

Abstract
Aim
This article examines whether the proportion of recanters increases (or decreases) as a function of time o test length of time theory.
Sample
2,221 US respondents in the National Longitudinal Survey of Youth child data. Bivariate and logistic regression analyses were used.
Results
Among recanters, 50% of cigarette and alcohol users recanted use by 4 years, and 50% of marijuana users recanted by 3 years. Predictors of recanting was being Black or Hispanic and younger age. The theory was not supported. Further research is needed to identify potential reasons why adolescents recant their use is such a short time span. The study’s limitations are noted.
Keywords: adolescent, self-report stability, alcohol, cigarette, marijuana, recanting, measurement, theory
BACKGROUND
In the physical and social sciences, measurement error has long been a key focus for methodologists (Schmidt & Hunter, 1999). Understanding biases related to measurement error is necessary to empirically and accurately test theories and hypotheses. All measures of constructs contain measurement error (Schmidt & Hunter, 1999); further, the relations we observe among two or more variables in research are typically between the measures we use and not the actual constructs. Thus, it is important that we have a clear understanding of the error associated with specificmethods of measurement. In psychometric theory, internal validity is the internal consistency of responses to the same (or similar) items when they are measured within time or across time (Barnea, Rahav, & Teichman, 1987). This is similar to the term reliability in the psychometric literature (Cronbach, 1947). Reliability studies frequently use the test–retest approach where joint or separate interviews are spaced days, weeks, or months apart, and responses are evaluated for agreement.
Survey research is largely dependent upon the ability of participants to recall details for a specific event such as when the episode occurred or the frequency of an event. The process of survey research has been examined from varying disciplines such as cognitive psychology (i.e., the impact of memory and judgment on the retrieval of information), linguistics (the communication and shared meaning of words), and survey methodology (Eisenhower, Mathiowetz, & Morganstein, 1991) to examine the underlying mechanisms of participant recall.
Length of time theory is one memory theory that posits that memories vary in their longevity. Friedman (1993) presented several types of memory for time. One set of theories can be classified as “strength theories.” Strength models assume that each memory has a unique strength that declines over time. Friedman (1993) conceptualizes the elapsed time between an event and the present time as “relative time.” Over time, one’s memory of any given event becomes weaker or less accurate. Hinrichs (1970) termed this as recall decay. Eisenhower et al. (1991) further discuss that recall decay is the inability to recall events that occur in the past or errors of omission. Thus, should this theory be accurate, then one would expect that in longitudinal, panel studies, participants would decrease in their accuracy of an event as time increases since the event.
Because much of the theoretical work in cognitive psychology regarding memory is based upon laboratory research, Jobe, Tourangeau, and Smith (1993) called for the examination and testing of memory theories in applied settings with methods such as survey research. The information gleaned from such studies can improve survey research methodologies as well as improve the information obtained from survey research.
The stability of adolescent substance use is an important issue to be addressed. Most prevention and intervention programs base recommendations on self-reported epidemiological data. Current epidemiological research suggests alcohol and other drug use among adolescents and young adults is pervasive. Lifetime prevalence rates of substance use, for instance, from the Monitoring the Future study, reveal that by 12th grade 48.4% used marijuana, 43.6% used cigarettes, and 72.3% have used alcohol. When examining the use of these substances for the past month, prevalence rates are 20.6% for marijuana, 43.5% for alcohol, and 20.1% for cigarettes in the past 30 days (Johnston, O’Malley, Bachman, & Schulenberg, 2010). Not only is alcohol and drug use pervasive, but it has also been linked to a number of health problems. Alcohol and other drug use has been linked with an increased risk in traffic accidents. Twenty two percent of fatal traffic crashes among youth aged 15–24 years involved a drunk driver (NSC, 2005; NHTSA, 2005), and poly substance use is a better predictor of crash risk than the use of a particular substance (Dunlop & Romer, 2010). Alcohol use has also been involved in sexual assaults (Buzy et al., 2004; Champion et al., 2004; McCauley et al., 2009), risky sexual behavior (Cooper, 2002; Dunn, Bartee, & Perko, 2003; Valois, Oeltmann, Waller, Hussey et al., 1999), suicide (Behnken, Yen-Chi, Temple, & Berenson, 2010; Bennett & Collins, 2000; Smith et al., 1999), truancy and bullying (Danielsson,Wennberg, Tengstrom,& Ramelsjo, 2010), and drowning (Driscoll, Harrison, & Steenkamp, 2004).
