

Abstract
Background:
The literature does not offer the rate of protection provided by different types of helmets used, especially as it applies to developing countries. We hypothesize that standard versus nonstandard types of helmets might differ in the rate of complications of head and neck trauma occurring in victims of motorcycle accidents. Here we report the rate of occurrence, the type of injuries and differences thereof in standard and nonstandard helmet bearers, and its relevance to protection from serious injury.
Methods:
The data were gathered from a data set of motorcycle accident victims admitted to the emergency department of Sina Hospital (Teheran/Iran). A cross-sectional study was designed for a 6-month period of time, June to December 2007. Variants analyzed included: demographics, types of helmets used, level of education of the victims (as in: being trained for using helmets and status of holding a valid driving license). The latter variants were evaluated for possibly influencing the outcome of the injured motorcyclists using either kind of helmets.
Results:
Among a total of 576 injured motorcyclists who had head, face, or neck injuries, 432 (75%) were using some kind of helmet. A total of 144 (25%) of the injured patients were admitted to the neurosurgical emergency service. There were 100 patients whose data sheets contained all variables which could be included in the pilot analysis of this cohort.
Discussion:
All 100 subjects were male patients with the age range of 32 ± 11 years. Twenty-five percent were using standard helmets at the time of accident, 43% had no cranio-facio-cervical injury except very mild skin abrasions, and 23% had facial injury, including skin lacerations needing sutures, two nasal bone fractures, and no maxillofacial damage. Among the patients using standard helmets, 44% had head injuries which needed to be taken care of (mostly nonoperatively), while 61% using nonstandard helmets had head trauma (P > 0.05). The other variables did not reach a significant value affecting the use of either standard or nonstandard helmets in prevention of craniofacial damages.
Conclusion:
This pilot analysis (comprising the data from 100 cases of motorcycle accidents) could not demonstrate statistically significant differences in injury patterns of different types of helmets and variants influencing their respective use. However, it can lead the way for further analysis of larger and more comprehensive head trauma databases regarding factors contributing to the issue of head injury.
Keywords: Cranio-cervico-facial trauma, cross-sectional analysis, head trauma, helmet, motorcycle accident
INTRODUCTION
Motorcycle is a convenient transportation vehicle especially in developing countries and popular for several reasons, i.e. being cheaper to acquire, of low running expenses (considering fuel consumption) and moving more rapidly in the local traffic jam. Due to a lack of protection provided by a passenger enclosure (such as the driver compartment in cars), accidents frequently result in death or disability leaving a heavy burden upon the national health organizations. It is quite evident for every citizen in larger or smaller villages of Iran that motorcyclists are the least protected and most danger producing vehicle drivers on the roads. It has been established that wearing helmet can effectively protect and reduce the rate and severity of head injury.[1,3,4,6–8,10,12,13,15,18–20] It is suggested by some authors that helmets with full coverage [Figure 1a] were found to be safer than half-shell helmets.[4] An extensive search in the literature via Pubmed, Embase, and other available search machines, using different key words (i.e., cranio-cervico-facial trauma, head trauma, helmet, and motorcycle accident) showed scarce evidence regarding the efficacy of various kinds of helmets used by different populations with varying socioeconomic situations.[5,9,16,17] With this study, we do not intend to prove the protective effect of helmets in motorcycle accidents per se, but hypothesize that standard versus nonstandard types of helmets might differ in the rate of head and neck trauma in victims of motorcycle accidents. We therefore intended to compare the protective efficacy of different kinds of helmets available in the Iranian market. Beyond this, we were interested in investigating selected variants possibly influencing the use of such helmets and its relevance to such motorcycle accidents.
Figure 1.

(a) Standard helmet. (b-d) Nonstandard helmets
MATERIALS AND METHODS
This is a cross-sectional study that includes the cases of motorcycle accident victims admitted to the emergency department at Sina Hospital, Tehran University of Medical Sciences (TUMS) during a 6-month period from June up to December 2007. All data were collected prospectively and were based on a questionnaire. This data-sheet contained all demographic variants and a photo of the encountered helmets as brought in by the referral (these were later classified as standard versus nonstandard helmets [Figure 1]). Further information was obtained regarding the MVA-victims, and we assessed the following variables: the individual's level of education, whether victims had been trained for using helmets and whether they had been holding a valid driving license.
