

Abstract
Background
Evidence about a possible causal relationship between non-specific physical symptoms (NSPS) and exposure to electromagnetic fields (EMF) emitted by sources such as mobile phone base stations (BS) and powerlines is insufficient. So far little epidemiological research has been published on the contribution of psychological components to the occurrence of EMF-related NSPS. The prior objective of the current study is to explore the relative importance of actual and perceived proximity to base stations and psychological components as determinants of NSPS, adjusting for demographic, residency and area characteristics.
Methods
Analysis was performed on data obtained in a cross-sectional study on environment and health in 2006 in the Netherlands. In the current study, 3611 adult respondents (response rate: 37%) in twenty-two Dutch residential areas completed a questionnaire. Self-reported instruments included a symptom checklist and assessment of environmental and psychological characteristics. The computation of the distance between household addresses and location of base stations and powerlines was based on geo-coding. Multilevel regression models were used to test the hypotheses regarding the determinants related to the occurrence of NSPS.
Results
After adjustment for demographic and residential characteristics, analyses yielded a number of statistically significant associations: Increased report of NSPS was predominantly predicted by higher levels of self-reported environmental sensitivity; perceived proximity to base stations and powerlines, lower perceived control and increased avoidance (coping) behavior were also associated with NSPS. A trend towards a moderator effect of perceived environmental sensitivity on the relation between perceived proximity to BS and NSPS was verified (p = 0.055). There was no significant association between symptom occurrence and actual distance to BS or powerlines.
Conclusions
Perceived proximity to BS, psychological components and socio-demographic characteristics are associated with the report of symptomatology. Actual distance to the EMF source did not show up as determinant of NSPS.
Background
Technological development does not only improve people's quality of life but is often accompanied by increased worry about potential health effects related to environmental exposures [1]. A considerable part of the general population does not only express serious concerns but also attributes various health complaints and symptoms to relatively low-level exposure to Electromagnetic fields (EMF), emitted by sources such as mobile phone devices, base stations and powerlines [2-5]. This phenomenon of symptom attribution to EMF exposure is often referred to as "Electromagnetic Hypersensitivity" (EHS) and more recently as "Idiopathic Environmental Intolerance attributed to Electromagnetic Fields" (IEI-EMF) [6].
According to the World Health Organization (WHO) IEI-EMF is characterized by physical symptoms such as redness, tingling and burning sensations in the face, fatigue, tiredness, lack of concentration, dizziness, nausea, heart palpitation and digestive disturbances [7]. These complaints are estimated to be prevalent in 1.5% of the general population in Sweden [2], 3.2% in California [8], 5% in Switzerland [3], 3.5% in Austria [4] and 10.3% in Germany [5] and seem to be frequently accompanied by occupational, social and mental impairment [9,10]. Age, gender, education, occupational status and ethnicity have been recognised as stable predisposing factors for the NSPS attributed to EMF [2,3,5,11].
Results from well-designed epidemiological studies indicate no consistent associations between various symptoms and residential EMF exposure [12-16]. Recent reviews strengthen the aforementioned evidence, concluding that a causal relationship between health complaints and exposure to EMF cannot be adequately and consistently supported [17-19]. Additionally, the need of improvement in major methodological aspects such as exposure characterization, symptom assessment, study design, population selection, sample size and the investigation of possible confounders has been highlighted. Since the causes of EMF-attributed symptoms are unspecified and so far there is a lack of objective findings that could support a causal mechanism, these subjective complaints belong to the domain of the so-called "Non-specific physical symptoms" or "Medically Unexplained (Physical) Symptoms" which are often attributed to environmental exposures [20]. In the current paper the term "Non-specific physical symptoms" (NSPS) is used to refer to the symptoms, as a broader and more neutral term which does not imply a link with particular etiologic agents, especially since similar symptoms are very common in the general population [21].