Fendrich and Vaughn (1994) reported the underreporting for marijuana and cocaine among National Longitudinal Study on Youth (NLSY) adults across a 4-year time span. They found that among adults, 19% of cocaine users and 12% of marijuana users denied their previously reported use 4 years later. Fendrich and Kim (2001) examined adult drug use recanting with a longitudinal design in 1988, 1992, and 1994. Specifically, they found 40% of cocaine users and 30% of marijuana users denied use in at least one follow-up period after prior reports of use. Fendrich and Rosenbaum (2003) reported recanting rates among teens in a Drug Abuse Resistance Education (DARE) program were 45% for alcohol use and about 50% for cigarette use. Kenkel, Lillard, and Mathios (2003) further studied the report stability for smoking cigarettes among the NLSY adults. Their findings indicated that about 11% of adult smokers recanted their use at a later wave of data collection up to 6 years from first reports of use. A study that examined recanting among adolescents found that across a 1-year period, 7% of alcohol users recanted use and 19% recanting drinking to intoxication, 10% recanted tobacco use, and 17% recanted marijuana use (Percy, McAlister, Higgins, McCrystal, & Thornton, 2005). Stanton, Papandonatos, Lloyd-Richardson, and Niaura (2007) identified a difference in recanting among different types of cigarette smokers across a 1-year follow-up. The range of recanting was 26.9% for light smokers to 5% for regular smokers.
Shillington and colleagues have examined adolescent substance use recanting with a national, panel study (Shillington & Clapp, 2000; Shillington, Clapp, & Reed, in press; Shillington, Clapp, Reed, & Woodruff, in press; Shillington, Reed, Clapp, & Woodruff, 2010). Their findings indicate that between 15% and 35% of adolescents deny their previously reported substance use at a later wave of data collection.
To date, no research has examined the stability of self-reported substance use among adolescents testing the length of time theory. The purpose of this study is twofold: (1) test the predictors of recanting in a large, diverse, population-based sample of children and adolescents and (2) test length of time theory by examining whether the proportion of recanters increases (or decreases) as a function of time.
METHOD
Data Source
We used self-report data collected from the children of women who participated in the NLSY79. Beginning in 1988 and continuing through 2006 the children (aged 10 years and older) of mothers who participated in the NLSY79 study answered a self-administered survey (biannually) covering sensitive topics such as substance use behaviors. Starting in 1994, two separate groups of children have been interviewed for the NLSY: (1) a group made up of children between the ages of 10 and 14 and (2) a group composed of adolescents aged 15 years or older. This older group is asked additional sets of questions not asked of the younger participants.
For the present analysis, we utilized data from the 1988–1998 NLSY surveys. Surveys after 1998 were redesigned to be computer assisted and had prior self-reported data already programmed in making the study of substance use recanting impossible. For example, if a respondent reported using cigarettes in 1998, the ever use of cigarettes would already be imbedded in the 2000 survey and the respondent would have no opportunity to rereport about lifetime use. Thus, for all surveys after 1998, respondents cannot recant the use of any substance.
Measures
The race and gender of each respondent was obtained from the 1979 mother’s screener survey. The NLSY uses three race/ethnicity categories: Black, Hispanic, and non-Black/non-Hispanic. For each survey year (1988–1998), both the child and adolescent surveys asked participantsif they had ever used cigarettes, alcohol, or marijuana (yes/no) and the age at which they first used these substances. We only included in our analyses age of first use values that were smaller than the participant’s chronological age when he or she first reported using a substance (i.e., we did not include an age of first use value of 18 if the participant’s chronological age at the time he or she was surveyed was 15).