The emergency department at Sina Hospital is a level one trauma service working 24 h/7 days/week. Injured motorcyclists were assessed by a resident of the neurosurgery service and a resident of the emergency service upon arrival to the emergency department and they collected all the data contained in the questionnaire.
All involved residents had been trained prior to commencement of the study in a group discussion to become familiar with the objectives of the research. The questionnaire entries were reviewed by the neurosurgeon conducting the research study the day after admission of the cases to the emergency department.
Statistical analysis
All data were analyzed by SPSS software version 11. An analysis was performed to test for a possible correlation of different factors (e.g., the type of helmets used by the motorcyclists) and its impact upon the severity of sustained cranio-cervico-facial injuries. Any P values <0.05 were regarded as significant.
RESULTS
Of 576 motorcyclists injured in street accidents, who were admitted to the emergency department of Sina Hospital, 432 had used helmets (75%) (CI = 95%, 71–78%). Amongst those 576 cases, there were 144 victims suffering from isolated cranio-cervico-facial injuries who were admitted directly to the neurosurgical department (25%). The others were mostly suffering from visceral, long bone, or other organ damages without serious neurosurgical problems. Those patients were admitted to the trauma service. The data sheet was fully and acceptably completed in 100 cases (out of the 144 admitted to neurosurgery) which were included for analysis. Standard management and work up were done for every case including general physical examination, skull and cervical X-rays, brain CT-scan, and CT-scan of the cervical vertebrae if the X-rays were suspicious for cervical fracture but nonconclusive.
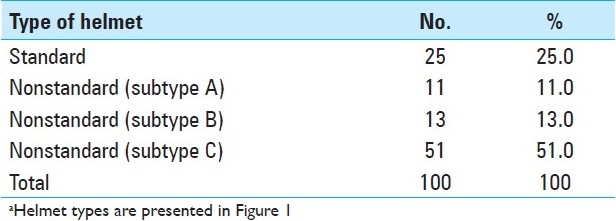
The type of helmets encountered were standard type A = 25%, nonstandard type B = 11%, type C = 13%, and type D = 51%. Interestingly enough, only 25% of the motor vehicle drivers had been given instructions about the helmets beforehand [Table 1].
Table 1.
Types of helmets used by motor cyclistsa
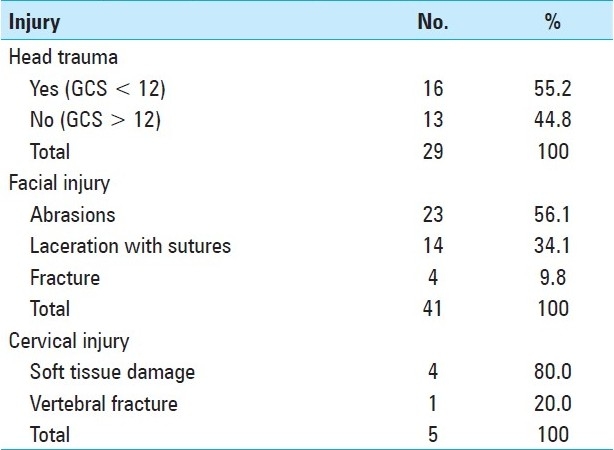
There were 29 victims with head trauma, of which 16 (55.2%) presented with a GCS < 12 and 13 with GCS > 12 [Table 2]. Among the cases with face injuries, 23 had only skin abrasions, 14 needed skin suturing, and 4 suffered from fractures in the bony structures of the face. Five patients were suffering from cervical injury, among whome four had soft tissue damages and one had cervical vertebral fracture which could be managed conservatively [Table 2].
Table 2.
Types of injuries among motorcycle drivers
All victims were male (which is explained by social determinants, since according to the laws and prohibitions females do not usually drive motorcycles in public in Iran). The average age of the victims was 32.3 ± 11.9 years (range 16–71 years). The level of education among them was assessed and divided into: school graduates 68%, high school graduates 37%, and 5% attendees of any type of university training programs. Ninety-one of the victims (91%) were motorcycle drivers and 9% were passengers sitting behind the rider. Only 64% of the victims had a valid driving license, the others were driving without having such a license. The average driving speed was estimated at 47 km/h ± 17, based upon the report of the attending police officers [Table 3].
