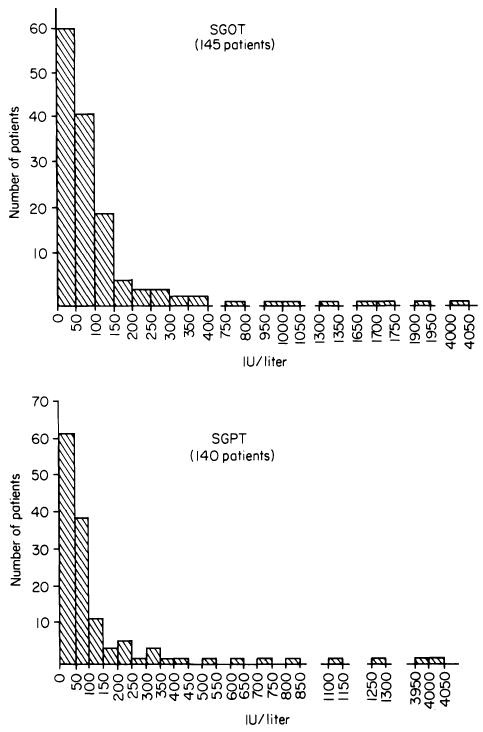
Serum glutamic-oxaloacetic transaminase (SGOT) and serum glutamic-pyruvic transaminase (SGPT) levels in renal homograft recipients. The SGOT was elevated in 59% of these patients, and the SGPT in 51 %. The normal values are less than 40 international units (IU) per liter. The levels shown here and in all the subsequent illustrations are the most abnormal observed in any given patient.
Fig. 3.

Total bilirubin was elevated above 1.0 mg/100 ml in 52 of the 143 patients studied. The normal values are less than 1.0 mg/100 ml.
Fig. 4.

Alkaline phosphatase was elevated in 65% of 132 patients after renal transplantation at some time in the postoperative course. The normal values are 14–38 IU.
There were often declines in serum protein concentrations, sometimes to extraordinarily low levels (Fig. 5). However, the significance of these changes in relation to liver disease was frequently difficult to analyze because of the complex clinical situation. Thus, some of these patients had persistent proteinuria as a contributory factor, and in many others important underlying causes were poor diet or high dose steroid therapy. Nevertheless, a hepatic etiology was undoubtedly at least partially responsible in some since there were also coincident depressions in the prothrombin time (Fig. 6) and a number of the same patients had marked BSP retention (Fig. 7); there was a more than 5% BSP retention in 31 of the 39 patients in which it was determined.
Fig. 5.

Total serum proteins were markedly reduced in most patients. The values given are the lowest ever observed in any given case. (A) Total. (B) Albumin.
Fig. 6.

Prothrombin times were below 40% at some time in 22 of the 119 patients in which it was estimated.
Fig. 7.

