

Abstract
Medical mistakes that include medication errors have raised concerns about medication safety. Due to high consumption of medicines and self-treatment by all, especially the aging population, the issue of proper medication use and safety is at the forefront of public health concerns globally. Each country has a different approach towards medication event monitoring that is compliant with its own health care system. This paper focuses on the efforts and endeavors of some of the countries around the world to create an efficient error reporting systems to ensure public safety. Our analysis indicates that there are established and effective medication vigilance systems in many developed countries. The different countries undertake activities which range from collecting information about prescriptions, surveying physicians about adverse drug events, and conducting sophisticated post-marketing surveillance studies. There is still need for such sophisticated system in India; however recent promising developments are occurring towards building a medication vigilance system. Development of these systems may eventually contribute to a global medication vigilance system, which could reduce concern with medication errors and safety.
Keywords: Canada, Europe, India, medication error, role of communication, USA
The healthcare industry, where even the smallest mistake can have catastrophic implications, should not have any place or scope for errors. The Institute of Medicine defines medical errors as “the failure to complete a planned action as intended or the use of a wrong plan to achieve an aim”. Medical errors maybe of several types; however, the focus of this paper is mainly on medication errors. The United States National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP) defines a medication error as “any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the health care professional, patient, or consumer. Such events may be related to professional practice, health care products, procedures, and systems, including prescribing, order communication, product labeling, packaging, and nomenclature, compounding, dispensing, distribution, administration, education, monitoring and use”[1].
In 2003, NCC MERP provided their support for the ‘Principles for Patient Safety Reporting Programs’ designed and researched by 100 healthcare organizations nationwide. These comprise of creation of a safe environment, proper medication error data analysis, physician and patient confidentiality, information sharing among healthcare organizations, and federal protection of the people and the information associated with the medication error processing[2].
Two reports have caught the attention of all policy makers in the world, especially in the United States. A study conducted by Lazarou and co-workers showed that the incidence of serious and fatal adverse drug reactions (ADRs) in hospitalized patients was very high[3]. Another report issued by the Institute of Medicine (IOM) (“To Err is Human: Building a Safer Health System” [4]), estimated that 40,000 to 98,000 deaths per year in the US can be attributed to medical errors, making it the eighth leading cause of death[5]. Medication errors which can be categorized into prescribing errors, dispensing errors and administrative errors, accounted for 28% of all medical mistakes in the US, including serious and sometimes fatal complications. During the 5 y period after the IOM report, some surveys have been conducted to study the opinion of the healthcare professionals about patient safety. Although there have been discrepancies between them as to the use of which of the following among these would help in better patient safety, the overall findings suggest that increase in the staff population, use of efficient error detection systems, careful use of information technology, use of appropriate staff in intensive care units, may help achieve the purpose. Health care professionals, policy makers, federal agencies and the government need to work in harmony in order to gain public assurance, safety and trust[5]. In his book ‘Medication errors’, Cohen mentioned that the “five rights of safe medication use (the right patient, right drug, right time, right dose, and right route of administration)” focuses more on individual failures rather than system failures. About 5 y after the IOM report, the IOM committee is urging Agency for Healthcare Research and Quality (AHRQ) to fund research initiatives which focus more on medication error prevention techniques[6].
The issue of medication error is likely to be even larger from a global perspective. Given the magnitude of the problem, it is imperative to establish systems that consistently disclose potential errors, reduce risks, and alleviate the effects of errors. The institute of medicine report entitled “Crossing the Quality Chasm: A New Health System for the 21st Century” attributes medication errors to system failures or errors. The report asserts that reducing risk and ensuring safety require greater attention to systems[7]. The report accentuates the whole issue as a “system” problem, particularly taking into consideration the number of processes involved. Collapse at any one step of the system permits medication errors to occur. In most cases, an individual's performance is governed by the system; hence the system itself causes the error. Medication errors that result in catastrophic events may result from combined efforts of “latent failures” in the system and “active failures” by individuals working in that system[8]. Efforts are being made globally to establish systems capable of collecting accurate and relevant medication error data, which may provide valuable information needed to minimize medication-related errors.
