

Abstract
Objective:
To study the prevalence of obesity and overweight among school children in Puducherry. To identify any variation as per age, gender, place of residence and type of school.
Setting and design:
Secondary data analysis of a school-based cross sectional study in all the four regions of Puducherry.
Materials and Methods:
Children between 6 and 12 yrs were sampled using multistage random sampling with population proportionate to size from 30 clusters. Anthropometric data (BMI) was analyzed using CDC growth charts. Data was analyzed using SPSS, BMI (CDC) calculator, CI calculator and OR calculator.
Results:
The prevalence of overweight (≥85th percentile) among children was 4.41% and prevalence of obesity (>95th percentile) was 2.12%. Mahe region had the highest prevalence of overweight (8.66%) and obesity (4.69%). Female children from private schools and urban areas were at greater risk of being overweight and obese.
Conclusions:
Childhood obesity is a problem in Puducherry and requires timely intervention for its control.
Keywords: Childhood obesity, overweight, Puducherry, school children
Introduction
Many countries in South-East Asia including India are going through an economic and nutrition transition.(1) The nutrition transition is associated with a change in dietary habits, decreasing physical activity and rising prevalence of obesity.(2) Overweight and obesity are major risk factors for a number of chronic diseases, including diabetes, cardiovascular diseases and cancer. Obesity in children and adolescents is gradually becoming a major public health problem in many developing countries, including India.(3) ‘One-half of obese school children become obese adults. However, whether or not obesity persists into adulthood, obesity in childhood appears to increase the risk of subsequent morbidity′.(4–6) Significance of estimating prevalence of childhood obesity thus cannot be overemphasized.
There are a few studies, reporting, prevalence of childhood and adolescent obesity and overweight from different parts of India (Punjab, Maharashtra, Delhi and South India) that range from 3% to 29%, and also indicate that the prevalence is higher in urban than in rural areas.(7) However, there is no published data on a representative sample from Puducherry on prevalence of childhood obesity. With recent rise in number of diabetics (5.04%)(8) and hypertensives in the Union Territory of Puducherry, it was necessary to have the accurate data on prevalence of childhood obesity and therefore an attempt was made to assess the prevalence of overweight and obesity among school children aged between 6 and 12 yrs. It was also decided to study any differences in prevalence based on age group, gender, place of residence (regions or urban/ rural) and place of study (Government / private school).
Materials and Methods
This study incorporates secondary analysis of anthropometric measurements of school children aged between 6 and 12 years obtained while carrying out a survey among them for prevalence of iodine deficiency disorders (IDDs) sponsored by Directorate of Health Services, Puducherry. The details of the materials and methods are as follows. (Although the primary study outcome was to study the burden of IDD among school children, the investigators performed a complete school health check-up as part of their study protocol).(The IDD study was not published at the time of submission of present study)
General settings
The Union Territory of Puducherry encompasses an area of 480 sq km with 4 districts/regions namely, Puducherry (Pondicherry) and Karaikal (within the state of Tamil Nadu), Mahe (within the state of Kerala) and Yanam (within the state of Andhra Pradesh).
Reference population
The population of Union Territory of Puducherry in 2001(9) was 9,73,829 of which 4,86,705 were Males. Puducherry district had highest population of 735,004 followed by Karaikal (170,640), Mahe (36,823) and Yanam (31,362). 66.57% of total population is urban. Mahe and Yanam districts are purely urban.(10)
The Union Territory has 263 villages/wards.(10) There are 379 (63.38%) Government and 219 (36.62%) private schools (primary, middle and secondary) having 1,50,747 students studying from 1st to 7th standard majority being in the age group of 6-12 yrs as per census data of 2005 -2006.(9)
Study population and study area
A total of 12,685 children in the age group of 6-12 years, studying in class I-VII, from government and private schools of urban as well as rural areas in each of the four districts were enlisted initially, from which the study sample was selected as mentioned below.
Study design
Secondary data analysis of a cross-sectional study was done.
Period of study
November 2008-March 2009.
