

Abstract
Background:
Studies have shown that nearly 3% of closed head injuries result in basal ganglia hemorrhages and that this may be a more frequent occurrence in pediatric patients. Various mechanisms based on shearing forces have been implicated in the injury; however, the underlying mechanism leading to the increased incidence in pediatric patients has not been well described. Angiographic data suggest that putamenal perforators in children are more severely stretched at acute angles compared to those in adults, which may be a contributing factor to the increased incidence.
Case Description:
We discuss a series of five relatively benign cases of traumatic putamenal strokes in children and review their presentations, mechanism of injury, neurological deficits, and management with reference to available literature.
Conclusion:
Although generally an alarming situation, benign presentations of putamenal strokes may be seen in pediatric populations after closed head injuries. In such cases, conservative management with subsequent rehabilitation and physical therapy is recommended.
Keywords: Pediatrics, putamenal hemorrhages, closed traumatic brain injury, cerebrovascular trauma
INTRODUCTION
Nearly 3% of closed head injuries result in basal ganglia hemorrhages manifesting with the symptoms of severe head injury.[6,8] However, these have been described as a separate traumatic entity.[8] Others have reported that this may be a more frequent occurrence in pediatric patients.[7] Although generally an alarming situation, benign presentations of putamenal strokes may be seen in pediatric patients, with symptoms including nausea, vomiting, loss of consciousness, temporary amnesia, and headaches. The exact mechanism underlying the basal ganglia strokes, especially in the absence of other cerebral damage, is poorly understood; although various mechanisms based on shearing forces have been proposed. With improvements in diagnostic imaging capabilities, damage to the perforating vascular system especially the lenticulostriate and anterior choroidal arteries has been implicated in the etiology of traumatic putamenal strokes.
In this study, we discuss a short series of five cases of relatively benign presentations of traumatic putamenal strokes in children and review their presentations, mechanism of injury, neurological deficits, and management with reference to available literature [Table 1].
Table 1.
Clinical summary of cases with traumatic putaminal strokes
CASE REPORTS
Case 1
A 5-year-old girl presented to the emergency room (ER) with a history of fall from stairs (approximately 6-feet in height). She had immediate loss of consciousness which lasted for a 5 min. There was also a history of three episodes of vomiting on the way to the hospital, but no history of fits or bleeding from ear or nose after the injury.
On examination, she had a pulse rate of 82 beats per minute with a blood pressure of 115/76 mmHg. Her Pediatric Glasgow Coma Scale (GCS) was assessed to be 11/13, both her pupils were equal in size, and reaction to light. Her movements over the left half of her body were comparatively reduced with a power of 3/5 according to the Medical Research Council (MRC) scale. The rest of the neurological and systemic examination was within normal limits.
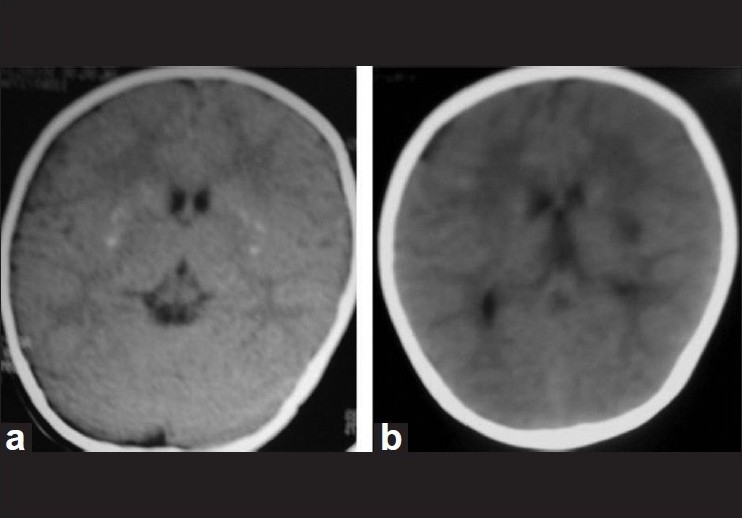
The initial brain computed tomography (CT) scan revealed a small ganglionic bleed associated with perifocal edema and a subtle mass effect [Figure 1a]. No other brain or intracranial lesions were noted.
Figure 1.