MEDICATION SAFETY EFFORTS BY VARIOUS COUNTRIES
Canada:
Institute of Safe Medication Practices (ISMP) Canada is a non-profit organization established in 2000, which ensures safe use of medications, prevention of medication errors and regulates healthcare policies by collaborating with several national and international patient safety organizations worldwide along with ISMP US. Prior to this, individual hospitals had programs to report adverse drug events but an aggregation was missing. The absence of a large database also meant inability to identify rare and recurrent events. The Canadian Society of Hospital Pharmacists had also initiated a task force to explore various ways to initiate a national reporting program for medication errors[9]. ISMP Canada, Canadian Institute for Health Information (CIHI) and Health Canada have led to the development of Canadian Medication Incident Reporting and Prevention System (CMIRPS) which is concerned with reporting and prevention of medication error incidences all over the nation. In 2004, Canadian Coalition on Medication Incident Reporting and Prevention (CCMIRP), consisting of several healthcare institutions, agencies and societies formed the national Canadian Medication error reporting system (MERS)[10]. About 96% of the hospitals in Canada have a medication incident reporting system[11]. ISMP Canada and ISMP US have created internet accessible software called Analyze ERR which records, tracks and performs a root cause analysis of the medication error. In about 30 hospitals in Canada, Analyze ERR is being used to evaluate its performance[12].
Europe:
The European Foundation for the Advancement of Healthcare Practitioners (EFAHP) is a non-profit organization that promotes safe, effective and economic patient care by multi-disciplinary teams in Europe. It was founded in 1999 by an International Medication Safety Advisory Panel. The foundation is developing new roles for healthcare professionals, such as specialist nurses, clinical pharmacists, community pharmacists, and pharmacy technicians. The foundation facilitates these new roles by arranging multidisciplinary meetings, literature and networking. Its European Medication Error Reporting Program provides a uniform method to report medication errors. This program is useful in helping healthcare organizations and practitioners across Europe use medicines more safely. The foundation does not ask for patient's identification, although it requests the identity of practitioner reporting a medication error to verify the information. The names of practitioners, institutions and organizations that report medication error is kept confidential until the reporter's consent is obtained to reveal the identity. The EFAHP has initiated medication safety awareness which includes meetings organized on a national level. These meetings are open to nurses, physicians, pharmacists, and other healthcare professionals. EFAHP also communicates with pharmaceutical companies about advising them on changes to be made in their products, if their products result in ADR. EFAHP has established Steering Committees in various European countries, to look at the adverse drug event issues. Knowledge on local and current issues from the Committees will secure good interaction between the target groups. The local Steering Committees are in charge of the local medication safety awareness programs in the specified countries[13–15].
United states:
The United States Pharmacopoeia (USP) Medication Error Reporting Program (MERP) is a program in cooperation with the Institute of Safe Medication Practices. The MERP is a nationwide program wherein health professionals who come across actual or potential medication errors can make a report to the USP, and are assured confidentiality and anonymity[16]. MERP includes data for a wide variety of problems such as misinterpretations, miscalculations, misadministration, difficulty in interpreting handwritten orders, or misunderstanding verbal orders. Each of these reports are reviewed by the USP for health hazards and all the information is forwarded to the Food and Drug Administration (FDA) and the specific product manufacturer. USP acts as a liaison with the FDA and the manufacturer if a report is submitted anonymously.
To augment the USP MERP and MedWatch programs, the USP has launched MedMARx®, an Internet-accessible method for hospitals to anonymously report and track medication errors in a standard format[17]. This software program permits users to track errors both within their organization as well as from other anonymous organizations by searching an aggregate database. MedMARx helps hospitals to monitor the progress of their error prevention strategies and shares their success with other institutions and also helps them to be aware of problems and solutions reported by other institutions.
Apart from these national efforts for reporting medication errors, there are several internal institutional programs which request reporting of medication errors. It has been seen that these internal medication error reporting programs are far more successful than their counterpart national programs. The frequency of reporting to the FDA is remarkably low. For many ADRs, only 1% of those that occur are likely to be reported to the FDA. Many have attributed this to the voluntary nature of these reporting[18].
India:
Though the issue of medication error has attracted attention from several quarters of the world, there are some countries yet which do not have the essential medication error monitoring systems and are oblivious to the problems created by medication errors. However, efforts are now being taken in these countries, especially India, to set up a pharmacovigilance system, which can collect information on ADRs. In the recent years, India has seen the establishment of a society for pharmacovogilance, which aims at “establishing pharmacovigilance as a distinct and influential clinical discipline in India”[19]. India also has 30 pharmacovigilance centers funded by the World Bank. These centers are scanning instances of adverse drug reaction since January 2005. These 30 centers form a network of regional and peripheral centers at medical colleges in several states and are responsible for collecting and interpreting the data, and for reporting their findings to the drug controller general of India.
