

Abstract
Background:
The scars of the cutaneous leishmaniasis and psychological problems of this disease need different interventions for its correction.
Aim:
Our objective in this study was to compare the efficacy of 50% trichloroacetic acid (TCA) solution and CO2 laser for treatment of the atrophic scars due to leishmaniasis.
Materials and Methods:
This was a randomized clinical trial performed in 92 patients. Patients were randomized into two groups: the first group was treated with 50% TCA solution, once monthly and for a maximum of 5 months, and the second group was treated with CO2 laser which was performed for only one time. Patients were followed-up at 3 and 6 months after starting the treatment. The improvement of scar was graded by a 6-point scale using digital camera and the collected data were analyzed using SPSS software.
Results:
In this study, 74 females and 18 males were enrolled. The improvement of scar was 48.13% in the TCA group and 44.87% in the CO2 laser group. This difference was not statically significant (P = 0.55). There was also no significant difference regarding side effects between these two groups.
Conclusion:
The results of our study showed that efficacy of focal with 50% TCA solution is compared with CO2 laser in treatment of leishmaniasis scar. Because of the low cost and simple application of TCA solution in comparison with CO2 laser, we suggest use of this treatment for correction of leishmaniasis scar or the atrophic scars.
Keywords: Cutaneous leishmaniasis, trichloroacetic acid, CO2 laser, scar, treatment
Introduction
Cutaneous leishmaniasis is an endemic disease of Iran. Unfortunately, there is no definite treatment for this disease.[1] Despite self-healing nature of this disease, the scar that remains due to the disease can induce many psychosocial problems for patients. Cutaneous leishmaniasis scar is an atrophic scar that is formed due to dermal atrophy and destruction of collagen following acute inflammatory reaction.
It is shown that application of 65 and 100% trichloroacetic acid (TCA) can be used for the treatment of atrophic acne scars.[2]
One of the other methods that are used extensively for treatment of the atrophic scars, such as those formed due to acne or chicken pox, is high-energy pulsed or scanned CO2 laser that can abrade epidermis in one pass.[3]
In one study that was performed in 30 patients with acne scar, chicken pox scar and atrophic scar due to heart surgery, 60% improvement in scar appearance was observed following short-pulse and continuous CO2 laser.[4]
Although CO2 laser can effectively repair the atrophic scars, some side effects the treatment causes, such as prolonged healing time, resistant erythema and hypopigmentation in 20% of treated cases, should also be considered.[3,5]
We designed the following study to evaluate the effect of focal peeling with TCA versus CO2 laser in treatment of leishmaniasis scar.
Materials and Methods
This study was a randomized controlled clinical trial that was performed in 92 patients, aged 18–50 years, with atrophic leishmaniasis scar. Only patients who had scar on their faces or hands were selected. Patients were randomized into two groups, each including 46 patients.
Patients with chronic diseases, immunodeficiency, history of hypertrophic scar or keloids, history of isotretinoin use is the last 1 year, pregnancy or lactation were included.
Informed consent was obtained from all patients. For 50% TCA application, the scar site was first defatted with acetone and then 50% TCA was applied to the scar site using cotton applicator. After whitening of the scar, the acid was neutralized using water and petrolatum was then applied. Patients were then instructed to apply sunscreen at the morning and noon and hydroquinone 4% cream at the nights.
This treatment was performed in monthly intervals and for a maximum of five times. Patients were followed every 2 weeks for 3 months and then at 6 months after starting the treatment.
For CO2 laser treatment, continuous wave CO2 laser, 10,600 nm, 3-mm spot size, fluence 5 J/cm2, 1–3 passes, based on depth of the scar was performed. CO2 laser treatment was performed only one time and the patients were followed at the start, 3 and 6 months after starting the treatment. In both the groups, any relevant side effect was recorded.
Digital photography was performed using SONY 5 megapixel, DSC-F707 with the same light and angle.
Improvement in the depth of scar was graded by using a 6-point score as follows: (1 = non healing, 2 = 7–19% improvement, 3 = 20–39% improvement, 4 = 40–59% improvement, 5 = 60–79% improvement, 6 = 80–100% improvement).