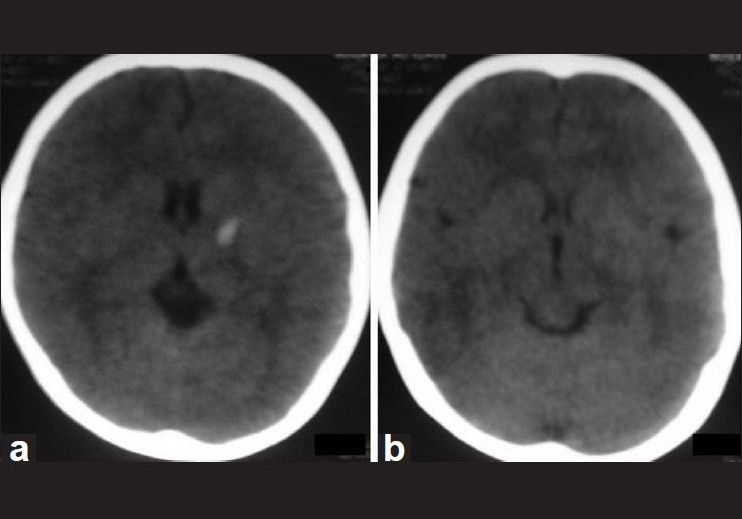
(a) The brain CT scan of case 1 showing a small ganglionic bleed with a subtle mass effect. (b) Repeat brain CT scan of the same patient showing resolving hematoma with subtle hypodensity
She was managed conservatively and her hemiparesis gradually improved. A_repeat CT scan at 2 weeks showed that the hematoma had almost resolved [Figure 1b]. She was started on regular physiotherapy and discharged 2 weeks later on a neurorehabilitation program.
At 6-month follow up, she had improved significantly, and regained a power of 5/5 in the affected limbs. Outcome assessed according to the Glasgow Outcome Scale (GOS) was 5.
Case 2
A 6-year-old boy was brought to the ER with a history of road traffic accident. He lost consciousness only briefly immediately after the episode and then had repeated episodes of vomiting. His history was negative for any fits or active bleeding from the ear or nose.
On examination, his pulse was 90 beats per minute with a blood pressure of 115/80 mmHg. His pediatric GCS was assessed to be 10/13, both his pupils were equal in size and reaction to light. He had a scalp laceration on the left parietal area, which had been appropriately sutured and dressed in ER. The patient also had left hemiparesis with a power of 3/5 in both upper and lower limb according to the MRC scale. The rest of the neurological and systemic examination was unremarkable.
The initial CT scan of the brain revealed a large hematoma in the left lentiform nucleus with perifocal edema [Figure 2a]. No other parenchymal injury, fractures, or midline shift were noted on the scan.
Figure 2.
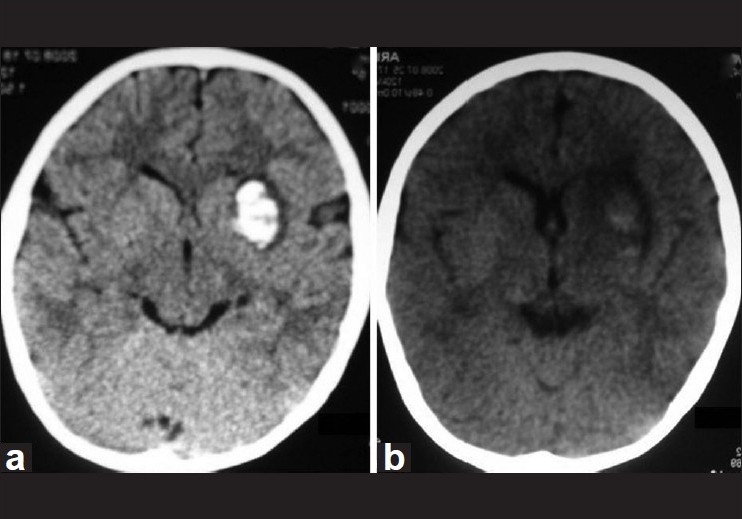
(a) The brain CT scan of case 2 showing a large left lentiform nucleus bleed with perifocal edema and mass effect. (b) Repeat brain CT scan of the same patient showing progressive resolution of the hematoma with decreasing mass effect
He showed clinical improvement on conservative management and became fully alert and conscious within 1 week. A repeat CT scan showed a resolving hematoma and surrounding edema [Figure 2b], and he was started on the regular rehabilitation program for hemiparetic children adopted at our hospital. At 4-month follow-up, the patient had regained functionality in the left side of his body (4/5 on MRC Scale) and was able to perform basic tasks. He had also begun to walk with minimum support using a walking frame and his GOS score at 4-month follow-up was 4.
Case 3
An 8-year-old boy was brought to ER with a history of road traffic accident in which he was hit by a motorbike. He had a history of temporary loss of consciousness followed by repeated episodes of nausea and vomiting. There were no complaints of bleeding from ear and nose or seizure like activity after the trauma.