Evolution of the national pharmacovigilance program in India; doctors, hospital staff and hospitals:
In a study conducted by Ramesh et al. involving 110 doctors from 3 hospitals in the Mysore city, South India, where national reporting of hospital based ADRs was available, it was found that the national pharmacovigilance center created awareness about ADRs, benefited the patients and reporting was quite simple. Some of the factors that discouraged the doctors from reporting them were the well known reactions from the patients, mild reaction ADRs and the indication to immediately manage the ADRs. In spite of all this, doctors were interested in continuing the same system, educating the nurse staff, knowing more about rare ADRs in monthly meetings and bringing out a quarterly/monthly bulletin on ADRs[20]. Another study looked at ADRs in a rural tertiary care teaching hospital in Gujarat, India. The ADRs were observed prospectively and retrospectively for 600 patients suffering from various lung diseases. The study showed that pharmacovigilance improved the reporting of ADRs in the prospective study (3%) compared to retrospective study (1%). Both the studies show that pharmacovigilance encourages meticulous observation of ADRs by doctors and the hospital staff and improved reporting of the same[21].
The pharmacovigilance center staff:
Some of the major functions of a pharmacovigilance center are detecting and assessing signals for adverse drug reactions (ADRs) by conducting epidemiological and cohort studies in high risk populations, preventing ADRs by communicating it to everyone, withdrawing or issuing warnings about the drug entities in question and providing risk benefit assessments for optimum drug utilization[22]. A report published by the B. J. Medical School situated in Gujarat, India which houses a peripheral pharmacovigilance center describes the improvements and impediments that a typical pharmacovigilance center faces. These are summarized as in Table 1[23].
TABLE 1.
IMPROVEMENTS AND CHALLENGES OF TYPICAL PHARMACOVIGILANCE CENTERS[23]
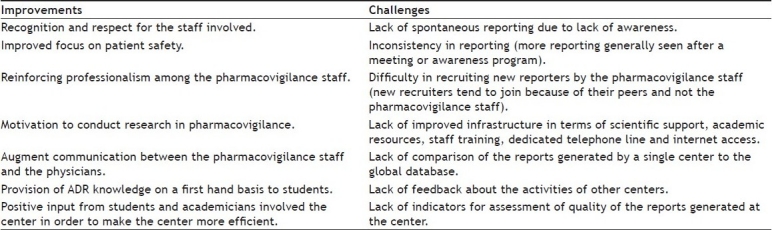
It is important to overcome the challenges faced by the pharmacovigilance centers by measuring their work performance on a periodic basis. Number of reports generated overall as well as per million population by the center, amount of valid reports generated and distributed by the center, number of people contributing to the reports, number of reports about specified drugs, number of regulatory or clinically significant signals generated, time required for the required regulatory actions or processes, conducting studies validating the reformations following the regulatory actions and provision of feedback and information to the reporters by publishing the data obtained from those studies are some of the performance indicators for evaluating pharmacovigilance centers that have been deduced by Kshirsagar and colleagues[22].
The pharmaceutical industry:
As the lag period between the release of drugs in the developed and the developing countries decreases, the non availability of the long term safety data of the drugs is becoming an increasing challenge. Along with the implementation of the National Pharmacovigilance Program in India, amendments have been made to the Schedule Y of the Drugs and Cosmetics Act 1945. These amendments concern the Indian pharmaceutical companies manufacturing generic drugs (monitoring and reporting spontaneous adverse drug reactions at regular intervals, preparation of periodic safety update reports, expedited reporting of serious unexpected adverse reactions, risk benefit analysis of the marketed products, safety data regulation and management and efficient signal detection) as well as those conducting clinical trials (pre defined regulatory timelines for error reporting and pre set conditions for expedited error reporting)[24]. The state of Maharashtra in India also centers the WHO's global network for post-marketing surveillance of pre-qualified vaccines. Generally, in the developing nations, there is a scarcity of post licensure safety data for pre-qualified vaccines which are introduced for use among the general population. The post marketing surveillance will enhance the monitoring of the safety of the vaccines[25]. Despite the establishment of the National Pharmacovigilance Program in Indian in 2004, some of the areas requiring attention are the integration of pharmacovigilance data and information in the public health programs, establishment of a national individual case safety report (ICSR) database and integration of the drug safety information obtained by the pharmaceutical industries with the benefits/harm assessments carried out by the Drugs Controller General of India (DCGI)[26].