Bromsulphalein (BSP) retention of greater than 6% after 45 minutes was observed in 31 of 39 patients in which this test was performed. The abnormal values usually improved with the passage of time.
The Effect of ALG Therapy on Liver Disease
Fifty-two (65 %) of the 80 patients treated with azathioprine and prednisone before June, 1966, developed evidence of liver damage. All 4 of the fatalities caused by acute hepatic failure were in this group.
In the next 2 years, horse ALG was used as an adjuvant immunosuppressive agent in combination with reduced doses of azathioprine and prednisone [12].
Thirty-six (54 %) of the 66 patients treated in the latter period also had some findings of hepatic damage, but generally to a less severe degree and never with a fatal outcome. Consequently, it has been our conclusion that the magnitude of the problem has been distinctly less since the addition of ALG to the immunosuppressive regimen.
Histopathologic Findings
Forty-two livers were studied either at autopsy or as the result of needle biopsies during life. The overall impression was that the more severe histologic findings were in the patients who had manifested the most marked derangements in liver function.
The finding of increased iron associated with diastase-resistant periodic acid-Schiff-positive granules in hepatocytes and Kupffer cells described by Hill et al. [5] was confirmed in almost all cases. The accumulations of iron were very large in 6 cases and not associated with other prominent changes.
Significant fatty metamorphosis was present in 18 of the livers; it was mild to moderate in 10 and severe in 8. It was often associated with nonspecific degenerative changes in hepatocytes or variable central necrosis. Slight bile stasis without other signs of severe liver injury was found in 5 instances. In 17 other autopsy cases, the same nonspecific pattern of injury was present but the frequency and severity of the lesions were lower.
Massive hepatic necrosis consistent with viral hepatitis was present in 4 livers. Moderate to severe central necrosis not accompanied by passive congestion was found in 5 other cases, and was accompanied by bile stasis in one. The cause of this injury was not apparent; it may have represented a milder form of massive necrosis. A variable degree of portal fibrosis was found in 3 cases, and in many others there was a scant to moderate infiltrate of chronic inflammatory cells in the portal triads. One case demonstrated typical post-hepatitic cirrhosis.
In contrast to the great frequency and severity of pulmonary infections in these patients, lesions attributable to infectious disease other than viral hepatitis were rare. There were 3 livers which contained the inclusions of cytomegalovirus. One case of hepatic histoplasmosis and one of hepatitis caused by a toxoplasma-like organism were found. Minute foci of hepatic necrosis without demonstrable organisms were seen in 2 cases. One patient with widespread reticulum cell sarcoma had multiple tumor masses in the liver.
Discussion
The data from this series indicate that detectable liver damage occurs in the majority of patients after renal homotransplantation. Unfortunately, it may be impossible to determine the etiology of the hepatic dysfunction in any given case. It seems likely that the causative factors are variable.
A significant number of these patients were probably the victims of viral hepatitis. Statistically, the renal transplant recipient should be at high risk from this kind of infectious complication since he is usually exposed to multiple blood transfusions as well as extracorporeal hemodialysis before operation. Hampers et al. [4] found that 7 % of nontransplantation patients who received one pint of blood and virtually all of those who received 6 or more transfusions developed anicteric hepatitis. It might be speculated that because of the immunosuppression and immunologic crippling imposed on the transplant recipient he would be prone to exhibit more serious manifestations of the disease.
The foregoing explanation for posttransplantation “hepatitis” could be well supported in a number of cases in this series. First, the onset of liver dysfunction often, although not invariably, occurred within the known incubation period (approximately 100 days) of serum hepatitis. Second, the clinical presentation and pathologic findings were often highly suggestive of this diagnosis. Finally, 4 members of the surgical staff who cared for these patients developed the same disease at about the same time or slightly afterward. The propensity of the liver to develop infectious complications during intensive immunosuppression can also be illustrated by the fact that several of the organs examined histopathologically had evidence of invasion by cytomegalovirus or fungi.
It is highly unlikely, however, that viral hepatitis or other infections can be indicted as the universal cause of the liver dysfunction after renal homotransplantation, as was emphasized by Hamburger et al. [3] and in earlier publications from our own institutions [8, 11]. It is well known from animal research that both azathioprine and prednisone can cause liver injury [9, 10] although the extrapolation of this kind of information to man has not been well supported by the kind of pathologic studies carried out by Hill, Porter, and Massion [5]. Nevertheless, it was pointed out above that the majority of hepatic complications occur during the first several postoperative months at a time when the most stringent immunosuppressive treatment is required to prevent rejection. A situation of double jeopardy may result not only from unmasked viral infection, but also from the inherent hepatotoxicity of the drugs.