On arrival, his pulse was 87 beats per minute and blood pressure was 115/75 mmHg. His GCS was 12/15, both his pupils were equal in size and reaction to light. There were no other neurological deficits and the rest of the examination was within normal limits.
The CT scan brain done on arrival showed a small hematoma in the area of right putamen with minimal perifocal edema, and no midline shift. The patient was managed conservatively and became fully conscious in 72 h.
He was started on regular physical therapy and discharged after 1 week with regular visits to our rehabilitation unit. At 4 month follow-up, he showed full neurological recovery without any residual deficits, and a GOS score of 5.
Case 4
A 7-year-old boy was brought to the ER after being involved in a road traffic accident, in which the car he was riding in rolled over. He had a history of loss of consciousness and repeated vomiting. There was no history of fits or bleeding from ear or nose.
On arrival his pulse was 95 beats per minute with a blood pressure of 95/60 mmHg. His GCS was 12/15, and both his pupils were equal in size and reaction to light. There was a 4-cm laceration on the patient's posterior parietal area on the right side. He had a left-sided hemiparesis with power of 3/5. The patient had a deformity of the right upper limb with suspected fracture of the humerus which was stabilized using a long arm back-slab. The rest of the_neurological and systemic examination was unremarkable.
The initial CT scan of the brain showed a large hematoma in right putamenal area with perifocal edema [Figure 3a]. There was associated mass effect and midline shift. An X-ray of the right humerus revealed a reduced fracture of humerus, which was immobilized in cast. The rest of the radiological survey was unremarkable. His scalp laceration was sutured and dressed in the ER.
Figure 3.
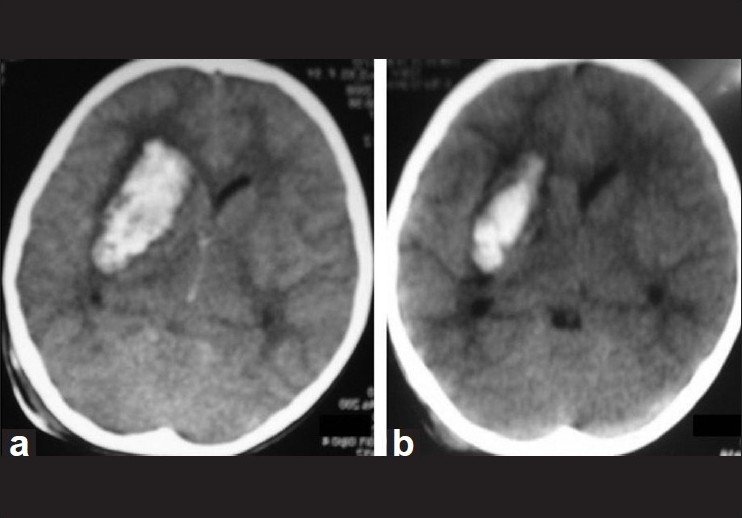
(a) The brain CT scan of case 4 showing a fairly large putamenal hematoma on the right side with mass effect and slight midline shift. (b) Repeat brain CT scan of the same patient showing resolving hematoma with perifocal hypodensity and reduced mass effect
The patient was managed nonoperatively with hypertonic saline in Pediatric Neuro-Intensive Care Unit for 24 h after which his imaging was repeated and he was shifted to step down unit, and started on regular limb physiotherapy. He was discharged home after a week on rehabilitation.
At 3-month follow up, he was able to perform basic tasks and was seen comfortably playing with a toy. He was also able to walk with support. A repeat CT scan showed an area of hypodensity with decreasing perifocal edema [Figure 3b]. He was advised to continue with physiotherapy and regular clinical follow-up. His recovery was not as good as the previous cases as he remained moderately disabled with a GOS score of 4 at 3-month follow-up.
Case 5
A 14-month male child presented to the ER with a history of fall from a bed (approximate height of 3 feet), after which he lost consciousness. He regained consciousness in about 2-3 min, and started to cry. On his way to the hospital, he had three episodes of vomiting. There was no history of seizure-like activity, or active bleeding from ear or nose.
On examination, his Pediatric GCS was 11/13 and his pupils were equal in size and reaction to light. There was a scalp swelling around the occipital area. He was noticed to have reduced movements over the right side of his body, with a power of 3/5. The rest of the examination was unremarkable.
The CT scan of his brain did not show any brain parenchymal injury 2 h after the incident [Figure 4a]. Repeat CT scan at 24 h showed a small hypodense area in the left putamenal area with surrounding mass effect but no midline shift. Clinical correlation of the CT scan confirmed an ischemic event of the area [Figure 4b].
