

Abstract
Objective
Our objective is to document the methodology of a randomized controlled clinical trial that demonstrates sound research methodology. The chiropractic treatment performed may be useful to allow practitioners to adopt a similar approach when treating hip osteoarthritis.
Methods
This study is a registered, ethics-approved, single-blinded, randomized controlled clinical trial. Recruitment included a controlled media release, phone screening, and physical assessment to rule out nonosteoarthritic hip pain. Primary outcome measures were the McMaster Overall Therapy Effectiveness Tool and the Western Ontario and McMaster Universities Osteoarthritis Index, which were assessed at baseline and after 1, 3, 6, and 9 months. Participants were randomly allocated to 1 of 2 intervention groups: protocol A or B. Protocol A received preadjustive stretches of hip musculature, followed by hip manipulation. Protocol B received the above intervention, followed by an additional assessment and chiropractic treatment of the lower limb kinetic chain. Participants received 9 treatments and then after 3 months were offered an additional 6 treatments. Statistics will be performed by an independent biostatistician.
Results
This article provides a valid and reliable protocol for a randomized controlled trial for the treatment of hip osteoarthritis with chiropractic care. Data should be analyzed for statistical significance to provide evidence for the efficacy of the interventions.
Conclusions
This study is an example of sound research methodology, which was scored as excellent on the Physiotherapy Evidence Database scale. Findings may be important in the scope of treatment, providing evidence for conservative management options for hip osteoarthritis.
Key indexing terms: Hip, Osteoarthritis, Chiropractic, Musculoskeletal manipulations, Kinematics
Introduction
Osteoarthritis (OA) is a musculoskeletal disorder that affects more than 12 million people in the United States1,2 and 3 million people in Australia.3 Ten percent of men and 20% of women aged between 45 and 65 years report OA,4 and this prevalence increases with age. It is believed that 80% of people older than 75 years show radiographic evidence of OA.5 In Australia, OA is the only musculoskeletal disorder among the leading causes of disease burden, which include a spectrum of physiological disorders such as ischemic heart disease, chronic obstructive pulmonary disease, stroke, depression, diabetes, and lung cancer.6 In the United States, OA is second only to ischemic heart disease as a cause of work disability in men older than 50 years and accounts for more hospitalizations than rheumatoid arthritis each year.5
Osteoarthritis typically presents as pain in one or more joints, loss of mobility, and decreased muscle function and strength.1 As it is associated with the aging population, this reduction in functional ability leads to an inability to perform activities of daily living such as managing personal hygiene (bathing, brushing hair and teeth), cooking meals, dressing, and attending social activities. Falls in the elderly are an inherent risk. Falls threaten the independence of older people; they are a significant cause of hospitalizations and morbidity and even lead to mortality. Studies report the incidence of falls in the elderly to be between 30% and 40% per year in people older than 65, and falls are responsible for two thirds of unintentional deaths in this age group.7-9 Falls are a result of a complex interplay of causes and risk factors: environmental hazards, muscle weakness, prescription medications, arthritis, use of an assistive device, and depression, as well as impairments in gait, balance, cognition, and vision.9 Musculoskeletal aging leads to poor mobility, weakness, and degenerative diseases.10 Specifically, a study on HOA shows that the affected hip has evident losses in muscle strength and muscle mass compared with the nonaffected hip.11 Chronic disuse of the lower limb in OA is a significant risk factor for falls in the elderly. It is not in the scope of this publication to outline the extensive literature on falls in the elderly; however, the Cochrane collaboration has published reviews on interventions preventing falls in the community12 and nursing homes and hospitals.13
Literature supports manipulative therapy for knee14-17 and HOA18-21; however, there are no studies that have investigated manipulative therapy of the full lower limb kinetic chain for hip OA (HOA) despite widespread use by manual therapists. It is believed that compensations of biomechanical dysfunction in the musculoskeletal system may result in change in function proximal or distal to the primary area of pathology.22 The concept of treating joint dysfunction within the full kinetic chain has been promoted within the chiropractic profession; and hence, this study shall investigate adding full lower limb kinetic chain manipulative therapy to a similar, previously published protocol of pre- and postmanipulation stretching.18
The objective of this article is to document the methodology of this study and provide information to allow practitioners to adopt a similar approach when treating HOA. Specific aims of the study include comparing 2 protocols of chiropractic management for the treatment of HOA and determining their efficacy via the McMaster Overall Therapy Effectiveness (OTE) Tool and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC).