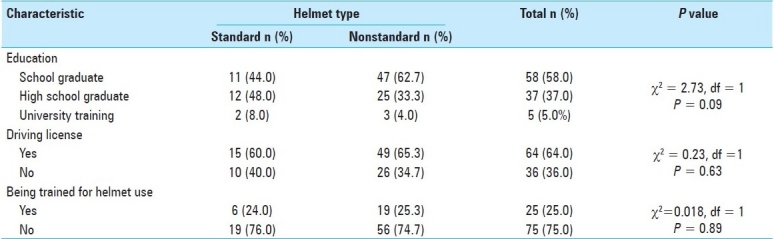
Table 3.
Background characteristics of motorcycle drivers referred to Sina Hospital, as subdivided by the helmet type (25 standard helmets and 75 nonstandard helmets, total sample size = 100)
There was one death in a patient with severe head trauma, the remaining 99 victims of the study cohort survived. The average duration of hospitalization was 2.3 days ± 2.2, with the shortest being 1 day and the longest 15 days.
Table 3 demonstrates that there was no significant relationship between the level of education or training and the type of helmet used by the motorcyclist injured in the accident (P > 0.05). There was also no significant relationship between the status of the victim as the motorcycle driver or the passenger and the type of helmet used (P = 0.33), although the number for the latter group was too small to draw a reliable conclusion.
Even though 64% of the injured patients held driving license, there was no significant relation to the type of helmet used by motorcyclists (P > 0.05) [Table 3]. Only 25% of the cyclists had received any instruction or training about using helmets before the incident and no significant relationship could be found to the type of helmet used [Table 3].
The relationship between the type of helmet used and the occurrence of crani-cervico-facial injuries was also nonsignificant [P > 0.05, Table 3], although this may be related to the relatively a minor injury pattern indicated by a comparably GCS admission score (e.g.: in developed countries, injuries may occur more frequently between motorcycles and cars, motorcycles and construction sites, etc.). The length of hospital stay was also not related to the type of helmet used by the cyclists (P > 0.05) [Table 3].
DISCUSSION
Motorcycle-related trauma is becoming increasingly a public health problem in the Iranian society.[17] While motorcycles account for only about 2% of all registered vehicles in the United States, nearly 9% of total US traffic fatalities were attributed to motorcycle riding. Although comparable data are not available for Iran, the absolute number of traffic victims will be significantly higher, based on the impression that motorcycles are being more frequently used.
In 2002, the fatality rate per 100,000 registered motorcycles in the USA was 65.35, an 18% increase from the 55.30 rate reported in 1997.[7,14] The increment in fatalities has been attributed to different factors such as the changes in the size and types of the vehicles, changes in toxicology screen results (reflecting drug abuse and alcohol intake) as well as changes in the age of the drivers and their habits.[1421] Prior reports have demonstrated that, after controlling for other environmental factors, “universal helmet laws” are associated with lower motorcyclist fatality rates.[3–5,20] Interestingly enough, this database shows that even in a developing country among 576 traumatized motorcyclists, 432 had been using helmets (75%). We have been trying to look for the influence of different types of helmets used by the motorcyclists in the Iranian population and its effect on injury patterns. Certainly, it is not a population based study, but we have started a comprehensive registry at our hospital from which we are reporting the result of a preliminary analysis of 100 cases. Looking extensively into different kinds of helmets available in the Iranian market, they could arbitrarily be classified into standard [Figure 1a] and nonstandard helmets [Figure 1b–d].
Comparing the results of this study with other reports on MVA in developing countries shows that the average age of the injured motorcyclists matches the affected age group mentioned in other reports and nearly all the injured victims were also male.[1,6,19,14] To this end, this injury pattern occurs in the most productive age group of society and subsequent disability has an enormous economic impact, and generates a significant cost-burden for continued long-term care in an emerging health care system.
Two other aspects are worth mentioning: the size of the motor cycle and consumption of alcoholic beverages is tightly controlled under Islamic regulations. Therefore, these factors have not been among the variants evaluated in our data set of motorcycle riders in Tehran and can hence not be compared with other reports. However, relevant issues such as holding a driving license, level of education, and previous training about the use of helmets were variants evaluated by us. We feel this to be an important aspect, since the implementation of measures influencing the prevention of injury seems differ in developing countries. These aspects are only anecdotally assessed by other authors from the developed world, for example Denmark[2,11] We consider this aspect worthwhile to be included in future research data registries such as ours.
As seen from Tables 3and 4, all of the mentioned variants showed a trend reflecting notable effects upon the use of certain helmet types though their values did not reach significance (P > 0.05).