Data analysis was performed using SPSS 13 software and statistical tests including t test, Wilcoxon and Mann-Whitney test. P value less than 0.05 was set as significant.
Results
Overall, 92 patients, aged 18–41 years, were evaluated. Selected patients had skin type of II-IV.
Forty-six patients were treated with 50% TCA solution (39 females, 7 males) and 46 patients were treated with CO2 laser (35 males, 11 females).
Improvement of leishmaniasis scar at 6 months follow up was found to be 48.13 and 44.87% for 50% TCA and CO2 laser, respectively (P = 0.55). Prevalence distribution of scar improvement based on a 6-point scale is shown in Figure 1.
Figure 1.
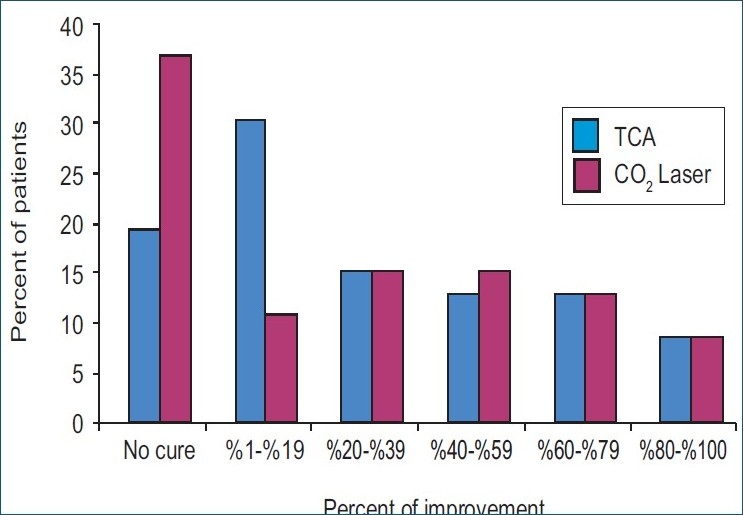
Prevalence distribution of scar improvement in the two groups treated with CO2 laser and 50% TCA solution at 6-month follow up
The reduction of scar depth before and after treatment was 1.63±0.74 (P = 0.04) and 1.34±1.3 (P = 0.04); both were significant as compared with the ones before treatment. However, there was no significant difference between the two methods of treatment regarding reduction of scar depth (P = 0.813).
In the group treated with 50% TCA solution, in 76.1% (35 patients) of cases, no side effect was observed and in 23.9% (11 patients) of cases, hyperpigmentation was observed in the scar site [Table 1].
Table 1.
Prevalence distribution of age, sex and skin type in patients showing hyperpigmentation in the two treatment groups

In the group treated with CO2 laser, 76.1% (35 patients) had no side effects and in 17.4% (8 patients) hyperpigmentation and in 6.5% (3 patients) resistant erythema was observed.
Discussion
Cutaneous leishmaniasis is an important health problem. One of the most important foci of cutaneous leishmaniasis is Isfahan province, Iran.[1] In some villages of Isfahan, Iran, more than 70% of people are affected by cutaneous leishmaniasis scar.[6]
Leishmaniasis scars are usually depressed and atrophic. Patients affected by these scars usually have psychosocial and cosmetic complains.[7]
Therapeutic modalities for repairing these scars include peeling, laser, dermabrasion, punch excision, resurfacing and use of soft tissue fillers.[8]
Application of TCA with more than 40% concentration can induce medium depth peeling, and therefore, precipitation of epidermal proteins, coagulative necrosis of epidermal cells and collagen of papillary and upper reticular dermis. Also, studies have shown that some clinical effects of TCA are due to restoration of dermal structures and increase of collagen, glycosaminoglycans and elastin in the dermis.[9]
In another study, application of 50% TCA solution in patients with acne scar showed that a patient's satisfaction ranged from 33.3% after the first treatment session to 80% after the third session.