The most recent systematic review focusing (exclusively) on experimental evidence was based on the examination of 46 studies involving 1117 subjects [19]. It was suggested that symptoms attributed to EMF might be a result of underlying psychological processes related to the nocebo effect. The latter reflects the triggering of symptoms under blind experimental conditions, due to individual's expectations of harmful health effects produced by a sham exposure source. Perceived exposure to EMF sources such as BS might be associated with elevated symptom scores [22] and could comprise an important element in this process; the subjective belief of being exposed to a hazardous source can reinforce the alertness for the presence of potential exposure indicators, the expectations of symptom occurrence and consequently the development and report of symptoms [23].
Although a number of studies have accentuated the role of psychological factors in unexplained environmental intolerances [23-28] evidence regarding a psycho-physiological process underlying this phenomenon is still scarce and consensus on a conceptual framework is lacking. In view of the possible overlap between diverse environmental sensitivities [29], it is also questionable whether IEI-EMF constitutes a unique condition or should be considered as a part of a broader syndrome. It has been shown that subjects with IEI-EMF report increased self-reported sensitivity to several other environmental stressors apart from EMF [2].
Approaches from the area of health psychology support the notion that investigation of both the individual and environmental context can elucidate the mechanisms behind the occurrence of ill health, including socioeconomic, geographic, demographic and psychological components [30]. In line with this perspective, research in environmental epidemiology has indicated that NSPS attributed to environmental exposures might be the result of an interaction between biological, psychological and social pathways [31].
This exploratory study aims to a better understanding of the pathways through which exposure to EMF could be associated with increased report of non-specific physical symptoms, by introducing potential determinants and moderators of this relationship. More specifically, adjusting for demographic, home and area characteristics, the present analysis was performed to subsequently test:
• Whether actual (objectively measured) distance and perceived (self-reported) proximity to BS are associated with report of NSPS, controlling for actual and perceived proximity to powerlines.
• The impact of psychological components such as self-reported environmental sensitivity, lack of perceived control and coping styles (problem oriented versus avoidance) on NSPS report.
Methods
Selection and recruitment
The study makes use of data which were collected in 2006 in the Netherlands. Residents were selected from twenty two residential areas with varying levels of urbanization, socioeconomic status (SES) and clustering of environmental problems (air pollution, noise and green area).
After selecting areas with contrasting levels of urbanization, SES and accumulation of environmental problems (irrelevant to EMF), a random sample of inhabitants age 18 and over was drawn via the registration offices of the selected municipalities. More people from one household could be selected. The initial (gross) sample consisted of N = 9502 persons. In the period between May-September 2006, people were invited to participate in a study about environmental quality, residential satisfaction and subjective health by either filling out a written questionnaire or a web based version. A small reward of 5 Euros was offered for participation. A press report was released in local newspapers. Two reminders were sent to non-responders. The total response rate was 37% (N = 3611). Among the respondents, 85% used the written questionnaire, while 15% participated via the website. For each included neighbourhood, an equal number of non-respondents was extracted; short telephone interviews were performed for this non-response group (N = 255, response rate: 41%) in order to determine the degree of selection bias.
The questionnaire data from the full sample were used in the current study, after linking the home addresses of the respondents to the location of BS and powerlines.
Ethics
The current study was approved by the Dutch Medical Ethics Review Committee (METC). The data set was collected in 2006 following the privacy guidelines of the Dutch Privacy Law regarding the use of personal data (WBP) of the National Institute for Public Health and the Environment. All data were treated anonymously and confidentially.
Procedure
The 3611 respondents lived at 2921 different addresses, determined by zip/postal code, house number and an optional house number extension. These were matched with the Address Coordinate File Netherlands (ACN) of the Dutch Land Registry which contains all the addresses of the Dutch dwellings as well as the Dutch standard co-ordinates of the dwellings. Records of the Antenna Bureau of the Netherlands for each base station, the Dutch standard co-ordinates and the type of communication were involved (GSM900, GSM1800, UMTS). The GIS-EMV information system operated by the Laboratory of Radiation Research at the National Institute for Health and the Environment (RIVM) was used to determine the base stations close to a respondent's address. Both the distance of the address to the base station and an identification of the base station itself were added as an attribute to the respondents' addresses.