Figure 4.
(a) The brain CT scan of case 5 at the time of admission showing no obvious parenchymal injury. (b) Repeat brain CT scan of the same patient showing an area of hypodensity in left putamen suggestive of ischemic parenchymal injury
He was managed conservatively with physiotherapy and subjected to regular follow-up. At 3 month follow-up he had a good recovery as he was able to walk with minimal support. His power on the affected side remained 4/5 at 3 months after the incident and his GOS score was 4.
DISCUSSION
Although the reported incidence is 3% in general population, traumatic putamenal strokes may be more common in the pediatric population. In previously reported studies almost all injuries leading to traumatic basal ganglia hemorrhages occurred in road traffic accidents with significant forces of impact and/or acceleration/deceleration sustained by the patient;[2,6] however, in our series we see minor traumatic incidents with falls from a height as low as 3 feet leading to symptomatic putamenal hemorrhages in children.
Several theories have been proposed to explain these injuries seen in this setting including occlusion, vasospasm, arterial emboli, dissection, thrombus formation, and vascular compression secondary to increased intracranial pressure.[1,3,4,10–12] These models have been supported by reports describing transient hemiparesis, in children, after minor trauma to the head with associated predominant faciobrachial neurological deficits. MRI findings in these patients include acute infarction of the internal capsule and corona radiata; however, no abnormalities were found in the large arteries on MRA most likely indicating an injury in the perforating arteries.[10,12] Due to the reversible nature of the hemiparesis, it was concluded that mechanical spasm of the perforating vessels might have played a role in the injury.[3,10,12]
However, traumatic dissection of perforating arteries might better explain underlying mechanism especially in hemorrhagic strokes.[11] The mechanism of injury proposed in such cases is traumatic rupture of the perforating arteries, chiefly the anterior choroidal artery or lenticulostriate artery leading to hemorrhage and ischemia of the affected area. Mosberg and Lindenberg considered that since the structures above the tentorium can move freely on impact when compared to the fixed structures below the tentorium there may be relative motion between the two causing stretch and shearing forces along the connecting structures, leading to multiple small hemorrhages.[9] These forces can also account for isolated basal ganglia hemorrhage without any other parenchymal injury. However, it may also be attributable to the sensitivity of different tissues to injury patterns as observed in experimental models.[5]
Following the previously reported data we compared the vascular anatomy of normal pediatric and adult patients undergoing cerebral angiography [Figure 5], in our center revealing that the arising perforators in the child were more tensely stretched at acute angles compared to the tortuously arising perforators in an adult as seen by Umansky et al. in their microanatomical study.[13] Considering the basic laws of physics the stretch of the perforators would automatically apply a certain amount of stress to the vessels; making them more prone to traumatic rupture and requiring lesser amount of force in order to do so. The findings of Mosberg and Lindenberg would also concur with this as the forces postulated by them would act in relatively the same plane as the tensile forces.[9]
Figure 5.
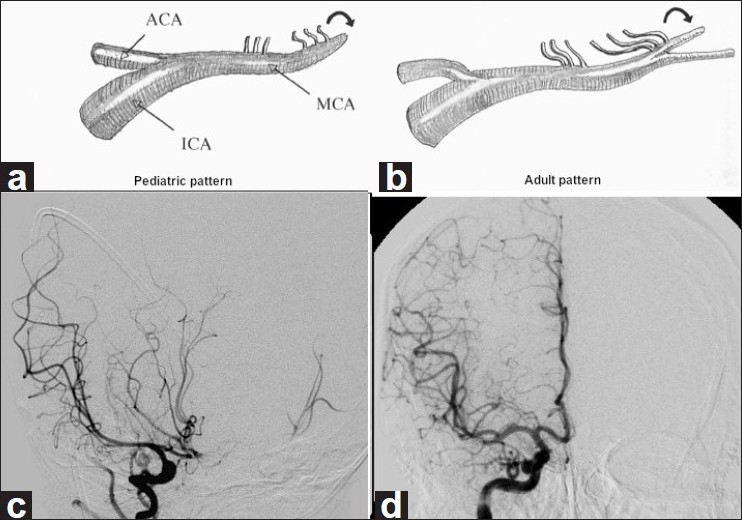
(a, b) Sketch on the top showing difference in angle of origin of lenticulostriate arteries from middle cerebral artery, more obtuse in the pediatric age group. A sample angiography in a pediatric case (c) and in an adult (d) confirming the findings as sketched
The absence of stretching forces along with the tortuous nature of the perforators [Figure 5] would protect the adult population from such traumatic hemorrhages in cases of minor trauma, making it a rare occurrence; however, the authors would like to point out that it may not be very rare in children and putamenal strokes should be kept in mind in cases of mild trauma involving children.