We defined recanting (or a recanter) as a participant who reported ever using a substance (i.e., cigarettes, alcohol, or marijuana) at any wave in the survey and then denying that use in a later wave of the survey. For example, if a participant reported using cigarettes in the 1988 and 1990 surveys but then denied cigarette use in the 1992 survey, he/she would be defined as recanting cigarette use. Because a recanting variable could only be created for participants who responded to at least two survey waves, we did not include single-wave respondents in the present analysis. A recanting variable was created for each substance examined in this study (alcohol, tobacco, and marijuana). Recanting was a dichotomous (yes/no) variable.
Our main variable of interest for this study is the interval (number of years elapsed) between a participant’s age of first use of a substance and the year in which he or she recanted using the substance. Thus, if a participant reported an age of onset for cigarette use of 15 and then recanted using cigarettes in 1990 at the age of 20, the value of this variable would be equal to five. This variable was used to assess whether recanting increased as a function of this time interval.
Sample
The sample for the present study was composed of 2,221 respondents who had (a) reported ever using cigarettes or alcohol or marijuana and (b) had participated in two or more waves of the NLSY study. Nearly half of the sample was female (49%). Fewer than half of the sample was non-Black/non-Hispanic (39.6%) and 37.3% were identified as Black. Slightly less than one quarter of the sample was identified as Hispanic (23.1%).
Data Analyses
For this study, we focused on two analyses. The first analysis examined the predictors of recanting in our sample. The second analysis tested length of time theory and examined whether recanting the use of cigarettes, alcohol, and marijuana increased as a function of time.
Predictors of Recanting
In order to examine the predictors of recanting substance use within our sample, we first tested the bivariate associations between recanting for each substance examined and the following predictor variables: gender, race/ethnicity, and the first report of age of first use. The race/ethnicity variable was dummy coded into two variables: (1) Hispanic vs. non-Hispanic and (2) Black vs. non-Black. Because the more surveys in which a respondent participated increase the possibility of the respondent recanting, we also examined the bivariate association between recanting and the number of survey waves a respondent participated in. Variables with a significant association to recanting were then entered into three separate logistic regression models examining the predictors of recanting cigarette use, alcohol use, and marijuana use, respectively.
Length of Time and Recanting
For the analysis testing whether recanting increased as a function of time, we calculated the proportion of participants who recanted the use of each substance within 2 years, 3 years, 4 years, etc., of first reporting the use of a substance. We then used linear regression to test whether the proportion of recanters for each substance (i.e., three linear regression models) increased as a function of time. The interval (number of years elapsed) between a participant’s age of first use of a substance and the year in which he or she recanted served as our independent variable and the proportion recanting for each interval served as the dependent variable. The following covariates were also included in the regression models for each substance: the proportion of Black, Hispanic, and male participants, as well as the mean age of first use and mean number of surveys waves participated in. These covariates were aggregated for each of the recanting intervals—i.e., the proportion of Blacks recanting within 2 years, etc. We weighted each regression model by the sample size corresponding to each proportion in order to control for proportions based on small sample sizes.
RESULTS
Table 1 displays the percentage of respondents who reported using cigarettes, alcohol, or marijuana at least once in his or her lifetime. Nearly one half of the sample reported drinking alcohol, while slightly more than 40% reported smoking cigarettes. Slightly more than 1/4 reported using marijuana. The percentage of respondents who recanted their use of cigarettes, alcohol, and marijuana is also shown in Table 1. Almost 25% of the sample recanted using both cigarettes and alcohol; however, only 13% recanted marijuana use. Bivariate associations between each covariate and recanting the use of cigarettes, alcohol, and marijuana are shown in Table 2. A participant’s race/ethnicity and age of first use were significantly associated with recanting for all three substances. Specifically, Blacks and Hispanics were more likely to recant each substance compared with whites. Furthermore, recanting was significantly associated with a younger mean age of first use for cigarette, alcohol, and marijuana use than participants who did not recant the use of these substances. Males were more likely to recant cigarettes and alcohol; however, gender was not associated with recanting marijuana use. The mean number of waves the respondent participated in from 1988 to 1998 was significantly associated with recanting cigarette use. Specifically, participants who recanted using cigarettes participated in a higher mean number of surveys than those that did not recant cigarette use. There was no significant association between mean number of waves a respondent participated in and the recanting of alcohol or marijuana use.
TABLE 1.