Sample size
The sample size studied in IDD study was 2940 based on revised guidelines.(11,12) The study sample had sufficient power to estimate the prevalence of childhood obesity at 95% confidence interval (CI), with expected frequency of childhood obesity being 7.3% and worst acceptable result of 8.4% (expected frequency figures based on a dissertation study carried out in the department).
Selection of study sample [Figure 1]
Figure 1.
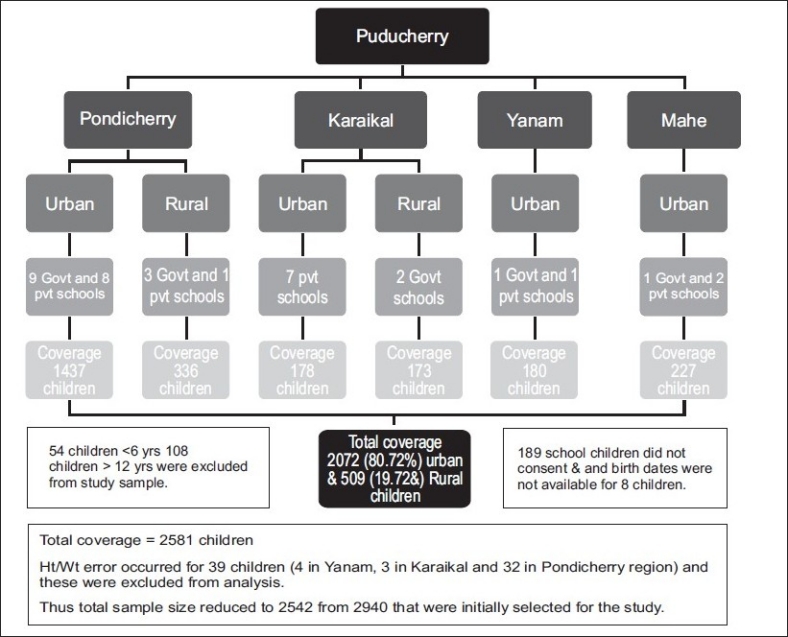
Flow chart for sample covered in union territory of Puducherry
Sampling method: Multistage sampling with population proportionate to size (PPS) was used.
Stage 1: Methodology for selection of survey sites by PPS sampling
Sampling frame comprised of cumulative population of each village/ward (cluster) of four districts. A total of 30 units (21 in Puducherry, 4 in Karaikal, 3 in Mahe and 2 in Yanam) were selected by systematic sampling using PPS.
Stage 2: Selection of school from each cluster
A ward/village-wise list of all schools (Primary, middle and secondary schools) showing total number of children was prepared and one school from each cluster was selected randomly.
Stage 3: Selection of school children from each school
Ninety-eight children (49 boys and 49 girls) aged 6-12 years studying in Classes I to VII were selected from each school, from the attendance register by systematic random sampling technique with equal representation in each age/gender category. Written consent for carrying out IDD study and general check up was obtained from the parents of the selected students 1 day prior to the survey with the help of Principal/Teachers of the school.
Exclusion criteria
All children found to be < 6, > 12 yrs of age, children whose exact birth date was not available, children without written informed consent and those with Ht/Wt error during data management were excluded from the data analysis.
Instrument and techniques
A predesigned and pretested interviewer administered questionnaire was used to collect information. A weighing (bathroom) scale and stadiometer were used to measure the weight (nearest 0.5 kg) and height (nearest 0.1 cm) of each child using standard procedure.(13) BMI was calculated as weight (kg)/height2 (m2). Sex- and age-specific percentile cut-points of a reference population (85th percentile for overweight and 95th percentile for obesity) were used.(14) The date of birth of each child was taken from the school records. Data was collected by a team of two interns (male/female) adequately trained and under the supervision of one faculty/junior resident.