Methods
Design
This study is an ethics-approved, registered, large-scale, single-blinded, randomized controlled clinical trial. The Institutional Review Board of Cleveland Chiropractic College gave approval for the trial to be conducted at Cleveland Chiropractic College Los Angeles (trial number CCCLA IRB approval 08102007). The Macquarie University Ethics Review Committee (Human Research) gave approval for the trial (ethics number HE22FEB2008-R05639). The trials were registered in the United States at ClinicalTrials.Gov (registration number NCT00523172) and in Australia through the Australian New Zealand Clinical Trials Registry (registration number ACTRN12609000664246). This study has used the Consolidated Standards of Reporting Trials checklist,23,24 items 1 to 12 (Fig 1).
Fig 1.
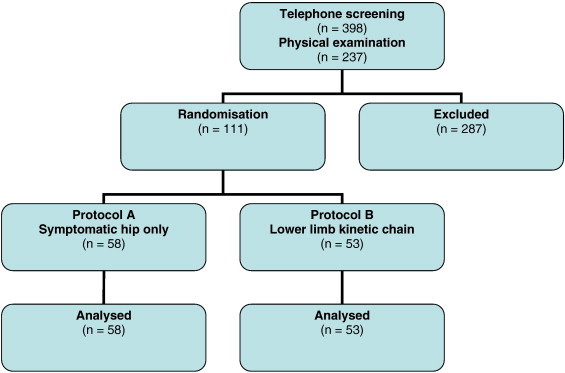
The Consolidated Standards of Reporting Trials flow diagram. (Color version of figure is available online.)
Settings
One university outpatient clinic located in Los Angeles, CA, USA, and 2 university outpatient clinics located in Sydney, Australia, were used for the duration of the trial.
Care providers
Senior interns, qualified in spinal and extremity manipulative technique, were used as care providers in this study. The care providers were selected via volunteering to participate in a randomized controlled trial and learning to perform a strict protocol of chiropractic care for participants diagnosed with HOA. Doctors of chiropractic employed as clinical supervisors at the institutional outpatient clinics clinically supervised the senior interns while performing treatment protocol.
Recruitment
Recruitment for the study commenced in January 2008, and the first participant was enrolled in May 2008. Recruitment was in the form of commercial newspaper and radio advertising, a controlled media release, free Web-based advertising, print media in the student outpatient clinics, and attendance to local community groups.
Participants
Interested individuals responded to an advertising campaign calling for people who suffered hip pain. They underwent initial phone screening to exclude systemic conditions or contraindications to manipulative therapy, that is, long-term corticosteroid use. They then presented for a physical assessment to rule out nonosteoarthritic hip pain. Subjects were included if they met the inclusion and possessed no exclusion criteria (Table 1). Inclusion criteria included meeting the American College of Rheumatology (ACR) clinical criteria for HOA25 and having recent radiographs graded by an independent chiropractic academic as having grade 1 to 3 HOA as per the Kellgren and Lawrence radiological assessment of OA.26,27 If recent radiographs were not available, participants had radiographs taken on-site at the student outpatient clinics that were graded and used to rule out bone pathology and for safety of the patient before manipulative therapy.15
Table 1.
Inclusion and exclusion criteria
| Inclusion | Exclusion |
|---|---|
| 1. ACR guidelines for HOA | 1. Significant visual, vestibular, neurological, peripheral, or sensory disorders |
| a. Hip pain AND ≤15° internal rotation AND ≤115° flexion | 2. History of hip joint replacement or bone pathology |
| OR | 3. History of lumbar herniated disc |
| b. Hip pain AND ≥15° internal rotation causing pain AND morning stiffness <60 min of duration | 4. Severe balance or proprioceptive problems |
| 2. Kellgren and Lawrence radiological assessment of OA | 5. Moderate to severe symptoms of HOA in both hips |
| a. Graded 1 to 3 HOA | 6. Marked or severe fear of manipulative therapy and/or exercise procedures |
Informed consent
Participants signed 2 consent forms to have personal health information published without divulging personal identifiers (one to keep and one that was returned to the university and the college). The informed consent form conveyed the following information: title of the trial; the purpose of the trial; the names of the chief investigators; the name of the university and department conducting the research; the dissemination of the results; the possibility of minor short-term muscular pain; in the event of adverse affect, the access to a professional practitioner; the right to withdraw at any time; the ethics approval; and contact details of the Ethics Committee.