The data on the location of the power lines were derived from the same geographical information system. In a collaboration of RIVM and KEMA (a technical consultancy with expertise in the energy sector) the Dutch network of overhead power lines has been digitised in 2002 from topographic maps (1:25000) [32]. The overhead high-voltage power lines have five voltage levels ranging from: 50 kilovolts to 380 kilovolts (kV). The total length of overhead high-voltage power lines amounts to nearly 4000 km. These power line data were used to select the power line closest to a sample address and to determine the shortest (perpendicular) distance of the sample address to that power line. Both, the distance of the address to the power line and an identification of the power line itself were added as an attribute to the sample address. An overview of the position of the addresses, BS and powerlines is illustrated in Figure 1.
Figure 1.

Distribution over the Netherlands of the house addresses, mobile phone base stations and powerlines that were included in the study (clusters refer to groups of addresses).
Material
The Somatization scale of the Four-Dimensional Symptom Questionnaire (4DSQ or 4DKL) [33] was used to measure NSPS. It contains 16 items, with a score range of 0-32. Responses are based on the individual experience during the period of "last week", categorized as "no", "sometimes", "regularly", "often", "very often" and "constantly". They are scored as 0 for "no", 1 for "sometimes" and 2 for the rest response categories. The cut-off points divide the scores into "low" (0-10), "moderately high" (11-20) and "very high" (21-32). The scale measures a variety of physical symptoms that could be related to distress or psychopathologic conditions. A moderate score might indicate the presence of increased levels of distress, while higher scores can reflect psychological mechanisms that involve maladaptive health beliefs and focusing attention on symptoms. The scale is characterized by high internal consistency (Cronbach's a = 0.84).
To assess self-reported environmental sensitivity, a list of 9 items based on the Sydney Airport Survey [34] was used, representing perceived sensitivities to environmental stressors such as noise, light, specific materials, color, smells, temperature changes, cold or warm environment. The answers are formatted in a 5-point scale ranging from strongly disagree (0) to strongly agree (4). The reference period was "during the previous week". A higher score indicates a higher perceived sensitivity.
Perceived Proximity to BS and powerlines was evaluated with two positive statements; "I live in the vicinity of a mobile phone base station" and "I live in the vicinity of a powerline" ("vicinity" was defined as neighborhood). Answers were categorized as "yes" (1) and "no" (0) reflecting a high and low perception of proximity respectively.
Coping Styles were assessed using the subscales of Active problem-solving (5 items) and Avoidance (2 items) of the Utrecht Coping List (short version) [35]. The first subscale illustrates a direct and logical approach towards problematic situations and the second one describes the effort to avoid to deal with a stressful stimulus. All items are scored on a 4-point Likert scale (1 = Seldom or Never, 2 = Sometimes, 3 = Often, 4 = Very often). These two subscales have been demonstrated to be reliable in the general Dutch population, with Cronbach's a = 0.81 for the Active problem-solving scale and a = 0.67 for the Avoidance scale.
Lack of Perceived Control was identified using two items from a Dutch version of the Life Orientation Test (LOT) [36]: "I am always optimistic about my future" and "I hardly ever expect things to go my way". Furthermore, an extra item was added and combined, namely "If I try I can influence the quality of my living environment", in order to enhance the individual sense of control that can lead to a positive outcome. The score is rated on a 5-point Likert scale ranging from strongly disagree (0) to strongly agree (4). After proper reversals the included items were summed, with higher scores indicating less perceived control. Good validity has been demonstrated in Dutch population samples [36].
Finally, the questionnaire included questions on socio-demographic characteristics such as age, gender, ethnicity, education, occupational status, type of residence and home ownership status.
Statistical analysis
Variables representing distance measures were log-transformed in order to obtain normally distributed variables. Multilevel linear regression models were used to determine the effect of actual distance and perceived proximity to BS and powerlines, psychological components and demographic and home characteristics on the occurrence of NSPS which was included as a continuous score in the analysis. Taking into account the hierarchical nature of the data, a selection of levels of random effects was made in a model (random intercepts) describing the relation between the (log) actual distance to BS and NSPS. The selection used tests based on the Restricted Maximum Likelihood (REML). Once the levels for random effects were chosen they were included in all subsequent analyses for comparison reasons.