The percentage of participants who ever used a substance and the percentage of participants who recanted using
| Percent ever use |
Percent recant |
|||
|---|---|---|---|---|
| Substance | Yes (%) | N | Yes (%) | N |
| Cigarettes | 40.7 | 1696 | 24.7 | 418 |
| Alcohol | 48.7 | 2042 | 24.8 | 507 |
| Marijuana | 26.2 | 1075 | 12.7 | 137 |
TABLE 2.
Bivariate associations between demographic variables, substance use variables, and recanting
| Recanted cigarette use Yes (%) |
Recanted alcohol use Yes (%) |
Recanted marijuana use Yes (%) |
|
|---|---|---|---|
| Gender | |||
| Male | 25.03* | 24.97** | 11.52ns |
| Female | 20.00 | 19.92 | 8.38 |
| Race/ethnicity | |||
| Black | 25.26*** | 20.31*** | 10.15** |
| Hispanic | 32.81 | 27.11 | 14.20 |
| non-Black, non-Hispanic | 13.48 | 19.11 | 6.27 |
| Age of first use Mean (SD) |
10.99 (2.69)*** | 10.39 (2.58)*** | 12.52 (2.74)*** |
| Total no. wave responses Mean (SD) |
4.13 (1.01)*** | 3.81 (1.07)ns | 3.86 (1.05)ns |
Note: ns, nonsignificant; SD, standard deviation.
p < .05.
p < .01.
p < .001.
The results of the three logistic regression analyses examining predictors of cigarette, alcohol, and marijuana use recanting are shown in Table 3. As shown in Table 3, Black and Hispanic respondents were significantly more likely to recant cigarette use than non-Black/non-Hispanic respondents. An older age of onset for cigarettes was associated with the lower odds of recanting use. Additionally, the odds of recanting cigarette use increased significantly with each additional survey wave in which a respondent participated. Gender was not significantly associated with recanting in the multivariate model. The sample size for marijuana recanting is smaller than that of cigarettes and alcohol given the lower prevalence of ever use relative to the other substances (see Table 1).
TABLE 3.
Results of logistic regression analyses modeling predictors of recanting (a) cigarette, (b) alcohol, and (c) marijuana use
| Variable | AOR | 95% CI | p value |
|---|---|---|---|
| Cigarettes | |||
| Female | 0.82 | 0.63–1.06 | ns |
| Black | 3.97 | 2.91–5.43 | <.001 |
| Hispanic | 2.75 | 1.95–3.88 | <.001 |
| Age of first use | 0.77 | 0.73–0.81 | <.001 |
| Total no. wave responses n = 1597 |
1.76 | 1.56–2.00 | <.001 |
| Alcohol | |||
| Female | 0.90 | 0.72–1.14 | ns |
| Black | 1.96 | 1.50–2.56 | <.001 |
| Hispanic | 1.39 | 1.01–1.90 | <.05 |
| Age of first use n = 1898 |
0.74 | 0.71–0.77 | <.001 |
| Marijuana | |||
| Black | 2.85 | <.001 | |
| Hispanic | 1.88 | <.05 | |
| Age of first use n = 1010 |
0.67 | <.001 | |
Note: CI, confidence interval: ns, nonsignificant.
The sample size for marijuana recanting is smaller than that of cigarettes and alcohol given the lower prevalence of ever use relative to the other substances (see Table 1).
Predictors of recanting alcohol use are displayed in Table 3. Similar to cigarette recanting, Black and Hispanic respondents were more likely to recant than non-Black/non-Hispanic respondents. If respondents were older when they first reported alcohol use, they were also less likely to recant. Participant gender was not associated with recanting alcohol use.
Table 3 shows the results of the logistic regression model predicting the recanting of marijuana use. Similar to the other models, Black and Hispanic participants were significantly more likely to recant marijuana use, and an older age of onset was significantly associated with a lower likelihood of recanting.