Definition of overweight and obesity
Children were categorized into three groups: obese (>95 th percentile), overweight (≥85th percentile) and normal (<85th percentile,> 5th percentile) using age- and sex-specific percentiles of BMI.(14)
Statistical analysis
Data were analyzed using Statistical package for the Social Sciences (version 16.0). The prevalence of overweight and obesity were calculated using BMI for age/gender percentiles derived through child and teen BMI calculator developed by CDC Atlanta.(15) Odds ratio (OR) and CI calculator was used to calculate OR and 95% CI.(16,17) For all statistical tests, P < 0.05 was taken as the significance level.
Ethical considerations
The study had ethical clearance. Written informed consent was also obtained. A prior permission by Director of health and family welfare as well as Director of education, Government of Puducherry was accorded to conduct the primary survey and the same was also intimated to all the school Principals. Permission was also obtained from Director of Health and Family welfare regarding reporting the findings of secondary data analysis.
Financial details
The IDD study was sponsored by Department of Health, Government of Puducherry under the National Iodine Deficiency Disorders Control Programme (NIDDCP) and supported by Department of Education, Puducherry.
Results
Initially 2940 school children were selected from 30 schools [16 (53.33%) Government schools] in all the four districts of Puducherry. Subsequently, after applying the exclusion criteria, sample size reduced to 2542 children consisting of 1345 (52.11%) male children. 80.28 % were from urban areas. Overall boys and girls were equally distributed in each age and gender (male: female ratio of 1.09:1) group. However, age group 12 had less children because 108 children had to be excluded from data analysis as they were >12-years-old [Figure 1].
Table 1 shows the prevalence of overweight and obesity by age among school children in Puducherry. Prevalence of overweight and obesity was highest (7.89% and 3.8%, respectively) in age group 11. Using χ2 for linear trend, Prevalence of overweight in age group 9 was 2.81 times more whereas in the age group 11 was 4.41 times more as compared to that among children belonging to age group 6. Similar inference could not be drawn for obese children as the distribution of obesity in various age groups was not found to be statistically significant (P= 0.5272).
Table 1.
Prevalence of overweight and obesity by age among school children in Puducherry
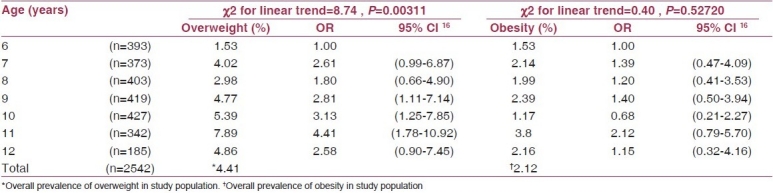
Table 2 shows overall prevalence of overweight and obesity by gender and regions among schoolchildren in Puducherry. The overall prevalence of overweight (≥85th percentile) among children was 4.41% (95% CI: 3.67, 5.27) and prevalence of obesity (>95th percentile) was 2.12% (95% CI: 1.63, 2.76). Prevalence of overweight and obesity was 4.24% (95% CI: 3.28, 5.47)(17) and 1.97 % (95% CI: 1.35, 2.87),(17) respectively, among males whereas prevalence of overweight and obesity among females was 4.58 % (95% CI: 3.55, 5.90)(17) and 2.29 % (95% CI: 1.59, 3.29)(17) respectively. Among all the four regions, Mahe had the highest prevalence of overweight (8.66%) and obesity (4.69%).
Table 2.