Other pharmacological agents often used in the care of these patients have also been on occasion reported to cause liver injury. These include the antihypertensive drug α-methyl-DOPA (Aldomet) and the antibiotics tetracycline, prostaphlin, methicillin, ampicillin, gantrisin, and amphoteracin B [1]. In addition some of the anesthetics used for these patients apparently can cause hepatic damage. Of the latter halothane has received the most attention, but there were no instances in our series in which the use of this or other anesthetic agents was followed by acute liver injury.
Vague though the conclusions may be about the presumed multiple etiologies of liver disease in patients receiving renal homografts under immunosuppressive therapy, it is crucial for obvious practical reasons to have an idea of the frequency of this kind of complication before embarking on trials of liver transplantation. With the latter procedure the differential diagnosis and proper management could become hopelessly confused by the coexistence of hepatic rejection and liver injury from other causes. The present study has demonstrated the number of times with which this perplexing picture may potentially have to be dealt.
With the onset of jaundice in renal homograft recipients, it may not be necessary to make adjustments in the immunosuppressive therapy providing the hepatic complication is not too severe or protracted. If, however, the liver disease is major and prolonged, it is often advisable to reduce the vigor of treatment, especially of azathioprine, and to accept the possible risk of homograft repudiation.
There are two reasons for this. First, it was noted several years ago [11] that the hyperbilirubinemia in such patients tended to decrease coincident with reductions in azathioprine dosage. Second, patients with serious hepatic injury are much more apt to develop bone marrow depression, presumably because the hepatic pathway of detoxification of azathioprine is partially lost. Efforts to continue preexisting doses of azathioprine may therefore be dangerous.
Summary
Liver damage in renal homotransplant recipients is more common than is generally believed. It occurred in 60% of 146 patients studied and was severe in 13.7 %. Common causes of liver damage are viral hepatitis and/or the use of immunosuppressive and other potentially hepatotoxic drugs. The incidence of major liver complications has been less since the introduction of horse antihuman-lymphocyte globulin as an adjuvant immunosuppressive agent.
Footnotes
Supported by United States Public Health Service grants AM-06344, HE-07735, AM-07772, AI-04152, FR-00051, FR-00069, AM-12148, and AI-AM-08898.
References
- 1.Goodman LS, Gilman A. The Pharmacological Basis of Therapeutics. 3rd. Macmillan; New York: 1967. p. 572.p. 1145.p. 1210.p. 1211.p. 1212.p. 1242.p. 1294. [Google Scholar]
- 2.Hamburger J, Crosnier J, Dormont J. Experience with 45 renal homotransplantations in man. Lancet. 1965;1:985. doi: 10.1016/s0140-6736(65)91218-3. [DOI] [PubMed] [Google Scholar]
- 3.Hamburger J, Crosnier J, Dormont J, Reveillaud RJ, Hors JH, Alsina J. Homotransplantation renale humaine. III. Complications extra-rénales. Presse Med. 1965;73:2911. [PubMed] [Google Scholar]
- 4.Hampers L, Prager D, Senior JR. Post-transfusion anicteric hepatitis. New Eng J Med. 1964;271:747. doi: 10.1056/NEJM196410082711501. [DOI] [PubMed] [Google Scholar]
- 5.Hill RB, Jr, Porter KA, Massion CG. Hepatic reaction to renal transplants modified by immunosuppressive therapy. Iron accumulation in hepatic injury. Arch Path (Chicago) 1966;81:71. [Google Scholar]
- 6.Hume DM. Progress in clinical renal homotransplantation. Advances Surg. 1966;2:419. [PubMed] [Google Scholar]
- 7.Merrill JP. Human tissue transplantation. Advances Immun. 1967;7:275. doi: 10.1016/s0065-2776(08)60130-3. [DOI] [PubMed] [Google Scholar]
- 8.Starzl TE. Experience in Renal Transplantation. Saunders; Philadelphia, Pennsylvania: 1964. [Google Scholar]
- 9.Starzl TE, Marchioro TL, Porter KA. Progress in homotransplantation of the liver. Advances Surg. 1966;2:295. [PMC free article] [PubMed] [Google Scholar]
- 10.Starzl TE, Marchioro TL, Porter KA, Taylor PD, Faris TD, Herrman TJ, Hlad CJ, Waddell WR. Factors determining short and long term survival after orthotopic liver homotransplantation in the dog. Surgery. 1965;58:131. [PMC free article] [PubMed] [Google Scholar]
- 11.Starzl TE, Marchioro TL, Terasaki PI, Porter KA, Faris TD, Herrman TJ, Vredevoe DL, Hutt MP, Odgen DA, Waddell WR. Chronic survival after human renal homotransplantation. Ann Surg. 1965;162:749. doi: 10.1097/00000658-196510000-00016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Starzl TE, Porter KA, Iwasaki Y, Marchioro TL, Kashiwagi N. The use of antilymphocyte globulin in human renal homotransplantation. In: Wolstenholme GEW, O'Connor M, editors. Antilymphocytic Serum. Churchill; London: 1967. pp. 4–34. [Google Scholar]