It is recommended for epidemiological studies to use a multilevel approach for confounding, since specific contextual characteristics such as SES may influence the associations between exposure and health [37]. In the current study each PC4 level contains a large but varying number of PC6 areas with a range 1 to 132 participants per code. Based on the results of the analysis of the random effects on NSPS it appeared that PC4 and PC6 were relevant to include in the multilevel analysis. Therefore, all models were adjusted for these random effects, plus SES (cross classification). Statistical significance of fixed effects was tested by comparing the goodness of fit of different models using a chi-square test of deviance. The estimation of effects on NSPS included five steps, which are presented as separate models.
In the primary analysis, the relationship between (log) actual distance to BS and NSPS was examined. A second linear mixed model tested the same relation while adjusting for demographic characteristics. In the following analysis (log) perceived proximity to BS and powerlines and (log) actual distance to powerlines were included. Next, the model was extended with variables related to home characteristics. In the final model, psychological variables were added to evaluate the relative contributions of coping styles, perceived control and self-reported environmental sensitivity.
In order to verify a possible moderating effect of psychological components on the relation between perceived proximity to BS and NSPS, the interaction term between each psychological component (avoidance, problem-solving, control, perceived sensitivity) and perceived proximity to BS were entered in the final model. This was based on the hierarchical moderated regression approach [38]. Descriptive statistics were produced using the Statistical Package for Social Sciences (SPSS), version 17. Linear mixed models and the moderated regression were conducted within the statistical software package R, version 2.10.0.
Results
Descriptive analyses and non-response
Table 1 presents the demographic structure and other key characteristics of the respondents. Descriptive analyses (using one-way ANOVA and t-test analyses) demonstrated a number of statistically significant differences in symptom report between different groups: Female participants had a higher score in NSPS t (3516) = -9.05, p = 0.00 compared to men.
Table 1.
General characteristics of the individuals included in the analysis
| Characteristic | Analytic sample (n = 3611) |
|---|---|
| Age in years (%) | |
| 18-24 | 208 (5.8) |
| 25-34 | 702 (19.4) |
| 35-44 | 799 (22.3) |
| 45-54 | 733 (20.5) |
| 55-64 | 586 (16.4) |
| 65 < | 550 (15.4) |
| Missing | 33 |
| Gender | |
| Male (%) | 1580 (44.1) |
| Female (%) | 2002 (55.9) |
| Missing | 29 |
| Ethnicity | |
| Native (%) | 2860 (79.7) |
| Non-native (%) | 730 (20.3) |
| Missing | 21 |
| Education* | |
| Lower (%) | 581 (16.6) |
| Middle (%) | 1292 (36.9) |
| Higher (%) | 1629 (46.5) |
| Missing | 109 |
| Occupational status | |
| > 20 hours per week (%) | 2045 (56.6) |
| < 20 hours per week (%) | 256 (7.1) |
| Unemployment/Retirement (%) | 635 (17.6) |
| Work incapacity (%) | 143 (4) |
| Students/Housewives | 532 (14.7) |
| Missing | 0 |
| Type of residency | |
| Separate (detached) house/Villa | 235 (6.8) |
| Semi-detached house | 900 (26) |
| Townhouse/Terraced house/Unit or flat with own Entrance | 1341 (38.7) |
| Unit or flat (with shared entrance or front door at walkway - covered/non-covered) | 988 (28.5) |
| Missing | 147 |
| Home ownership status | |
| Owned (%) | 2195 (61.2) |
| Rented (%) | 1391 (38.8) |
| Missing | 25 |
| Perceived proximity (subjects answering "yes") | |
| Base Stations (%) (total missing: 111) | 1197 (34.2) |
| Powerlines (%) (total missing: 103) | 523 (14.9) |
| Mean (SD) | |
| Actual distance to BS (in metres) | 347.3 (259.9) |
| Actual distance to powerlines (in metres) | 2381 (1508.5) |
| Non-specific physical symptoms | 6.1 (5.43) |
| Missing | 28 |
*Note: Higher: scientific education; Middle: professional education; Lower: lower than professional
Significant differences were found between different age groups F(5, 3548) = 7.52, p = 0.00; the highest scores were reported by the youngest (mean = 7.1, SD = 5.52) and the oldest category (mean = 6.31, SD = 5.47). Differences were also observed across the categories of educational level F (2, 3476) = 88.7, p = 0.00, with people of lower education reporting the highest symptom score (mean = 8.18, SD = 6.75). Symptom report also differed in terms of occupational status F (4, 3578) = 67.7, p = 0.00; the highest symptom score was reported by people unable to work (mean = 11.84, SD = 7.4) and unemployed individuals (mean = 7.04, SD = 5.9). Finally, non-native participants scored significantly higher in NSPS t(984) = -3.04, p = 0.002 than natives. Information about the prevalence of each of the 16 examined symptoms is provided in Figure 2. The associations between actual distance and perceived proximity for BS and powerlines are shown in Figures 3 and 4; the non-parametric Wilcoxon test yielded no significant results (p = 0.15 and p = 0.17 respectively).