Prevalence of overweight and obesity by gender and region among school children in Puducherry
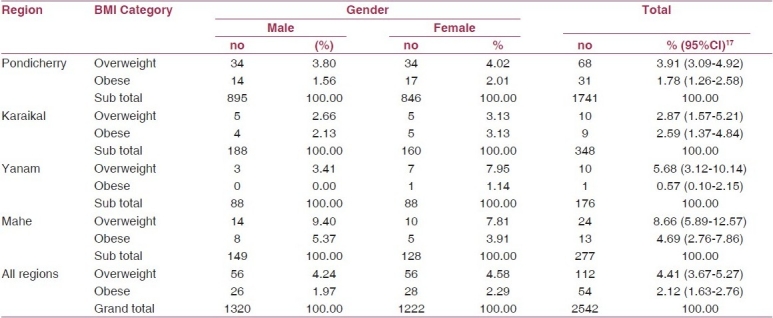
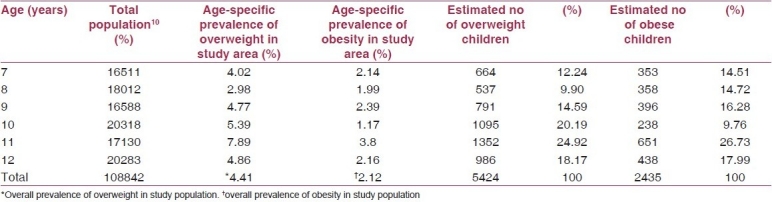
Table 3 shows the estimated number of overweight and obese children between 7 and 12 yrs of age in Puducherry based on 2001 census data for the state. As we could not ascertain the number of children aged 6 yrs separately we therefore excluded this group while estimating the true prevalence of Union Territory of Puducherry. In a population of 1,08,842, between 7 and 12 yrs there are 5424 overweight and 2435 obese children using the prevalence estimate of 4.41% and 2.12%, respectively. The largest numbers of overweight (1352) and obese (651) children belong to age group 11 yrs. The estimated true prevalence of overweight among children (7-12 yrs) was 4.98% and that of obesity was 2.24%.
Table 3.
Estimated number of overweight and obese children based on census data, 2001, by age-specific prevalence rates of study population
Discussion
It is emerging convincingly that the genesis of Type 2 Diabetes and Coronary Heart Disease begins in childhood, with childhood obesity serving as an important factor.(18) There has been a phenomenal rise in proportions of children having obesity in the last 4 decades especially in the developed world. Studies emerging from different parts of India(19–24) within last decade are also indicative of similar trend.
In the present study the true prevalence of overweight and obesity was 4.98% and 2.24% respectively. Mahe region surrounded by Kerala reported the highest prevalence of overweight [8.66%] and obesity [4.69%]. A similar finding was reported from another study in Kerala(19) that showed an increased prevalence of overweight and obesity from 4.94% and 1.26% in 2003 to 6.57% and 1.89% in 2005 with particular rise in the age group 5-11 yrs. Yanam surrounded by Andhra Pradesh had 2nd highest prevalence of overweight [5.68%], and lowest prevalence of obesity [0.57%]. A similar study among adolescents in Hyderabad(20) reported prevalence of overweight of 7.2% (95% CI: 5.7, 8.7). In Puducherry and Karaikal regions surrounded by TamilNadu, the prevalence of overweight and obesity ranged from 2.87% to 3.91% and 1.78% to 2.59%, respectively [Table 2]. A study carried out in urban school of Chennai,(21) Tamil Nadu, reported a high prevalence of overweight (8.0-10.81%) and obesity (5.26-9.52%). By and large each region from the Union Territory of Puducherry showed trends similar to the respective surrounding states indicating a strong influence of local environmental and sociocultural factors on the pattern of overweight and obesity found in these children.
Our study showed higher prevalence of overweight and obesity among females in all the regions of Puducherry except Mahe where reverse trend was seen. These findings were in concordance to that reported from other studies within the respective states that surrounded each of these four regions.(19–21). Females are more likely to be obese as compared to males, owing to inherent hormonal differences.(25)
Prevalence of overweight and obesity was 5.07% (9%5 CI: 4.20-6.11)(17) and 2.61 %(95% CI: 2.00-3.40),(17) respectively, among children residing in urban areas, higher than those in rural areas with reported prevalence for overweight and obesity of 1.76 % (95% CI: 0.93-3.32)(17) and 0.2 % (95% CI: 0.03 to 1.10),(17) respectively. Children from urban areas were 3.04 times (95% CI: 1.52-6.09)(16) and 14.10 times (95% CI: 1.94-102.38)(16) at greater risk of being overweight andobese compared to children in rural areas. Similar trend was observed in other studies.(19–20)
It was observed that prevalence of overweight and obesity was 2.84% (95% CI: 2.09-3.86)(17) and 1.82 %(95% CI: 1.24-2.68),(17) respectively, among children studying in Government schools, whereas it was found to be higher among children studying in private schools, being 6.23% (95% CI: 4.99-7.77)(17) and 2.48 % (95% CI: 1.73-3.53),(17) respectively. Children from private schools were 1.71 times (95% CI: 1.14-2.56)(17) and 1.06 times (95% CI: 0.61-1.83)(17) at greater risk of being overweight and obese, respectively, compared to children in Government schools. Similar trend was also observed in other studies.(19–20) These findings suggest that children belonging to relatively higher socioeconomic strata who are likely to study in private schools and reside in urban areas , are at higher risk of obesity, most likely due to associated lifestyle changes leading to inappropriate diet and increasing levels of physical inactivity.