Treatment allocation
Eligible participants were randomly allocated to 1 of 2 intervention groups: protocol A or protocol B. A random number generator was used to randomly sequence the 2 groups in allocations of 6 at a time. This reduced the potential of uneven groups if a smaller than expected response rate occurred. As each participant was successfully screened, he or she was allocated in 1 of 2 ways. In Australia, the protocol was recorded (per previous randomization as protocol A or B) on an electronic spreadsheet that only one research assistant, uninvolved with assessment or treatment, had access to. Upon the participant becoming eligible, the assistant then allocated the protocol. Hence, allocation was concealed at the time of recruiting. In the United States, the process was the same, using an uninvolved research assistant with the randomized numbers (representing protocol A or B) placed folded over in opaque envelopes and allocated as per a patient becoming eligible.
Participants were blinded as to which intervention they were allocated to, in an attempt to control for the Hawthorne effect.28,29 Senior interns who administered the treatment to the participant were not, and cannot, be blinded to the intervention.
Assessments
Outcome measures were assessed at the initial physical assessment; on the conclusion of 9 treatment sessions; and after 3, 6, and 9 months by assessors blind to patient allocation.
Outcome measures
Primary outcome measures included the McMaster OTE Tool and the WOMAC. Secondary outcome measures included hip range of motion measured with a goniometer, Harris Hip Score, and the Berg Balance Scale. The OTE is a valid and reliable 15-point questionnaire asking whether their HOA symptoms or overall quality of life has improved, remained the same, or worsened since the last visit using “improved (score +1 to +7),” “unchanged (score 0),” or “deteriorated (score −1 to −7).” Patients indicating improvement or worsening identify the extent of the change, answering additional questions on a final 7-point scale from 1 (almost the same) to 7 (a very great deal better/or worse).30,31 A +30% change with dichotomization of this primary outcome measure (percentage improved or not improved) will be considered a successful, statistically and clinically significant change.30-33 The WOMAC is self-administered and assesses the 3 dimensions of pain, disability, and joint stiffness in knee and hip OA using 24 questions.34 Each question is answered by the subject using a 100-mm visual analog scale, and measures are totaled for a maximum possible score of 2400. It has received much support for its measure of arthritic effects on a subject.34
Protocol
Both groups received an intervention of manual therapy. Protocol A received preadjustive stretches of the iliopsoas, rectus femoris, tensor fascia latae, sartorius, long adductors, and short adductors. Stretches were followed by high-velocity, low-amplitude long-axis traction hip pulls on the symptomatic hip. The hip pulls were modified with internal rotation and/or abduction where the range of motion felt restricted (subjectively by the intern). Postadjustive active-assisted stretches were delivered to hip musculature such as the hip flexors, hip adductors, hip abductors, tensor fasciae latae, piriformis and/or in the Patrick Fabre position.18,25 Protocol B received the above intervention, followed by an additional assessment of the lumbar spine and ipsilateral sacroiliac, knee, ankle, and foot joint complexes. Any restriction in range of motion was documented; and high-velocity, low-amplitude manipulation; joint mobilization; and/or post isometric stretching was performed on each individual joint complex to restore movement.
The participants in both protocols attended college and university outpatient clinics. They received 9 treatments (2 treatments per week for 1 month) of approximately 15 to 20 minutes' duration. They were reassessed at the end of 9 visits and then reassessed again at 3, 6, and 9 months. Participants were offered an additional 6 treatments after the 3-month assessment point, provided at an as-needed basis, which were able to be taken before the 9-month reassessment.
Adverse reactions
Participants' individual files include subjective, objective, adverse effects and progress notes for each treatment. This enables reporting of any adverse reactions, such as muscles soreness, stiffness, pain, and changes in gait. An important part in the reporting of any intervention is the occurrence and prevalence of adverse effects and should be integrated into the methodology for all clinical trials.