Figure 1 shows the percentage of participants who recanted the use of cigarettes, alcohol, and marijuana as a function of time. Results of the linear regression analysis revealed a significant relationship of time for the recanting of each substance; however, none of the covariates (proportion of Black and Hispanic participants, mean age of first use, and mean number of waves participated in) included in these regression analyses were significant. For cigarette use, more than 50% of participants recanted their use by 4 years and nearly 75% recanted by 6 years. The results of the linear regression showed a significant negative relationship between the percentage recanting cigarette use and time (β = −.742, p < .01). A similar pattern was observed for alcohol with nearly 50% recanting within 4 years and more than three-quarter recanting within 6 years. Furthermore, results of the linear regression analysis demonstrated a significant negative relationship between the percentage of participants recanting alcohol use and time (β = −738, p < .01). Fifty percent of marijuana users recanted within 3 years and more than 80% recanted by 8 years. The results of the linear regression between time and recanting marijuana use was also significant demonstrating a negative relationship between these variables (β =−.750, p < .05)
FIGURE 1.
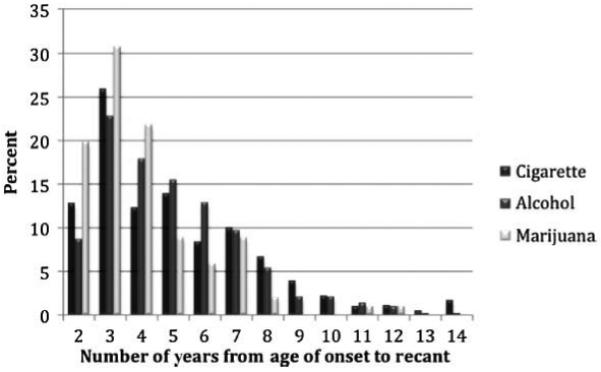
Percentage of participants recanting cigarette, alcohol, and marijuana use by time.
DISCUSSION
This study examined adolescent self-report stability and recanting of substance use using six waves of the NLSY data spanning 10 years. The length of time theory of recall decay was tested through these analyses. Recall decay posits that events in memory have a specific strength and that over time this strength decreases to the point of forgetting (error of omission). The findings from this study do not support this theory in that we found adolescents tend to deny or forget prior reported use of alcohol, cigarettes, and marijuana within the first few waves of follow-up interviews.
This study found, similar to prior research, that ethnic minority subgroups have higher rates of recanting compared with non-Black/non-Hispanic respondents (Fendrich & Kim, 2001; Fendrich & Rosenbaum, 2003; Fendrich & Vaughn, 1994; Shillington & Clapp, 2000; Stanton, et al., 2007). Johnson and Bowman (2003) discuss in-depth systematic sources of measurement error across ethnic and racial subgroups. They present a number of explanatory models such as cultural deficit model for poverty and education in that there may be a tendency to underreport drug use because of differing attitudes and values that are culturally influenced. The Cultural Conflict model posits that an individual would deny use because of concerns of mistrust, privacy, and confidentiality and, further, would underreport because of a concern about negative stereotypes. Another model discussed is one of conformity in which one would not report use because of social desirability and interviewer effects. The last model presented by Johnson and Bowman (2003) is that of cultural distrust. This would stem from historical experiences of mistreatment by the research community.
This study cannot support any of these explanations, but they could be possible explanations for the findings from this and a myriad of other prior alcohol and drug misuse research. However, these models are related to the denial of substance use and not recanting per se. Future research is needed however to investigate the degree to which any of these models may apply to substance use recanting per se, which may be different from denial of use in general. It is important, first, to note that the majority of those who reported use did not recant their use at a later time. Across all waves of data collection, it was found that about one fourth of alcohol and cigarette users recanted their prior reports of use and about 13% recanted prior marijuana use. The pattern for all three substances across 10 years of data collection was that 50%–70% of recanters recanted their use within the first 5 years after their first reported onset.
The findings indicate that independent of other covariates, the risk of denying use of all three substances studied is high within the first years of initial follow-ups. The pattern of recanting was similar across all three substances studied here.
Strengths and Limitations
The study design is a strength. It utilized a national, panel study with 2-year follow-up assessments spanning 10 years. With it we were able to examine report stability for use and test the length of time theory of recall decay. The large and ethnically diverse sample of youth, coupled with a very low attrition rate, allowed for detailed wave-to-wave analyses of specific ethnic groups over long periods. However, these data have limited external validity as the adolescents were born to younger mothers.
