

Abstract
Pericardial cysts are uncommon congenital abnormalities that occur in the middle mediastinum. Most of these are found incidentally on chest x-rays. The occurrence of pericardial cyst in children is quite rare. It needs to be differentiated from other cystic mediastinal masses. A rare case of pericardial cyst in a 5 year old male child is reported. The child presented with chest pain, cough and fever. The preoperative diagnosis of pericardial cyst was suggestive on echocardiography and CT scan. It was confirmed on histopathology after successful surgical excision. The rarity of this benign mediastinal lesion in children prompted us to report this case.
Keywords: Pericardial cyst, mediastinal mass, cardiac tumors
INTRODUCTION
Pericardial cysts are benign congenital mediastinal lesions that result from either abnormal fusion or failure of fusion of the primitive mesenchymal pericardial lacunae that normally fuse to form a pericardial sac in the embryo.[1,2] They are commonly reported in middle-aged adults, most frequently in the third or fourth decades of life, and have rarely been encountered in the childhood.[1] These occur equally among men and women. There have been about 20 reported cases of pericardial cysts presenting before the age of 18 years, with only a few cases being reported in the age group of up to 5 years.[3] The overall incidence of pericardial cyst is 1:1,00,000 in all age groups.[4] These constitute only 6% of all mediastinal masses and up to 11% of all mediastinal cysts.[1,5,6] Most of the cases of these cysts are asymptomatic, and are found incidentally during routine chest radiography or echocardiography.[7] The clinical presentation is variable and can range from asymptomatic patients (75%) in whom the diagnosis is incidental to those with complaints such as pain or heaviness in the chest, difficulty in breathing or cough.[7]
CASE REPORT
A 5-year-old male child presented with history of dull aching chest pain for the last 3 months. It was associated with low-grade intermittent fever and nonproductive cough for the last 20 days. The child's birth history was uneventful, with a birth weight of 2.8 kg, and he was fully immunized as per the schedule. On examination, the patient was sick and pale, with a pulse rate of 136/min. The respiratory system examination revealed bilaterally clear chest. On precordial examination, the heart sounds were soft and feeble. An abdominal examination revealed palpable liver, which was 5 cm below the costal margin. On hematological investigation, hemoglobin was 10.5 gm%, with a white blood cell count of 6.0 × 109/l and a platelet count of 350 × 109/l. The chest radiograph revealed widened mediastinum. An echocardiography suggested a large cystic lesion occupying the anterior mediastinum and compressing both the right and left ventricles and the right atrium. On contrast-enhanced computed tomography (CECT), a large cystic mass in the middle mediastinum was identified. It was seen extending from just above the arch of the aorta and up to the diaphragm. The cyst was displacing the great vessels, trachea and heart posteriorly [Figure 1]. Both the lung fields were clear and the heart chambers were normal in size, but were compressed posteriorly. The differential diagnoses of thymic cyst, lymphangioma, hydatid cyst and pericardial cyst were considered. The cyst was excised by median sternotomy. A large pericardial cystic structure measuring approximately 10.0 cm × 9.5 cm × 9.0 cm was seen loosely adherent to the pericardium [Figure 2]. Its outer surface was glistening and was filled with clear fluid. Histopathological examination revealed the structure of a cyst lined with flattened mesothelial cells suggestive of pericardial cyst. The postoperative period was uneventful and the patient is doing well in follow-up.
Figure 1.
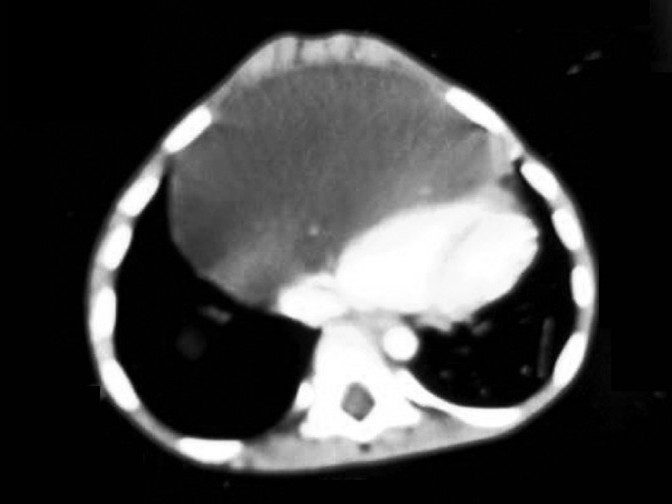
CT scan showing a huge pericardial cyst in the anterior mediastinum displacing the heart
Figure 2.

Intraoperative photograph revealing a large pericardial cyst with a glistening outer surface
DISCUSSION
Pericardial cysts are uncommon mediastinal abnormalities that are usually congenital but may also be acquired after a cardiothoracic surgery.[8] They may occur in patients of all ages, but commonly present in adults. These are quite rare in childhood and are mostly asymptomatic. Symptoms, if present, are usually because of compression by the cystic mass. Chest pain, dyspnea and paroxysmal tachypnoea are the most common symptoms that are found in 25-30% of the patients.[1] Other symptoms a patient may report are epigastric fullness, airway obstruction, asthma, venous obstruction, etc. However, cyst rupture, cardiac compression, atrial fibrillation and even sudden death have been reported.[5] These lesions are usually detected on a chest radiograph performed for some other cardiopulmonary reasons. These intrathoracic masses on chest radiographs appear as cardiomegaly.