Although Boto et al. reported that the final outcomes were unfavorable in 84% of their patients, which showed no correlation with volume of the hematoma,[2] we found favorable outcomes in 100% of our patients on a long-term follow-up and neurorehabilitative measures. This may be due to the fact that our patients had relatively benign injuries and that the compliance and compressibility of brain tissue is higher in pediatric populations; leading to better tolerance of the mass effects of the hematoma.
We recommend that even though the contralateral hemiparesis may be an alarming sign, conservative management with rehabilitative physiotherapy be employed in children with relatively benign traumatic putamenal strokes.
Footnotes
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2011/2/1/51/80116
Contributor Information
Zain A. Sobani, Email: zsobani@gmail.com.
Arshad Ali, Email: doc4brains@yahoo.com.
REFERENCES
- 1.Ahn JY, Han IB, Chung YS, Yoon PH, Kim SH. Posttraumatic infarction in the territory supplied by the lateral lenticulostriate artery after minor head injury. Childs NervSyst. 2006;22:1493–6. doi: 10.1007/s00381-006-0157-9. [DOI] [PubMed] [Google Scholar]
- 2.Boto GR, Lobato RD, Rivas JJ, Gomez PA, de la Lama A, Lagares A. Basal ganglia hematomas in severely head injured patients: Clinicoradiologicalanalysis of 37 cases. J Neurosurg. 2001;94:224–32. doi: 10.3171/jns.2001.94.2.0224. [DOI] [PubMed] [Google Scholar]
- 3.Dharker SR, Mittal RS, Bhargava N. Ischemic lesions in basal ganglia in children after minor head injury. Neurosurgery. 1993;33:863–5. doi: 10.1227/00006123-199311000-00012. [DOI] [PubMed] [Google Scholar]
- 4.Endo M, Ichikawa F, Miyasaka Y, Yada K, Ohwada T. Capsular and thalamic infarction caused by tentorial herniation subsequent to head trauma. Neuroradiology. 1991;33:296–9. doi: 10.1007/BF00587809. [DOI] [PubMed] [Google Scholar]
- 5.Graham DI, Adams JH. Pathology of brain damage in head injury. Cooper PR Head Injury. 1997 [Google Scholar]
- 6.Katz DI, Alexander MP, Seliger GM, Bellas DN. Traumatic basal ganglia hemorrhage: Clinicopathologicfeatures and outcome. Neurology. 1989;39:897–904. doi: 10.1212/wnl.39.7.897. [DOI] [PubMed] [Google Scholar]
- 7.Levin HS, Grossman RG. Neurobehavioral consequences of closed head injury. Oxford University Press; 1982. [Google Scholar]
- 8.Macpherson P, Teasdale E, Dhaker S, Allerdyce G, Galbraith S. The significance of traumatic haematoma in the region of the basal ganglia. J NeurolNeurosurg Psychiatry. 1986;49:29–34. doi: 10.1136/jnnp.49.1.29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mosberg WH, Lindenberg R. Traumatic Hemorrhage from the Anterior Choroidal Artery. JNeurosurg. 1959;16:209–21. doi: 10.3171/jns.1959.16.2.0209. [DOI] [PubMed] [Google Scholar]
- 10.Nabika S, Kiya K, Satoh H, Mizoue T, Oshita J, Kondo H. Ischemia of the internal capsule due to mild head injury in a child. PediatrNeurosurg. 2007;43:312–5. doi: 10.1159/000103313. [DOI] [PubMed] [Google Scholar]
- 11.Okuno T, Takao T, Ito M, Konishi Y, Mikawa H, Nakano Y. Infarction of the internal capsule in children. J Comput Assist Tomogr. 1980;4:770–4. doi: 10.1097/00004728-198012000-00007. [DOI] [PubMed] [Google Scholar]
- 12.Seckin H, Demirci AY, Degerliyurt A, Dagli M, Bavbek M. Posttraumatic infarction in the basal ganglia after a minor head injury in a child: Case report. Turk Neurosurg. 2008;18:415–9. [PubMed] [Google Scholar]
- 13.Umansky F, Gomes FB, Dujovny M, Diaz FG, Ausman JI, Mirchandani HG, et al. The perforating branches of the middle cerebral artery. A microanatomical study. J Neurosurg. 1985;62:261–8. doi: 10.3171/jns.1985.62.2.0261. [DOI] [PubMed] [Google Scholar]