Thus area of residence, socioeconomic conditions and age/gender differences were felt to be important contributors towards overweight and obesity in our study population. Our study had some limitations like nonschool going children were not studied and only one school was selected per cluster. Besides, risk factors for childhood obesity could not be directly studied as this information was not specifically sought for in the original study. However, strength of our study remains in the fact that it provides an overview of burden of childhood obesity among representative sample of children between 6 and 12 yrs for the first time and can prove to be a benchmark for future comparisons by the public health personnel and decision makers. It also indicates the need to devise meaningful control measures, both home and school-based pending, further research on risk factors for childhood obesity and also to monitor the trend in near future considering the alarming rise in the number of diabetics and hypertensive within the state in recent past.
Footnotes
Source of Support: None declared
Conflict of Interest: None declared.
References
- 1.Shetty PS. Nutrition transition in India. Public Health Nutr. 2002;5:175–82. doi: 10.1079/PHN2001291. [DOI] [PubMed] [Google Scholar]
- 2.Popkin BM. The nutrition transition in low-income countries: An emerging crisis. Nutr Rev. 1994;52:285–98. doi: 10.1111/j.1753-4887.1994.tb01460.x. [DOI] [PubMed] [Google Scholar]
- 3.Popkin BM, Doak CM. The obesity epidemic is a worldwide phenomenon. Nutr Rev. 1998;56:106–14. doi: 10.1111/j.1753-4887.1998.tb01722.x. [DOI] [PubMed] [Google Scholar]
- 4.Must A, Strauss RS. Risks and consequences of childhood and adolescent obesity. Int J Obes Relat Metab Disord. 1999;23:S2–11. doi: 10.1038/sj.ijo.0800852. [DOI] [PubMed] [Google Scholar]
- 5.Gidding SS, Bao W, Srinivasan SR, Berenson GS. Effects of secular trends in obesity on coronary risk factors in children: The Bogalusa Heart Study. J Pediatr. 1995;127:868–74. doi: 10.1016/s0022-3476(95)70020-x. [DOI] [PubMed] [Google Scholar]
- 6.Chu NF, Pan WH. Prevalence of obesity and its comorbidities among schoolchildren in Taiwan. Asia Pac J Clin Nutr. 2007;16:601–7. [PubMed] [Google Scholar]
- 7.Kaur S, Kapil U, Singh P. Pattern of chronic diseases amongst adolescent obese children in developing countries. [Last cited 2009 Dec 27];Curr Sci. 2005 88:1052–6. Available from: http://www.ias.ac.in/currsci/apr102005/1052.pdf . [Google Scholar]
- 8.Purty AJ, Vedapriya DR, Bazroy J, Gupta S, Cherian J, Vishwanathan M. Prevalence of diagnosed diabetes in an urban area of Puducherry, India: Time for preventive action. [Last cited 2009 Dec 27];Int J Diab Dev Ctries. 2009 29:6–11. doi: 10.4103/0973-3930.50708. Available from: http://www.ijddc.com/text.asp?2009/29/1/6/50708 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Statistics. puducherry.gov.in Puducherry, Directorate of Economics and Statistics. [Last cited 2009 May 23]; Available from: http://statistics.puducherry.gov.in/ [Google Scholar]
- 10.Vaittianadane S. Figures at a glance. In: Vaittianadane S, editor. Statistical Handbook,2001-2002. Pondicherry: Publication section Directorate of Economics and Statistics; 2003. pp. 14–7. [Google Scholar]