All secondary analyses are limited by the investigators’ inability to alter survey measures or study procedures. The NLSY was not designed explicitly to measure substance use. Nor was the survey designed with the intent to assess reliability issues. Furthermore, the data for this study were self-reports of use. There was no validation of the self-reported use by way of a saliva test for example and therefore should be interpreted with caution. The definition of race/ethnicity was a limitation, since the non-Black and non-Hispanic groups could be composed of a heterogeneous mix of cultural and ethnic groups.
Some of the report instability may be due to the issue of the youth’s interpretation of the questions. Children who reported prior use and denied it later may have reported “yes” to marijuana, for example, but had only a puff or two. Later denial may be a result from a decision that such use is not true use. Future research may examine this issue of question phrasing. The participants who recanted may have forgotten, or they may have decided they did not want their use to be “on record” by reporting it in a research study (particularly minority youth). Future research is needed that can probe participants when recanting takes place. Such probing could lead to a more in-depth understanding of motivations for denial or memory errors.
Future Research and Conclusions
The issue of recall decay and adolescent alcohol and substance use recanting needs to be examined within the context of a broader theoretical perspective regarding factors affecting the reporting of potentially sensitive behavior. In order to further contribute to the field and possibly improve adolescent survey research on alcohol and other drugs, there is a need to conduct qualitative research and longitudinal research. A theoretical framework, for a more in-depth understanding of report discrepancies, should guide such research of discrepancies as they occur. Furthermore, research is also needed to examine if adolescent self-report stability and recanting are impacted by the longitudinal trajectory of substance use patterns.
GLOSSARY
- Length of Time Theory
one memory theory that posits that memories vary in their longevity. Strength theories posit that each memory has a unique strength that declines over time.
- Report Stability
The consistency of self-reports of behaviors that necessarily cannot change. An example would be lifetime cigarette use. Once it is reported as positive, then one should always report “yes” for such use.
THE AUTHORS
Audrey M. Shillington is Professor at the San Diego State University, School of Social Work and Associate Director for the Center on Alcohol and Other Drug Studies. She received her Ph.D. from the Washington University. She was a Post-Doctoral Fellow at the National Institute of Mental Health and received a Master’s in Psychiatric Epidemiology from the School of Medicine at the Washington University. She has published over 50 peer-reviewed publications and been Principal Investigator and Coinvestigator on grants totaling over $6.5 million. Her research has focused on psychometrics and measurement of alcohol and drug use, as well as adolescent and young adult substance use prevention and interventions.
Dr. Mark B. Reed received his graduate training in Social Psychology from the University of Maryland, College Park. Dr. Reed has conducted research in the field of substance use prevention since 2000, and his current research interests include (1) genetic and environmental determinants of substance use/abuse and (2) the social and psychological risk/protective factors related to changes in adolescent/young adult substance use trajectories.
Dr. John D. Clapp is the Director of the Center for Alcohol and Drug Studies, Professor at the School of Social Work, Adjunct Professor for the Graduate School of Public Health, at the San Diego State University as well as the Director for the US Department of Educations, Higher Education Center. He received his Ph.D. from The Ohio State University in 1995, with a specialization in health and social science research methods. Dr. Clapp’s research interests are in the epidemiology and prevention of alcohol and other drug (AOD) problems, with an emphasis on person and environment interactions.
Susan I.Woodruff, Ph.D., is a Behavioral Epidemiologist and Professor at the School of Social Work at the San DiegoState University. She has over 25 years of experience in the area of health research, much of it with underserved, high risk, and understudied populations. Her primary area of interest over the past few years has been tobacco and drug use prevalence, risk factor assessment, and intervention. Dr. Woodruff has served as Principal Investigator, Coinvestigator, or Statistician on several large epidemiological and intervention studies focused on adolescents, including a randomized study testing an Internet virtual world chat room approach to smoking cessation for young smokers; an intervention study to reduce environmental tobacco smoke (ETS) in the home by providing smoking parents’ feedback about children’s level of hair nicotine; a prospective study of cultural risk factors for smoking among Latino adolescents; and a national multilevel assessment study of tanning salon use among adolescents.
Footnotes
Declaration of Interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the article.