Table 4.
Cranio-cervico-facila injuries among motorcycle drivers referred to Sina Hospital as subdivided by the type of helmet

However, as can be seen from our results, wearing a standard helmet could reduce the risk of cranio-cervico-facial injuries more prominently than the nonstandard types B, C, and D. Standard type A helmet could prevent head trauma in almost 56% of the patients, but even nonstandard helmets were still effective to this end in 39% of the injured motorcyclists. These rates are similar to those reported before, emphasizing the safety achieved by the use of helmets[1,10,13,18–20] although they were not statistically different when comparing the two types of helmets [OR = 0.49, Table 4].
Even though the period of hospital stay was generally not affected by the type of helmets used, it might be more significantly influenced by the mechanism of injury, speed of the driver, size of the vehicle, and other safety guards of the motorcycle.
Limitations
There are several limitations of this study. Firstly, the number of included cases is rather low representing a total of only 100 cohort patients of a total of 576 patients admitted with this injury mechanism to our hospital. However, as we have pointed out in the “Introduction” section, we intended to report the preliminary results of an ongoing study only, which is a larger prospective project currently being undertaken at our level one trauma center. A second aspect is that all individuals included in this study cohort were assessed by census only, and all have been referred to a single treatment center. Data collection may thus have included some bias based on local referral patterns. Thirdly, we are not aware of the number of trauma victims, who died at the scene of the accident, and we do not know whether they did wear any helmets (and if so of which type). We consider this a rare event and do not believe that it has disturbed the results of our study. However, this aspect could be included in further studies.
CONCLUSION AND SUGGESTIONS
Although not all results reached statistical significance in the issues highlighted in this study, some suggestions can be made:
Motorcyclists should be instructed to properly and consistently wear a helmet for their safety.
Motorcycle drivers should be obliged to hold standard driving licenses and follow rules for safe driving.
It seems necessary to advocate not to put nonstandard helmets on the market, since there risk reduction for head and neck injury is inferior to standard types. This could be achieved not only by prohibiting their production, but also by selling cheaper standard helmets in the markets.
We suggest that the motorcycle producing companies sell standard helmets as a package along with their motorcycles and instruct the buyers to use them appropriately. This way a proper education of users can be ensured.
It is necessary to undertake similar prospective projects in a number of different trauma centers in societies in which motorcycle riding is a major way of transportation, such as in Middle and Far-East countries. This would allow to collect a pool of data for better documentation and ultimately allow to organize a multicenter trial (possibly involving manufacturers) investigating effective measures to reduce head and neck injury risk in motor cycle accidents.
Footnotes
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2011/2/1/49/79771
Contributor Information
Abbas Amirjamshidi, Email: abamirjamshidi@yahoo.com.
Ali Ardalan, Email: aardalan@gmail.com.
Kourosh Holakouie Nainei, Email: holakouie@yahoo.co.uk.
Sadegh Sadeghi, Email: sadeghisadegh@yahoo.com.
Mehrdad Pahlevani, Email: mehrtat@yahoo.co.uk.
Mohammad Reza Zarei, Email: mrzarei@sina.tums.ac.ir.