Analysis
Sample size
A sample size of 51 patients per group provides very good power for comparing percentage improvement in the primary outcome measure of the OTE. Per previous data, if this percentage in the manipulative (or manual) therapy plus rehabilitation is 80% and the percentage improvement is 50% in the rehabilitation alone group, then 51 patients per group gives a power just less than 90% (0.88). This assumes a 2-sided test at an α level of 5%. Power is also very good for comparing pain using the visual analog scale (a component of WOMAC) and can be converted to a percentage score of 100.35,36
Descriptive statistics are reported as mean (SD) for continuous outcomes and percentage for categorical outcomes. The percentage improvement as measured by OTE will be compared between the 2 groups using a χ2 test.35 For measurements between subjects (treatment group) and measurements within subjects (over time), a repeated-measures analysis of variance will be used.36 Continuous measures, such as the WOMAC, Harris Hip Scale, and goniometry will use t tests, confidence interval, and assessment as well as calculations of effect size.35,36 If a preliminary graph of a continuous variable shows a marked deviation from normality, a transformation will be examined to see if it will produce a distribution closer to normal. Intention-to-treat analysis will be used for all comparisons. Results will be reported using both P values and 95% confidence intervals. All tests will use a 2-sided α level of 0.05. Intention-to-treat analysis will be assumed to follow patients to analyze dropout, adverse effects, or commencement of alternative treatment (ie, hip surgery).36
Discussion
We have presented the protocol for a registered, ethics-approved, randomized controlled trial of chiropractic management for the full lower limb kinetic chain for persons diagnosed with HOA. The participants of this study were diagnosed with HOA based on established ACR25 and Kellgren-Lawrence radiographic guidelines.26 They completed a short-term (9 visits), medium-term (3 months), and long-term (9 months) intervention of 1 of 2 protocols. Protocol A participants received treatment of the symptomatic hip only, whereas protocol B participants received treatment of the symptomatic hip as well as treatment of the lumbar spine and sacroiliac joints, knee, and foot complexes.
The Physiotherapy Evidence Database scale of criteria is used to rank research to determine the quality of each publication.37 This scale is scored on 11 criteria to give a score out of 10, with a rating of 9 to 10 considered excellent, 6 to 8 as good, 4 to 5 as fair, and 3 or less as poor methodological quality. The Physiotherapy Evidence Database scale is a validated scale and was developed by a Delphi Consensus by Verhagen et al.38 This study has been scored as a 9 out of 10, which is considered excellent. The study was unable to meet criterion 6, as therapists who administered treatment cannot be blinded.
Findings from this study may be important in the scope of treatment options for HOA beyond medication, exercise, and surgery. It may provide additional conservative management options before the need for surgical intervention. Sound methodology will provide results that are valid and reliable and may be used in treatment guidelines for HOA.
Limitations
Limitations exist in this study. Multiple chiropractic interns were involved in various aspects of this study, including physical assessment, diagnosis, and delivering treatment. The interns were specifically trained for this HOA study protocol and were supervised by licensed chiropractors employed by the tertiary institution. Arguments regarding the pros and cons of this approach have been discussed elsewhere; and it remains a possibility that even better outcomes could be secured by fewer, highly trained practitioners.18,21 Another limitation of using university outpatient clinics was closures. This resulted in some patients' return visits occurring over a slightly extended time frame (longer than 2 weeks).
Conclusion
This article outlines a study protocol that is currently being applied to an ethics-approved, registered, large-scale, internationally collaborated clinical chiropractic study. It is an example of sound research methodology that should be applied to future clinical chiropractic studies. The study compares the interventions of one-region vs multiregion (the lower limb kinetic chain) treatment of HOA. Findings of this study may be important in the scope of treatment options for patients and chiropractors and to provide evidence for inclusion in management guidelines for HOA.
Funding sources and potential conflicts of interest
The Cleveland Chiropractic College Los Angeles received $100 000 from the UniHealth Foundation, Los Angeles. The UniHealth Foundation is a nonprofit philanthropic organization whose mission is to support and facilitate activities that significantly improve the health and well-being of individuals and communities within its service area. No conflicts of interest were reported for this study.