REFERENCES
- Barnea Z, Rahav G, Teichman M. The reliability and consistency of self-reports on substance use in a longitudinal study. British Journal of Addiction. 1987;82:891–898. doi: 10.1111/j.1360-0443.1987.tb03909.x. [DOI] [PubMed] [Google Scholar]
- Behnken MP, Yen-Chi LL, Temple JR, Berenson AB. Forced sexual intercourse, suicidality, and binge drinking among adolescent girls. Addictive Behaviors. 2010;35:507–509. doi: 10.1016/j.addbeh.2009.12.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bennett AT, Collins KA. Suicide: A ten-year retrospective study. Journal of Forensic Sciences. 2000;45(6):1256–1258. [PubMed] [Google Scholar]
- Buzy WM, McDonald R, Jouriles EN, Swank PR, Rosenfield D, Shimek JS, et al. Adolescent girls’ alcohol use as a risk factor for relationship violence. Journal of Research on Adolescence. 2004;14(4):449–470. [Google Scholar]
- Champion HLO, Foley KL, DuRant RH, Hensberry R, Altman D, Wolfson M. Adolescent sexual victimization, use of alcohol and other substances, and other health risk behaviors. Journal of Adolescent Health. 2004;35(4):321–328. doi: 10.1016/j.jadohealth.2003.09.023. [DOI] [PubMed] [Google Scholar]
- Cooper LM. Alcohol use and risky sexual behavior among college students and youth: Evaluating the evidence. Journal of Studies on Alcohol. 2002;(Supp. 14):101–117. doi: 10.15288/jsas.2002.s14.101. [DOI] [PubMed] [Google Scholar]
- Cronbach LJ. Test reliability: Its meaning and determination. Psychometrica. 1947;12:1–16. doi: 10.1007/BF02289289. [DOI] [PubMed] [Google Scholar]
- Danielsson AK, Wennberg P, Tengstrom A, Ramelsjo A. Adolescent alcohol use trajectories: Predictors and subsequent problems. Addictive Behaviors. 2010;35:848–852. doi: 10.1016/j.addbeh.2010.05.001. [DOI] [PubMed] [Google Scholar]
- Driscoll TR, Harrison JA, Steenkamp M. Review of the role of alcohol in drowning associated with recreational aquatic activity. Injury Prevention. 2004;10(2):107–113. doi: 10.1136/ip.2003.004390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dunlop SM, Romer D. Adolescent and young adult crash risk: Sensation seeking, substance use propensity and substance use behaviors. Journal of Adolescent Health. 2010;46:90–92. doi: 10.1016/j.jadohealth.2009.06.005. [DOI] [PubMed] [Google Scholar]
- Dunn MS, Bartee RT, Perko MA. Self-reported alcohol use and sexual behaviors of adolescents. Psychological Reports. 2003;92(1):339–348. doi: 10.2466/pr0.2003.92.1.339. [DOI] [PubMed] [Google Scholar]
- Eisenhower D, Mathiowetz NA, Morganstein D. Recall error: Sources and bias reduction techniques. In: Biemer PP, Groves RM, Lyberg LE, Mathiowetz NA, Sudman S, editors. Measurement errors in surveys. Wiley; New York: 1991. pp. 127–144. [Google Scholar]
- Fendrich M, Kim JYS. Multiwave analysis of retest artifact in the National Longitudinal Survey of Youth drug use. Drug and Alcohol Dependence. 2001;62:239–253. doi: 10.1016/s0376-8716(00)00177-0. PII: S0376–8716(00)00177–0. [DOI] [PubMed] [Google Scholar]
- Fendrich M, Rosenbaum DP. Recanting of substance use reports in a longitudinal prevention study. Drug and Alcohol Dependence. 2003;70:241–253. doi: 10.1016/s0376-8716(03)00010-3. doi:10.1016/S0376–8716(03)00010–3. [DOI] [PubMed] [Google Scholar]
- Fendrich M, Vaughn CM. Diminished lifetime substance use over time. An inquiry into differential underreporting. Public Opinion Quarterly. 1994;58:96–123. [Google Scholar]
- Friedman WJ. Memory for the time of past events. Psychological Bulletin. 1993;113:44–66. [Google Scholar]
- Hinrichs JV. A two-process memory-strength theory for judgment in recency. Psychological Review. 1970;77:223–233. [Google Scholar]