THE NEXT STEP:COMMUNICATION OF DRUG SAFETY
Communication can prove to be an important tool to convey medication safety information. After the occurrence of an error, it is essential that the hospital discloses before their patients the true and complete nature of the error as to how, why, where and when it occurred and the necessary measures to be taken to avoid it in the future. However, disclosure should be made in such a way so as to keep the cultural norms and values of the patient in mind. A patient from US might react differently compared to a patient from India. Patients coming from developing countries might not be as well informed or curious as patients coming from developed nations. Efforts should be made to reduce language barriers and prevent the feeling of mistrust while the healthcare personnel are communicating with the victimized individual and his/her relatives. Emotional support and sympathy might be very helpful in helping the patient recuperate from the harmful consequences and trauma suffered as a result of the medical mishap[20]. It is essential that the overuse, underuse and misuse of the medication be prevented[21]. The increase in patient willingness to take new drugs coupled with increased direct to consumer advertising has overwhelmed existing ability of global systems to detect, act upon, and disseminate information about potential medication errors in a timely manner, culminating in many “communication mishaps”. Any “message” must be received, understood, and acted upon appropriately before any claims are made on the success of the communication. This is particularly important in countries like India, where many medications can often be obtained from a drug store without the actual prescription of the physician.
The Erice report of 1997 recommends that information about the medications be exchanged transparently between the physician and the patient. According to the report, each and every aspect about the drug should be discussed and answered credibly by the concerned healthcare personnel. The physician should share adequate knowledge about the risks and benefits of the intake of medications to make the patient aware of the consequences of the drug therapy. Physicians must help the patients clarify uncertainties if any, about any medication. It always helps if the physicians are up to date about their knowledge with proper evidence on any particular drugs whose safety is being questioned and it is their moral duty to convey this information to the patients in order to ensure public safety. An efficient error reporting system which can help aggregate all the information on medication errors occurring nationwide and keep the public informed should be highly recommended. Long term medication safety monitoring will help to keep the consumers aware of the harmful and beneficial implications of their drug regimen[22,23,24,25]. It is also important to standardize terminologies. In their recent report, the USFDA has mentioned the measures that they are taking to ensure that drug safety information is being communicated properly to the public. For fear of discontinuing a beneficial drug, USFDA takes several factors into consideration prior to communicating the emergent medication safety information resulting out of post marketing surveillance. Some of these factors are data reliability, how serious is the adverse drug event, correlation of the drug to the adverse event, popularity of the drug, its effect on the market, how it affects the children and the elderly and the corrective measures that can be taken to prevent further harm. USFDA uses several means for communicating drug safety information like proper labeling on prescription drugs for the healthcare providers, labeling on over the counter (OTC) products for the consumers, package inserts in medicines for the patients describing summarized information about the safety of that particular drug, public health advisories for the common people in order to inform about the emerging drug safety information, patient information sheets for the consumers describing information about newly approved drugs, healthcare professional sheets for the physicians which give emerging drug safety information, and alerts, thereby helping them to make informed clinical decisions, and lastly, alerts on patient information and healthcare professional sheets to inform both the consumers and providers about any changes that have to be made on the labeling due to emerging safety information available[26].
DISCUSSION
Medication errors are a common occurrence in every healthcare institution and organization. They are a result of a system failure rather than an individual failure. The process of achieving substantial control over medication errors by building a comprehensive and integrated global medication error reporting system is complex, futuristic and comprised of many challenges and hurdles. Although some extant systems in North America and Europe are collecting information on medication error events, there is still need of such sophisticated system in India. In addition to a pharmacovigilance centre in India, a national internet assessable error reporting software like the ones prevalent in the western countries, regulatory policies involving the usage of allopathic and alternative medications used in non allopathic systems like Ayurveda, Unani, Siddha and Homeopathy, proper training of healthcare professionals and increased awareness might yield in better medication error data aggregation and help combat the problem of insufficient post surveillance data on newly marketed and existing drugs as a result of decrease in drug lag between India and the western countries[27].
India should focus squarely here, especially during the post marketing phase on risk detection and risk management. This would involve identifying appropriate methodologies to examine risk. The information thus obtained, should then be disseminated to all concerned (prescribers, dispenser, and patients). The post-marketing surveillance programs from the countries mentioned earlier have considerable variations among themselves and each of these systems has their strengths and weaknesses. Fear of malpractice claims faced by the healthcare professionals lead to under reporting of the errors, mistrust and skepticism towards the society and drug regulatory authorities. An environment, where the physicians are free of the fear of loss of autonomy and their professional credibility being challenged, should be fostered.