Figure 2.
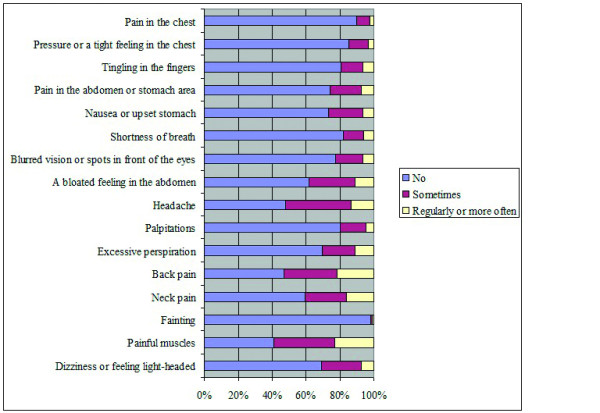
Frequencies (%) of the 16 self-reported symptoms in the sample.
Figure 3.

Box plot indicating the non-significant correlation between actual distance and perceived proximity to mobile phone base stations.
Figure 4.

Box plot indicating the non-significant correlation between actual distance and perceived proximity to powerlines.
A comparison of the 3611 respondents with 255 people (response rate 41%) who did not participate in the study, indicated small differences in demographic structure between the two groups: Participants were in general younger (mean age: 47 years) and had a higher level of education (46.5%) compared to non-participants (mean age: 50 years, higher education: 30%). In addition, participants were significantly less satisfied with their residential situation than the non-respondents (80% versus 90%, p < 0.05) and scored significantly lower on perceived health (68% versus 73%, p < 0.05). There were no differences in the male/female ratio. Based on these findings a moderate non-response bias might exist, which can be explained by the fact that part of the distribution is inherent to the study design and sampling process.
Multivariate analysis
Table 2 summarizes the results of the steps followed for the development of the full multilevel model.
Table 2.
Effects of actual distance and perceived proximity to BS and psychological components on NSPS
| Beta estimate (95% CI)* | ||||||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | ||
| Fixed effects | ||||||
| log Actual distance to BS | -0.02 (-0.35 - 0.34) | -0.004 (-0.33 - 0.32) | 0.14 (-0.19 - 0.45) | 0.28 (-0.05 - 0.6) | 0.25 (-0.037 - 0.57) | |
| Female Gender | 1.46 (1.05 - 1.87) ‡ | 1.48 (1.09 - 1.9) ‡ | 1.46 (1.04 - 1.85) ‡ | 0.97 (0.57 - 1.36) ‡ | ||
| Age | -0.04 (-0.20 - 0.12) | -0.07 (-0.25 - 0.08) | -0.10 (-0.27 - 0.06) | -0.06 (-0.22 - 0.09) | ||
| Education | -1.91 (-2.6 - -1.27) ‡ | -1.93 (-2.59 - -1.29) ‡ | -1.76 (-2.4 - -1.05) ‡ | -1.44 (-2.07 - -0.82) ‡ | ||
| Occupational status (Work Incapacity) | 4.54 (3.44 - 5.65) ‡ | 4.48 (3.39 - 5.6) ‡ | 4.33 (3.23 - 5.44) ‡ | 3.8 (2.72 - 4.9) ‡ | ||
| (< 20 hours/week) | -1.02 (-1.93 - -0.16) - | -1.05 (-1.97 - -0.20) - | -0.94 (-1.84 - -0.07) - | -1 (-1.85 - -0.17) - | ||
| (> 20 hours/week) | -0.69 (-1.3 - -0.09) - | -0.66 (-1.25 - -0.05) - | -0.56 (-1.16 - 0.06) | -0.27 (-0.90 - 0.27) | ||
| Students/housewives | 0.14 (-0.65 - 0.88) | 0.15 (-0.61 - 0.91) | -0.01 (-0.72 - 0.78) | 0.001 (-0.71 - 0.74) | ||
| Ethnicity | 0.29 (-0.22 - 0.79) | 0.31 (-0.20 - 0.82) | 0.32 (-0.17 - 0.83) | 0.36 (-0.14 - 0.83) | ||
| Perceived proximity to BS | 0.91 (0.24 - 1.58) + | 0.90 (0.23 - 1.58) + | 0.75 (0.08 - 1.37) - | |||
| Perceived proximity to powerlines | 0.99 (0.57 - 1.44) ‡ | 0.99 (0.54 - 1.42) ‡ | 0.87 (0.44 - 1.3) ‡ | |||