References
- 1.Jacobs J. Osteoarthritis of the hip. A compendium of evidence-based information and resources. Am Acad Orthop Surg. 2003 [Google Scholar]
- 2.Lawrence R.C., Helmick C.G., Arnett F.C. Estimates of the prevalence of arthritis and selected musculoskeletal disorders in the United States. Arthritis Rheum. 1998;41:778–799. doi: 10.1002/1529-0131(199805)41:5<778::AID-ART4>3.0.CO;2-V. [DOI] [PubMed] [Google Scholar]
- 3.March L., Bagga H. Epidemiology of osteoarthritis in Australia. Med J Aust. 2004;180:S6–S10. doi: 10.5694/j.1326-5377.2004.tb05906.x. [DOI] [PubMed] [Google Scholar]
- 4.March L., Schwarz J., Carfrae B., Bagge E. Clinical validation of self-reported osteoarthritis. Osteoarthr Cartil. 1998;6:87–93. doi: 10.1053/joca.1997.0098. [DOI] [PubMed] [Google Scholar]
- 5.Arden N., Nevitt M. Osteoarthritis: epidemiology. Clin Rheumat. 2006;20:3–25. doi: 10.1016/j.berh.2005.09.007. [DOI] [PubMed] [Google Scholar]
- 6.Mathers C.D., Vos E.T., Stevenson C.E., Begg S.J. The burden of disease and injury in Australia. Bull W H O. 2001;79:1076–1084. [PMC free article] [PubMed] [Google Scholar]
- 7.Hawk C., Hyland J.K., Rupert R., Colonvega M., Hall S. Assessment of balance and risk for falls in a sample of community-dwelling adults aged 65 and older. Chiropr Osteopat. 2006;14:3. doi: 10.1186/1746-1340-14-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Orces C.H. Trends in fall-related mortality among older adults in Texas. Tex Med. 2008;104:55–59. [PubMed] [Google Scholar]
- 9.Rao S.S. Prevention of falls in older patients. Am Fam Physician. 2005;72:81–88. [PubMed] [Google Scholar]
- 10.Freemont A.J., Hoyland J.A. Morphology, mechanisms and pathology of musculoskeletal ageing. J Pathol. 2007;211:252–259. doi: 10.1002/path.2097. [DOI] [PubMed] [Google Scholar]
- 11.Suetta C., Aagaard P., Magnusson S.P. Muscle size, neuromuscular activation, and rapid force characteristics in elderly men and women: effects of unilateral long-term disuse due to hip-osteoarthritis. J Appl Physiol. 2007;102:942–948. doi: 10.1152/japplphysiol.00067.2006. [DOI] [PubMed] [Google Scholar]
- 12.Gillespie L.D., Robertson M.C., Gillespie W.J. Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2009;2:CD007146. doi: 10.1002/14651858.CD007146.pub2. [DOI] [PubMed] [Google Scholar]
- 13.Cameron I.D., Murray G.R., Gillespie L.D. Interventions for preventing falls in older people in nursing care facilities and hospitals. Cochrane Database of Syst Rev. 2010;1:CD005465. doi: 10.1002/14651858.CD005465.pub2. [DOI] [PubMed] [Google Scholar]
- 14.Deyle G.D., Allison S.C., Matekel R.L. Physical therapy treatment effectiveness for osteoarthritis of the knee: a randomized comparison of supervised clinical exercise and manual therapy procedures versus a home exercise program. Phys Ther. 2005;85:1301–1317. [PubMed] [Google Scholar]
- 15.van Baar M.E., Dekker J., Oostendorp R.A.B. The effectiveness of exercise therapy in participants with osteoarthritis of the hip or knee: a randomized clinical trial. J Rheumatol. 1998;25:2432–2439. [PubMed] [Google Scholar]
- 16.Pollard H., Ward G., Hoskins W., Hardy K. The effect of a manual therapy knee protocol on osteoarthritic knee pain: a randomised controlled trial. J Can Chiropr Assoc. 2008;52:229–242. [PMC free article] [PubMed] [Google Scholar]
- 17.Fish D., Kretzmann H., Brantingham J.W. A randomized clinical trial to determine the effect of combining a topical capsaicin cream and knee joint mobilization in the treatment of osteoarthritis of the knee. J Amer Chiropr Assoc. 2008;45:8–23. [Google Scholar]
- 18.Hoeksma H., Dekker J., Ronday H. Comparison of manual therapy and exercise therapy in osteoarthritis of the hip: a randomized clinical trial. Arthritis Rheum. 2004;51:722–729. doi: 10.1002/art.20685. [DOI] [PubMed] [Google Scholar]
- 19.Brantingham J., Williams A., Parkin-Smith G., Weston P., Wood T. A controlled, prospective pilot study into the possible effects of chiropractic manipulation in the treatment of osteoarthritis of the hip. Euro J Chiropr. 2003;51:149–166. [Google Scholar]
- 20.Hoskins W., McHardy A., Pollard H., Windsham R., Onley R. Chiropractic treatment of lower extremity conditions: a literature review. J Manip Physiol Ther. 2006;29:658–671. doi: 10.1016/j.jmpt.2006.08.004. [DOI] [PubMed] [Google Scholar]