Another problem that maybe associated with the current surveillance involves underestimation of the true incidence rate of medication errors. The populations at risk are often unknown. Regulatory approach on drug safety monitoring focuses solely on new and/or unexpected adverse medication events. Mostly, only these are reported to the regulatory agency. However, majority of the 100,000 drug-related deaths in the U.S. are due to “expected” drug reactions and medication errors that are not required to be reported to the regulatory agency. According to a report in Journal of the American Medical Association, the drug safety data should be reviewed carefully by the FDA every 5 y so that the necessary changes can be made to the medication labeling. The FDA must increase the drug safety monitoring staff that should be also able to take post marketing regulatory actions. Also newly approved drugs which are marketed should carry a particular sign or symbol for identification for a minimum period of 2 years so that the patients and the physicians are aware of the potential risks involved in taking that particular drug[21]. Healthcare is a diversified field comprising of a myriad and complex professional hierarchy, infrastructure, policies, rules and regulations. A proper leadership which fosters a work culture of safety from the grass root to the acme of a healthcare organization is essential[28].
Acknowledgments
This work was not supported by any financial source. The authors acknowledge research assistance provided by Dr. Rahul Shenolikar and Dr. Amit Kulkarni on this manuscript.
Footnotes
Patel and Balkrishnan: Medication Error Systems Across the Globe
REFERENCES
- 1.National coordinating council for medication error reporting and prevention. About Medication Errors. [updated on 2008 Jan 8]. Available from: http://www.nccmerp.org/aboutMedErrors.html .
- 2.National coordinating council for medication error reporting and prevention. [updated on 2008 Jan 8]. Press Releases. Available from: http://www.nccmerp.org/press/press2003-11-25.html .
- 3.Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA. 1998;279:1200–05. doi: 10.1001/jama.279.15.1200. [DOI] [PubMed] [Google Scholar]
- 4.Kohn LT, Corrigan JM, Donaldson MS. Institute of Medicine. To Err is Human: Building a Safer Health System. Washington DC: National Academy Press; 2000. [PubMed] [Google Scholar]
- 5.Altman DE, Clancy C, Blendon RJ. Improving patient safety--five years after the IOM report. N Engl J Med. 2004;351:2041. doi: 10.1056/NEJMp048243. [DOI] [PubMed] [Google Scholar]
- 6.Burke JP. Medication Errors. N Engl J Med. 2007;357:624. [Google Scholar]
- 7.Institute of Medicine. Crossing the Quality Chasm: A New Health System for then 21st Century. Washington DC: National Academy Press; 2001. [PubMed] [Google Scholar]
- 8.Batalden PB, Mohr JJ. Building knowledge of health care as a system. Qual Manag Health Care. 1997;5:1–12. [PubMed] [Google Scholar]
- 9.Orser B. Reducing medication errors. CMAJ. 2000;162:1150–51. [PMC free article] [PubMed] [Google Scholar]
- 10.Council of Europe. Creation of a better medication safety culture in Europe: Building up safe medication practices 2006. [updated on 2008 Nov 15]. Available from: http://www.coe.int/t/e/social_cohesion/soc-sp/medication%20safety%20culture%20report%20e.pdf .
- 11.2005/06 Annual Report - Hospital Pharmacy in Canada. Ethics in Hospital Pharmacy. [updated on 2008 Nov 15]. Available from: http://www.lillyhospitalsurvey.ca/hpc2/content/2006_report/mentalhospitals.pdf .
- 12.David U. Medication error reporting systems: Problems and Solutions. New Medicine. [updated on 2008 Nov 15]. Available from: http://www.ismpcanada.org/download/Medication%20Error%20Reporting%20Systems%20-%20Problems%20and%20Solutions.pdf .
- 13.European Foundation for the Advancement of Health Practitioners. [updated on 2008 Nov 17]. Available from: http://www.efahp.org/v2/about/about.php .
- 14.Castot A. The French pharmacovigilance system. Bratisl Lek Listy. 1998;99:29–30. [Google Scholar]
- 15.Centre for Adverse Reactions Monitoring, New Zealand. [updated on 2008 Nov 17]. Available from: http://carm.otago.ac.nz/CARM.asp .