| log Actual distance to powerlines | 0.10 (-0.28 - 0.54) | -0.0002 (-0.39 - 0.42) | -0.05 (-0.40 - 0.25) | |||
| Home ownership status (Rented) | 1.16 (0.64 - 1.64) ‡ | 0.84 (0.35 - 1.33) + | ||||
| House type | 0.78 (-0.09 - 1.61) | 0.57 (-0.22 - 1.38) | ||||
| Perceived environmental sensitivity | 0.16 (0.13 - 0.19) ‡ | |||||
| Lack of Perceived control | 0.43 (0.32 - 0.54) ‡ | |||||
| Problem-solving | -0.05 (-0.12 - 0.02) | |||||
| Avoidance | 0.18 (0.09 - 0.28) ‡ | |||||
| Random effects (variances) | ||||||
| Postcode level | ||||||
| PC4 | 1.09 † ‡ | 1.12 | 0.36 | 0.35 | 0.31 | 0.11 |
| PC6 | 1.1 † - | 0.85 | 0 | 0.21 | 0 | 0 |
| Neighborhood level | ||||||
| SES | 1.35 † | 1.31 | 0.62 | 0.64 | 0.22 | 0.21 |
| Measurement level | ||||||
| Residual | 26.4 † | 26.4 | 25.1 | 24.4 | 24.5 | 22.3 |
*95% CI = 95% Confidence interval calculated by means of the standard error. - p <0.05. + p <0.01. ‡ p < 0.001. † Effects of random parameters on NSPS before adjusting for individual characteristic.
In the unadjusted model the effect of actual distance to BS was not significant (Model 1, Table 2). Results did not change after controlling for demographic characteristics. A significant effect was observed for gender, education and occupational status (Model 2).
In the next model (Model 3) the variables of actual distance and perceived proximity to powerlines were entered; although there was no relation between actual distance to powerlines and symptoms (estimate = 0.13, 95% CI -0.28 to 0.54), increased perceived proximity towards both BS and powerlines was associated with increase of symptom report. The fixed effect of actual distance to BS was increased but remained non-significant as in the previous equations.
When aspects related to the home environment were included, only the effect of renting a home was found to be significant (Model 4).
In the final model, the added contribution of psychological variables such as lack of perceived control, self-reported environmental sensitivity and the coping styles of problem-solving and avoidance was evaluated; a significant impact on NSPS was found for lack of perceived control and increased environmental sensitivity and avoidance, but not for problem-solving. Table 2 gives an overview of the final model estimates (Model 5).
In this fifth step, an analysis of interaction terms showed that there was a trend towards a moderator effect of perceived environmental sensitivity on the relation between perceived exposure to BS and NSPS (χ2 = 3.66, df = 1, p = 0.055). The other terms had no significant influence.
It is also noteworthy that after the inclusion of the fixed effects, the random effects of PC4 and PC6 were no longer significant. Dichotomization of actual distance to base stations (≤500 m., >500 m.) in line with the approach of Blettner et al. [5] did not change the results.