Radiographically, these cysts abut the cardiac contours and are smooth-walled, round or irregularly shaped, with homogenous internal density. Once suspected, the diagnosis can be established using noninvasive techniques. The imaging studies helpful in diagnosis are echocardiography, computed tomography (CT) scan and magnetic resonance imaging. Transesophageal echocardiography is useful in identifying the exact location of a pericardial cyst and in differentiating a cyst from other lesions like fat pad, ventricular aneurysm, aortic aneurysm or a tumor.[5] A CT scan has been the modality of choice for diagnosis and follow-up. It can establish the cystic nature of a mediastinal mass but neither establish a pathological diagnosis nor, always, differentiate a pericardial cyst from other benign cysts of foregut origin, thymic cysts and cystic hygromas.[2]
However, the diagnosis can be especially difficult if the lesion occurs outside the typical location, at the right cardiophrenic angle or when the lesion is extensive and confluent with mediastinal structures, which is rare.[1]
Pericardial cysts are most frequently located at the right cardiophrenic angle (70%), 22% in the left; however, they can occur throughout the mediastinum.[7] These are typically soft and unilocular, but may be multilocular, with a diameter of 1–5 cm.[1] These are usually spherical or teardrop shaped, which may be attached to the pericardium directly or by a pedicle, but do not communicate with the pericardial space. The gross appearance of the excised pericardial cysts is banal, being represented by thin fibrous-walled structures that collapse completely when opened. Their internal surfaces are uniformly smooth and contain serous fluid; therefore, called spring water cysts. Histopathologically, the cyst wall is lined by a flat or cuboidal layer of mesothelium.[5]
The differential diagnoses of the pericardial cyst that should be considered clinically include teratoid cyst and tumor, cystic hygroma, lymphangioma, angioma, lipoma, neurogenic tumor, sarcomas, lymphoma, thymic lesions, cysts of foregut origin (bronchogenic cysts, esophageal duplications), bronchogenic carcinoma, metastases, granulomatous lesion and abscess, besides other diseases, such as diaphragmatic hernia, and aneurysms of the heart or great vessels.[1] However, the final diagnosis is confirmed by a histopathological examination of the cyst. Adult polycystic kidney disease has been associated with the formation of cysts in the extra-renal tissues all over the body.[6]
Asymptomatic patients with pericardial cysts should be managed conservatively.[1,2] Treatment is required in symptomatic patients or in those with unclear diagnosis. The indications for resection of pericardial cysts are large size, symptoms, uncertainty of malignant potential and prevention of life-threatening emergencies. The various treatment modalities include percutaneous aspiration of cyst, ethanol sclerosis, surgical resection or video-assisted thoracoscopic surgery (VATS).[1,4,5] Currently, VATS is the approach most commonly used in practice.[4] It has many advantages over open procedures like better cosmosis, improved intraoperative visualization, short postoperative recovery and reduced pain. But, in our case, median thoracotomy was performed as the facility for VATS was not available at our institute. If undiagnosed and untreated, the patient may present with complications like cardiac temponade leading to heart failure, respiratory distress, cyst rupture leading to pleural and pericardial effusion and sudden death etc. In cases of life-threatening presentations, cyst aspiration or emergency thoracotomy may also be required.
CONCLUSION
This case of a giant pericardial cyst in a 5-year-old child is being presented to highlight the fact that the diagnosis of pericardial cyst should be kept in mind,in any anterior intrathoracic cystic lesion even though it is very rare in children. Surgical excision becomes mandatory when these pericardial cysts cause ventilatory and/or hemodynamic impairment.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Nina VJ, Manzano NC, Mendes VG, Salgado FN. Giant pericardial cyst: Case report. Rev Bras Cir Cardiovasc. 2007;22:349–51. doi: 10.1590/s0102-76382007000300013. [DOI] [PubMed] [Google Scholar]
- 2.Daskalopoulos DA, Kuhn JP, Gingell RL, Pieroni DR. Diagnosis of Pericardial Cyst in a young child by computed tomography of the thorax. Tex Heart Inst J. 1983;10:63–5. [PMC free article] [PubMed] [Google Scholar]
- 3.Noyes BE, Weber T, Vogler C. Pericardial cysts in children: Surgical or conservative approach? J Pediat Surg. 2003;38:1263–5. doi: 10.1016/s0022-3468(03)00285-9. [DOI] [PubMed] [Google Scholar]
- 4.Eto A, Arima T, Nagashima A. Pericardial cyst in a child treated with video-assisted thoracoscopic surgery. Eur J Pediatr. 2000;159:889–91. doi: 10.1007/pl00008362. [DOI] [PubMed] [Google Scholar]
- 5.Ozturk E, Aparci M, Haholu A, Sonmez G, Mutlu H, Basekim CC. Giant, dumbbell- shaped pericardial cyst. Tex Heart Inst J. 2007;34:386–7. [PMC free article] [PubMed] [Google Scholar]
- 6.Liaquat HB, Ali L, Ara J. Pericardial cyst: A rare congenital anomaly. Pak J Med Sci. 2009;25:1018–20. [Google Scholar]
- 7.Varghese TK, Lau CL. Sabiston Textbook of Surgery: The Biological basis of modern surgical practice. In: Townsend CM, Beauchamp RD, Evers BM, Mattox KL, editors. The mediastinum. 18th ed. Philadelphia: Saunders; 2008. p. 1695. [Google Scholar]
- 8.Patel J, Park C, Michaels J, Rosen S, Kort S. Pericardial cyst: Case reports and a literature review. Echocardiography. 2004;21:269–72. doi: 10.1111/j.0742-2822.2004.03097.x. [DOI] [PubMed] [Google Scholar]