- Jobe JB, Tourangeau R, Smith AF. Contributions of survey research to the understanding of memory. Applied Cognative Psychology. 1993;7:567–584. [Google Scholar]
- Johnson TP, Bowman PJ. Cross-cultural sources of measurement error in substance use surveys. Substance Use & Misuse. 2003;38:1447–1490. doi: 10.1081/ja-120023394. [DOI] [PubMed] [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the future national survey results on drug use, 1975–2009. Volume I: Secondary school students. National Institute on Drug Abuse; Bethesda, MD: 2010. p. 734. NIH Publication No. 10–7584. [Google Scholar]
- Kenkel D, Lillard DR, Mathios A. Smoke or fog? The usefulness of retrospectively reported information about smoking. Addiction. 2003;98:1307–1313. doi: 10.1046/j.1360-0443.2003.00445.x. [DOI] [PubMed] [Google Scholar]
- McCauley JL, Conoscenti LM, Ruggiero KJ, Resnick HS, Saunders BE, Kilpatrick DG. Prevalence and correlates of drug/alcohol-facilitated and incapacitated sexual assault in a nationally representative sample of adolescent girls. Journal of Clinical Child and Adolescent Psychology. 2009;2:295–300. doi: 10.1080/15374410802698453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Highway Traffic Safety Administration . Traffic safety facts 2004: Young drivers. National Center for Statistics and Analyses; Washington, DC: 2005. Report No. DOT HS 809 918. [Google Scholar]
- National Safety Council Fact sheets: Young drivers, 2004. 2005 Retrieved from http://www.nsc.org/library/facts/yngdrive.html.
- Percy A, McAlister S, Higgins K, McCrystal P, Thornton M. Response consistency in young adolescents’ drug use self-reports: A recanting rate analysis. Addiction. 2005;100:189–196. doi: 10.1111/j.1360-0443.2004.00943.x. doi:10.1111/j.1360-0433.2004.00943.x. [DOI] [PubMed] [Google Scholar]
- Schmidt FL, Hunter JE. Theory testing and measurement error. Intelligence. 1999;27:183–198. [Google Scholar]
- Shillington AM, Clapp JD, Reed MB. The stability of self-reported marijuana use across eight years of the National Longitudinal Survey of Youth. Journal of Child and Adolescent Substance Abuse. doi: 10.1080/1067828x.2011.614873. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shillington AM, Clapp JD, Reed MB, Woodruff SI. Adolescent Alcohol use self-report stability: A decade of panel study data. Journal of Child and Adolescent Substance Abuse. in press. [Google Scholar]
- Shillington AM, Clapp JD. Self-report stability of adolescent substance use: A first look at gender, ethnicity, and behavioral problems: Drug and alcohol dependence. An International Journal on Biomedical and Psychosocial Approaches. 2000;60(1):19–27. doi: 10.1016/s0376-8716(99)00137-4. [DOI] [PubMed] [Google Scholar]
- Shillington AM, Reed MB, Clapp JD, Woodruff SI. Self-report stability of adolescent cigarette use across 10 years of panel study data. Journal of Child and Adolescent Substance Abuse. 2010;19(2):171–191. doi: 1080/10678281003635089. [Google Scholar]
- Smith GS, Branas CC, Miller TR. Fatal nontraffic injuries involving alcohol:Ametaanalysis. Annals of Emergency Medicine. 1999;33(6):659–668. [PubMed] [Google Scholar]
- Stanton CA, Papandonatos G, Lloyd-Richardson EE, Niaura R. Consistency of slef-reported smoking over a 6- year interval from adolescence to young adulthood. Addiction. 2007;102:1831–1839. doi: 10.1111/j.1360-0443.2007.01974.x. doi:10.1111/j/1360-0443.2007.0194.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Valois RF, Oeltmann JE, Waller J, Hussey JR. Relationship between number of sexual intercourse partners and selected health risk behaviors among public high school adolescents. Journal of Adolescent Health. 1999;25(5):328–35. doi: 10.1016/s1054-139x(99)00051-8. [DOI] [PubMed] [Google Scholar]