- 21.Brantingham J.W., Globe G., Pollard H. Manipulative therapy of lower extremity conditions: expansion of a literature review. J Manip Physiol Ther. 2009;32:53–57. doi: 10.1016/j.jmpt.2008.09.013. [DOI] [PubMed] [Google Scholar]
- 22.Elbaz A., Mirovsky Y., Mor A. A novel biomechanical device improves gait pattern in patient with chronic nonspecific low back pain. Spine. 2009;34:E507–E512. doi: 10.1097/BRS.0b013e3181a98d3f. [DOI] [PubMed] [Google Scholar]
- 23.Moher D., Jones A., Lepage L. Use of the CONSORT statement and quality of reports of randomised trials: a comparative before and after evaluation. JAMA. 2001;285:1992–1995. doi: 10.1001/jama.285.15.1992. [DOI] [PubMed] [Google Scholar]
- 24.Begg C., Cho M., Eastwood E.L.S. Improving the quality of reporting of randomised controlled trials: the CONSORT statement. JAMA. 1996;276:637–639. doi: 10.1001/jama.276.8.637. [DOI] [PubMed] [Google Scholar]
- 25.Altman R., Alarcon G., Appelrouth D. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hip. Arthritis Rheum. 1991;34:505–514. doi: 10.1002/art.1780340502. [DOI] [PubMed] [Google Scholar]
- 26.Kellgren J.H., Lawrence J.S. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16:494–502. doi: 10.1136/ard.16.4.494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Reijman M., Hazes J.M., Pols H.A. Validity and reliability of three definitions of hip osteoarthritis: cross sectional and longitudinal approach. Ann Rheum Dis. 2004;63:1427–1433. doi: 10.1136/ard.2003.016477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Franke R.H., Kaul J.D. The Hawthorne experiments: first statistical interpretation. Am Sociol Rev. 1978;43:623–643. [Google Scholar]
- 29.McCarney R., Warner J., Iliffe S. The Hawthorne effect: a randomized controlled trial. BMC Med Res Methodol. 2007;7:30. doi: 10.1186/1471-2288-7-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.O'Meara E., Lewis E., Granger C. Patient perception of the effect of treatment with candesartan in heart failure. Results of the Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity (CHARM) programme. Eur J Heart Fail. 2005;7(4):650–656. doi: 10.1016/j.ejheart.2005.01.021. [DOI] [PubMed] [Google Scholar]
- 31.Chan L., Mulgaonkar S., Walker R., Arns W., Ambühl P., Schiavelli R. Patient-reported gastrointestinal symptom burden and health-related quality of life following conversion from mycophenolate mofetil to enteric-coated mycophenolate sodium. Transplantation. 2006;81(9):1290–1297. doi: 10.1097/01.tp.0000209411.66790.b3. [DOI] [PubMed] [Google Scholar]
- 32.Juniper E.F., Guyatt G.H., Willan A., Griffith L.E. Determining a minimal important change in a disease-specific Quality of Life Questionnaire. J Clin Epidemiol. 1994;47(1):81–87. doi: 10.1016/0895-4356(94)90036-1. [DOI] [PubMed] [Google Scholar]
- 33.Guyatt G.H., Juniper E.F., Walter S.D., Griffith L.E., Goldstein R.S. Interpreting treatment effects in randomised trials. BMJ. 1998;316(7132):690–693. doi: 10.1136/bmj.316.7132.690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Roos E., Klassbo M., Lohmander L. WOMAC osteoarthritis index. Reliability, validity, and responsiveness in participants with arthroscopically assessed osteoarthritis. Western Ontario and MacMaster Universities. Scand J Rheumatol. 1999;28:210–215. doi: 10.1080/03009749950155562. [DOI] [PubMed] [Google Scholar]
- 35.Lenth R.V. Java applets for power and sample size. SPSS Inc. headquarters, 233 S. Wacker Drive, Chicago, Illinois 60606 2006-9. http://www.stat.uiowa.edu/~rlenth/Power Available from:
- 36.Portney L., Watkins P. Foundations of clinical research: applications to practice. 3rd ed. Pearson Prentice-Hall; New Jersey: 2009. pp. 167–584. [Google Scholar]
- 37.Maher C.G., Sherrington C., Herbert R.D., Moseley A.M., Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83:713–721. [PubMed] [Google Scholar]
- 38.Verhagen A.P., de Vet H.C.W., de Bie R.A., Kessels A.G.H., Boers M., Bouter L.M. The Delphi list: a criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by Delphi consensus. J Clin Epidemiol. 1998;51:1235–1241. doi: 10.1016/s0895-4356(98)00131-0. [DOI] [PubMed] [Google Scholar]