

A 27-year-old man with Behets disease was admitted to hospital after two episodes of typical rest chest pain and numbness of the left arm in the past 24 hours. Past medical history showed no risk factors for coronary artery disease. Behets disease had been diagnosed 7 years ago, and he was currently treated with colchicine.
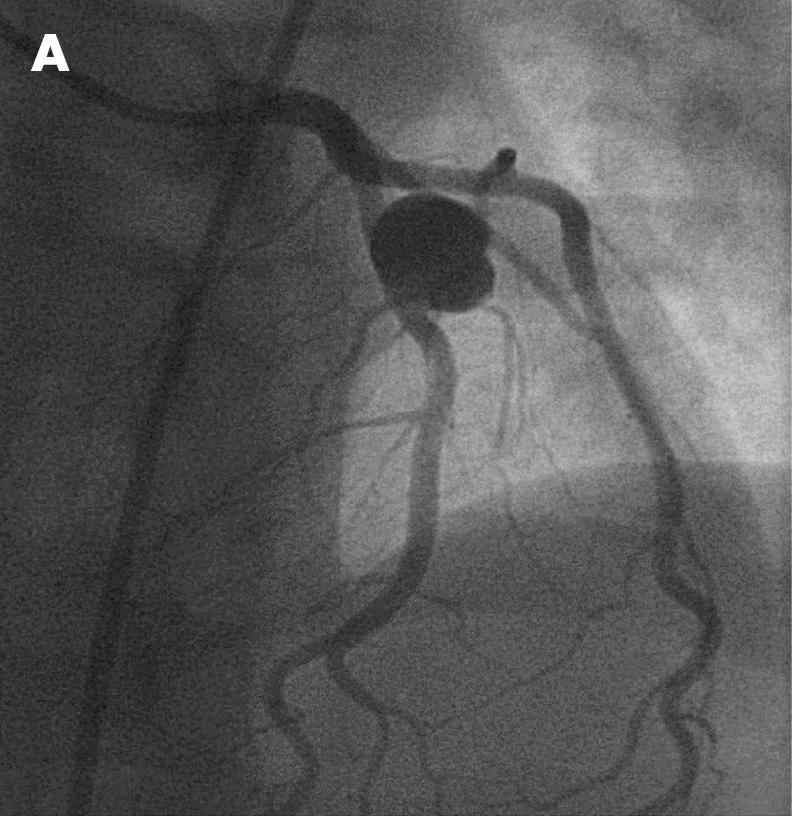
On first examination in the emergency room, blood pressure was 120/70 mm Hg and heart rate 75 bpm. Echocardiography showed sinus rhythm with normal repolarisation. Laboratory tests showed raised troponin at 1.6 IU/nl (normal <0.4). Based on these data, non-ST elevation myocardial infarction was diagnosed. An early coronary angiogram was performed, showing an isolated giant aneurysm of the mid left anterior descending artery (panel A). A left ventriculogram showed a normal ejection fraction. Intravascular ultrasound analysis of the mid left anterior descending artery demonstrated at the site of aneurysm neither thrombus nor atherosclerotic lesion, but a mild thickening of the intima and media layers, suggesting an inflammatory process.This abnormal intravascular ultrasound finding was also seen close to the aneurysm despite a normal angiographic aspect (panel B). No other vascular localisations were detected, particularly in pulmonary arteries.
We did not attempt coronary intervention and decided on conservative treatment with oral antithrombotic treatment. Ten days after this acute coronary syndrome, since the patient was symptom-free, he was discharged under aspirin 160 mg and clopidogrel 75 mg once a day. The patient has not had any further episodes of chest pain and complications during a 6-month follow-up period.

Acknowledgments
This article has been adapted from Cuisset T, Quilici J, Bonnet J-L. Giant coronary artery aneurysm in Behets disease Heart 2007;93:1375