- 16.USP. USP medication error reporting program. [updated on 2008 Dec 1]. Available from: http://www.usp.org/patientSafety/reporting/mer.html .
- 17.The Institute for Safe Medication Practices. USP launches MedMARx® as the third major national reporting program for adverse drug events. [updated on 2008 Dec 1]. Available from: http://www.ismp.org/MSAarticles/MedMARx.html .
- 18.Balkrishnan R, Furberg CD. Developing an optimal approach to global drug safety. J Intern Med. 2001;250:271–9. doi: 10.1046/j.1365-2796.2001.00883.x. [DOI] [PubMed] [Google Scholar]
- 19.Society of Pharmacovigilance, India. [updated on 2008 Dec 3]. Available from: http://www.medbeats.com/sopi.html .
- 20.Ramesh M, Parthasarathi G. Adverse Drug Reactions reporting: Attitudes and perceptions of medical practitioners. Asian J Pharm Clin Res. 2009;2:10–4. [Google Scholar]
- 21.Gor AP, Desai SV. Adverse drug reactions (ADR) in the inpatients of medicine department of a rural tertiary care teaching hospital and influence of pharmacovigilance in reporting ADR. Indian J Pharmacol. 2008;40:37–40. doi: 10.4103/0253-7613.40488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kshirsagar NA, Olsson S, Ferner RE. Consideration of the desirable features and possible forms of practical indicators of the performance of pharmacovigilance centers. Int J Risk Saf Med. 2010;22:59–66. [Google Scholar]
- 23.Dikshit RK, Desai C, Desai MK. Pleasures and pains of running a pharmacovigilance center. Indian J Pharmacol. 2008;40:S31–S4. [PMC free article] [PubMed] [Google Scholar]
- 24.Arora D. Pharmacovigilance obligations of the pharmaceutical companies in India. Indian J Pharmacol. 2008;40:S13–S6. [PMC free article] [PubMed] [Google Scholar]
- 25.UR 48, Uppsala reports January 2010, The Uppsala monitoring center, Sweden. [updated on 2010 Aug 15]. Available from: http://www.who-umc.org/graphics/22435.pdf .
- 26.UR 46, Uppsala reports July 2009, The Uppsala monitoring center. [updated on 2010 Aug 15]. Available from: http://www.who-umc.org/graphics/21039.pdf .
- 27.Leape LL, Woods DD, Hatlie MJ, Kizer KW, Schroeder SA, Lundberg GD. Promoting patient safety by preventing medical error. JAMA. 1998;280:1444–7. doi: 10.1001/jama.280.16.1444. [DOI] [PubMed] [Google Scholar]
- 28.Kuehn BM. IOM: overhaul drug safety monitoring. JAMA. 2006;296:2075–6. doi: 10.1001/jama.296.17.2075. [DOI] [PubMed] [Google Scholar]
- 29.The ERICE Declaration On Communicating Information Drug Safety. [updated on 2008 Dec 3]. Available from: http:/www.prescrire.org/docus/ericeEn.pdf .
- 30.Wood AJ. The safety of new medicines: the importance of asking the right questions. JAMA. 1999;281:1753–4. doi: 10.1001/jama.281.18.1753. [DOI] [PubMed] [Google Scholar]
- 31.Herxheimer A, McPherson A, Miller R, Shepperd S, Yaphe J, Ziebland S. Database of patients’ experiences (DIPEx): a multi-media approach to sharing experiences and information. Lancet. 2000;355:1540–3. doi: 10.1016/S0140-6736(00)02174-7. [DOI] [PubMed] [Google Scholar]
- 32.Bowdler J. Effective communications in pharmacovigilance: The Erice Report. Birmingham, England: W Lake Limited; 1997. [Google Scholar]
- 33.U.S. Food and Drug Administration. Center for Drug Evaluation and Research (CDER). Guidance Drug Safety Information – FDA’s Communication to the Public. [updated on 2008 Dec 3]. Available from: http://www.fda.gov/cder/guidance/index.htm .
- 34.Gogtay N, Dalvi S, Kshirsagar N. Safety monitoring: An Indian perspective. Int J Risk Saf Med. 2003;16:21–30. [Google Scholar]
- 35.Leape LL, Berwick DM. Five Years After To Err Is Human: What Have We Learned? JAMA. 2005;293:2384–90. doi: 10.1001/jama.293.19.2384. [DOI] [PubMed] [Google Scholar]