REFERENCES
- 1.Bachulis LB, Sangster W, Gorrell GW. Patterns of injury in helmeted and non-helmeted motorcyclists. Am J Surg. 1988;155:708–11. doi: 10.1016/s0002-9610(88)80151-x. [DOI] [PubMed] [Google Scholar]
- 2.Bjornstig UL, Bylund PO, Lekander T, Brorsson B. Motorcycle fatalities in Sweden. Acta Chir Scand. 1985;151:577–81. [PubMed] [Google Scholar]
- 3.Bradbury A, Robertson C. Pattern and severity of injury sustained by motorcyclists in road traffic accidents in Edinburgh, Scotland. Health Bull (Edinb) 1993;5:86–91. [PubMed] [Google Scholar]
- 4.Chiu WT, Kuo CY, Hung CC, Chen M. The effect of the Taiwan motorcycle helmet use law on head injuries. Am J Public Health. 2000;90:763–6. doi: 10.2105/ajph.90.5.793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Coben JH, Steiner CA, Miller TR. Characteristics of motorcycle-related hospitalizations: Comparing states with different helmet laws. Accid Anal Prev. 2007;39:190–6. doi: 10.1016/j.aap.2006.06.018. [DOI] [PubMed] [Google Scholar]
- 6.Gopalakrishna G, Peek-Asa C, Kraus JF. Epidemiologic features of facial injuries amongst motorcyclists. Ann Emerg Med. 1998;32:425–30. doi: 10.1016/s0196-0644(98)70170-2. [DOI] [PubMed] [Google Scholar]
- 7.Houston DJ, Richardson LE. Motorcyclist fatality rates and mandatory helmet-use laws. Accid Anal Prev. 2008;40:200–8. doi: 10.1016/j.aap.2007.05.005. [DOI] [PubMed] [Google Scholar]
- 8.Ichikawa M, Chadbunchachai W, Marui E. Accident Analysis and Prevention, Effect of the helmet act for motorcyclists in Thailand. Accid Anal Prev. 2003;35:183–9. doi: 10.1016/s0001-4575(01)00102-6. [DOI] [PubMed] [Google Scholar]
- 9.Keng SH. Helmet use and motorcycle fatalities in Taiwan. Accid Anal Prev. 2005;37:349–55. doi: 10.1016/j.aap.2004.09.006. [DOI] [PubMed] [Google Scholar]
- 10.Kraus JF, Peek C, McArthur DL, Williams A. The effect of the 1992 California motorcycle helmet use law on motorcycle crash fatalities and injuries. J Am Med Assoc. 1994;272:1506–11. [PubMed] [Google Scholar]
- 11.Larsen CF, Hardt-Madsen M. Fatal motorcycle accidents in the county of Funen (Denmark) Forensic Sci Int. 1988;38:93–9. doi: 10.1016/0379-0738(88)90013-8. [DOI] [PubMed] [Google Scholar]
- 12.Liu B, Ivers R, Norton R, Blows S, Lo SK. Helmets for preventing injury in motorcycle riders. Cochrane Database Syst Rev. 2004;2:CD004333. doi: 10.1002/14651858.CD004333.pub2. [DOI] [PubMed] [Google Scholar]
- 13.Mock CN, Maier RV, Boyle E, Pilcher S, Rivara FP. Injury prevention strategies to promote helmet use decrease severe head injuries at a level I trauma center. J Trauma. 1995;39:29–33. doi: 10.1097/00005373-199507000-00004. [DOI] [PubMed] [Google Scholar]
- 14.Norvell DC, Cummings P. Association of helmet use with dealt in motorcycle crashes: A matched-pair cohort study. Am J Epidemiol. 2002;156:483–7. doi: 10.1093/aje/kwf081. [DOI] [PubMed] [Google Scholar]
- 15.Peek-Asa C, McArther DL, Kraus JF. The prevalence of non-standard helmet use and head injuries among motorcycle riders. Accid Anal Prev. 1999;31:229–33. doi: 10.1016/s0001-4575(98)00071-2. [DOI] [PubMed] [Google Scholar]
- 16.Rasouli MR, Nouri M, Zarei MR, Saadat S, Rahimi-Movaghar V. Comparison of road traffic fatalities and injuries in Iran with other countries. Chin J Traumatol. 2008;11:131–4. doi: 10.1016/s1008-1275(08)60028-0. [DOI] [PubMed] [Google Scholar]
- 17.Sarkar S, Peek C, Kraus JF. Fatal injuries in motorcycle riders according to helmet use. J Trauma. 1995;38:242–5. doi: 10.1097/00005373-199502000-00017. [DOI] [PubMed] [Google Scholar]
- 18.Shankar BS, Ramzy AI, Soderstorm CA, Dischinger PC, Clark CC. Helmet use, patterns of injury, medical outcome, and costs among motorcycle drivers in Maryland. Accid Anal Prev. 1992;24:385–96. doi: 10.1016/0001-4575(92)90051-j. [DOI] [PubMed] [Google Scholar]
- 19.Sosin DM, Sacks JJ, Holmgreen P. Head injury-associated death from motorcycle crashes: Relationship to helmet-use laws. J Am Med Assoc. 1990;264:2395–9. [PubMed] [Google Scholar]
- 20.Swaddiwudhipong W, Boonmak C, Nguntra P, Mahasakpan P. Effect of motorcycle rider education on changes in risk behaviours and motorcycle-related injuries in rural Thailand. Trop Med Int Health. 1998;3:767–70. doi: 10.1046/j.1365-3156.1998.00301.x. [DOI] [PubMed] [Google Scholar]