- 11.Tiwari B K. Annexure III. In: Tiwari B K, editor. Revised Policy Guidelines on National Iodine Deficiency Disorders Control Programme, Revised Edition. New Delhi: National Rural Health Mission IDD and Nutrition Cell Directorate General of Health Services Ministry of Health and Family Welfare Government of India; 2006. pp. 13–7. [Google Scholar]
- 12.Purty AJ. Methods. In: Singh Z, editor. Prevalence of Goiter and Urinary Iodine status of school children in Puducherry (India)-progress towards elimination of Iodine Deficiency Disorders (IDD) Puducherry: Department of community medicine PIMS; 2009. p. 22. [Google Scholar]
- 13.Jelliffe BD. The Assessment of the Nutritional Status of the Community. Geneva: World Health Organization; 1966. pp. 63–78. [Google Scholar]
- 14.Centers for Disease Control and Prevention. Division of Nutrition, Physical Activity and Obesity, National Center for Chronic Disease Prevention and Health Promotion. [Last cited 2009 Dec 27]. Available from: http://www.cdc.gov/obesity/childhood/defining.html .
- 15.Centers for Disease Control and Prevention. Division of Nutrition, Physical Activity and Obesity, National Center for Chronic Disease Prevention and Health Promotion. [Last Cited 2009 June 02]. Available from: http://www.cdc.gov/healthyweight/assessing/bmi/childrens_bmi/tool for schools.html .
- 16.Hutchon David J R. BSc, MB, ChB, FRCOG Consultant Gynaecologist, Memorial Hospital, Darlington, England. [Last cited 2009 May 29]. Available from: www.hutchon.net/confidOR.htm.
- 17.Herbert Rob. [Last cited 2009 Dec 27]. Available from: http://www.pedro.org.au/wpcontent/uploads/CIcalculator.xls .
- 18.Bhave S, Bavdekar A, Otiv M. IAP National Task Force for Childhood, Prevention of Adult Diseases: Childhood Obesity. Indian Pediatr. 2004;41:559–75. [PubMed] [Google Scholar]
- 19.Raj M, Sundaram KR, Paul M, Deepa AS, Kumar RK. Obesity in Indian children: Time trends and relationship with hypertension. Natl Med J India. 2007;20:288–93. [PubMed] [Google Scholar]
- 20.Laxmaiah A, Nagalla B, Vijayaraghavan K, Nair M. Factors Affecting Prevalence of Overweight Among 12- to 17-year-old Urban Adolescents in Hyderabad, India. Obesity. 2007;15:1384–90. doi: 10.1038/oby.2007.165. [DOI] [PubMed] [Google Scholar]
- 21.Subramanyam V, Jayashree R, Rafi M. Prevalence of overweight and obesity in affluent adolescent girls in Chennai in 1981 and 1998. Indian Pediatr. 2003;40:332–6. [PubMed] [Google Scholar]
- 22.Chhatwal J, Verma M, Riar SK. Obesity among pre-adolescent and adolescents of a developing country (India) Asia Pac J Clin Nutr. 2004;13:231–5. [PubMed] [Google Scholar]
- 23.Khadilkar VV, Khadilkar AV. Prevalence of Obesity in Affluent School Boys in Pune. Indian Pediatr. 2004;41:857–8. [PubMed] [Google Scholar]
- 24.Panjikkaran ST, Kumari K. Augmenting BMI and Waist-Height Ratio for establishing more efficient obesity percentiles among school children. Indian J Community Med. 2009;34:135–9. doi: 10.4103/0970-0218.51233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Rajul K Gupta. Nutrition and the Diseases of Lifestyle. In: RajVir Bhalwar., editor. Text Book of Public health and Community Medicine. 1st ed. Pune: Department of community medicine, AFMC, New Delhi: Pune in Collaboration with WHO India Office; 2009. p. 1199. [Google Scholar]