The risk of post inflammatory hyperpigmentation is one of the limiting factors for use of TCA solution in treatment of scars. However, the results of the study that was performed by Al-Waiz et al. showed that postinflammatory pigmentation was cleared in 73.4 after 3 months of treatment.[5]
Focal TCA peeling usually has a few side effects and the area usually heals very fast. In addition, the results of TCA focal peeling are long lasting.[11]
CO2 laser abrades epidermis and upper dermis without any damage to sebaceous glands, hair follicles and sweat duct, and therefore, causes remodeling of skin and neocollagenesis.[13,14]
Our findings showed promising results regarding application of 50% TCA solution for treatment of leishmaniasis scars. TCA solution is readily available and its application is fast and simple. The patients usually have very few side effects [Figure 2].
Figure 2.

The results of treatment of leishmaniasis scars with 50% TCA solution after 5 monthly applications. Photograph B shows the results of treatment, 1 month after the fifth session of the treatment
We suggest the use of focal TCA peeling for treatment of cutaneous leishmaniasis scars.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil.
References
- 1.NilfroushZadeh MA, Sadeghian G, Cutaneous Leishmaniasis. Isfahan University of Medical Sciences. 2002:45–47. [Google Scholar]
- 2.Lee JB, Chung WG, Kwahck H. Focal treatment of acne scars with trichloroacetic Acid. Surg Dermatol. 2002;11:1017–21. doi: 10.1046/j.1524-4725.2002.02095.x. [DOI] [PubMed] [Google Scholar]
- 3.Lupton JR, Alster TS. Laser scar revision. Clin Dermatol. 2002;20:55–65. doi: 10.1016/s0733-8635(03)00045-7. [DOI] [PubMed] [Google Scholar]
- 4.Bernstein LJ, Kauvar AN, Grossman MC, Geronemus RG. Scar resurfacing with high-energy, short – pulsed and flash scanning carbon dioxide lasers. Surg Dermatol. 1998;24:101–7. doi: 10.1111/j.1524-4725.1998.tb04060.x. [DOI] [PubMed] [Google Scholar]
- 5.Al-waiz MM, Al-Shargi AI. Medium – depth chemical peels in the treatment of acne scars in dark – skinned in individuals. Surg Dermatol. 2002;28:383–7. doi: 10.1046/j.1524-4725.2002.01081.x. [DOI] [PubMed] [Google Scholar]
- 6.Ardhali S, Rezaei K, Nadim A. Leishmaniasis parasite and Leishmaniasis. Tehran, Markaze Nashre Daneshgahi; 1986:149–60. [Google Scholar]
- 7.Bayat A, Ferguson MWJ. Skin scarring. BMJ. 2003;326:88–92. doi: 10.1136/bmj.326.7380.88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hirsch RJ, Lewis AB. Treatment of acne scarring. Semin Cutan Med Surg. 2001;20:190–8. doi: 10.1053/sder.2001.27557. [DOI] [PubMed] [Google Scholar]
- 9.Brodland DG, Cullimore KC, Roenigk RK, Gibson LE. Depth of chemexfoliation induced by Various concentrations and application techniques of trichloroacetic acid in a porcine model. J Dermatol Surg Oncol. 1989;15:967–71. doi: 10.1111/j.1524-4725.1989.tb03183.x. [DOI] [PubMed] [Google Scholar]
- 10.Dinner M, Artz J. The art of the TCA chemical peel. Clin Plast Surg. 1998;1:53–62. [PubMed] [Google Scholar]
- 11.Cho SB, Park CO, Chung WG, Lee KH, Lee JB. Histometric and histochemical analysis of the effect of trichloroacetic acid concentration in the chemical reconstruction of skin scars method Chung Dermatol Surg. 2006;32:1231–6. doi: 10.1111/j.1524-4725.2006.32281.x. [DOI] [PubMed] [Google Scholar]
- 12.Brody HJ. Variations and comparisons in medium-depth chemical peeling. J Dermatol Surg Oncol. 1989;15:953–63. doi: 10.1111/j.1524-4725.1989.tb03182.x. [DOI] [PubMed] [Google Scholar]
- 13.Weinstein C, Roberts TL. Aesthetic skin resurfacing with the high-energy ultra pulsed CO2 laser. Clin plast surg. 1997;33:4303. [PubMed] [Google Scholar]
- 14.Weinstein C. Carbon dioxide laser resurfacing. Long-term follow up in 2123 patients. Clin Plast Surg. 1998;25:10930. [PubMed] [Google Scholar]