Discussion
The results of this study show that the actual distance to mobile phone base stations and powerlines did not predict non-specific physical symptoms, while socio-demographic and psychological factors have a significant effect on symptom report. Higher self-reported environmental sensitivity, perceived proximity to base stations and powerlines, lower perceived control, increased avoidance, living in a rented home, female gender, lower educational level and incapacity for work were significantly associated with increased NSPS report.
Comparing the symptom frequency in our sample with previous studies using the somatization scale of 4DSQ in the working population [39], we observed an average increase between 3%-6% (per symptom) for people reporting symptoms "regularly or more often" ("Fainting" was the only exception, reported almost in the same frequency). This increase can be explained if we take into account that in the current study more demographic categories are included (such as people being unemployed/retired or unable to work who are prone to symptom report). Therefore we consider these symptom rates as representative for the general population. This can be also supported by the fact that the mean symptom scores in the current sample (83% scored between 0 - 10, 14% 11 - 20 and 2.8% 21 - 32) were lower compared to general practice patients [40] and higher compared to the working population [40].
Previous cross-sectional studies investigating the link between actual distance to an EMF source and NSPS, showed inconclusive results due to methodological differences. A study solely based on female participants didn't detect any effect of distance from powerlines on the report of NSPS [41] while a recent epidemiological study determining actual distance from BS using geo-coding, demonstrated a statistically significant but very small impact of actual distance on NSPS [5]. A possible explanation could be that in our study the association between actual distance and symptoms was tested for a greater range of other possible determinants than in the earlier studies. In addition, in the current analyses we adjusted for area effects (PC4 and PC6) and SES levels. Still, the effect of actual distance in our study was increased considerably in the fourth model and almost reached borderline significance. This is unlikely to be caused by collinearity among the examined variables, since the Variance Inflation Factor (VIF) indicated a low possibility for multicollinearity. Nevertheless, an effect overestimation due to overadjustment for (similar) socio-demographic characteristics cannot be ruled out. It is notable that after adjustment for house characteristics, the effect of "full-time" employment (> 20 hours/week) was no more significant. Additionally, the unadjusted effect of actual distance to BS (measured per meter) on NSPS is negligible compared to the unadjusted effects of the other examined variables (data are not shown). The fact that we found strong determinants of NSPS in the analyses, especially in the last model, reduces the possibility of residual confounding. However, other potentially strong determinants of symptomatology such as obesity and smoking habits were not taken into account.
A main outcome was the significant effect yielded for perceived proximity to both BS and powerlines on NSPS, which was stronger for powerlines compared to BS. This might be partly explained by the visual aspects of powerlines. Even though previous findings have suggested a relation between NSPS and self-reported distance/proximity [42], the latter was not examined as a psychologically-oriented determinant but rather as a proxy of the actual exposure and there was a lack of proper confounding investigation.
Another important finding was the contribution of psychological characteristics to symptom report; increased perceived environmental sensitivity, lack of perceived control and an avoidant coping style were associated with elevated report of NSPS even after adjusting for actual distance and perceived proximity to BS and powerlines, demographic, home and area characteristics. The role of these psychological factors as determinants of NSPS related to EMF has to date not been extensively investigated in epidemiological studies therefore there are no previous results for comparison. However, there is some evidence that IEI-EMF samples tend to report also other sensitivities [2]. In addition, avoidance behavior has been suggested as a possible characteristic of sensitive to EMF people [6] and perceived control as a determinant of subjective pain experience [43]. No effect was observed in the current study for the problem oriented coping strategy, the improvement of which comprises an important element in psychological treatments of NSPS [44]. Possibly, this does not hold for environmental stressors which are typically outside the control of individuals [45].
This is the first study in which the possible relation between actual distance and perceived proximity to BS and powerlines, perceived environmental sensitivity, coping strategies, perceived control and NSPS was investigated in a relatively large population sample.
An important strength is the limited possibility of awareness bias, since the sample was not originally derived from subjects residing in varying vicinities of BS but was stratified based on areas with contrasting risk of environmental problems such as air and noise pollution and limited availability of green. Apart from the two questions on perceived proximity to BS and powerlines, the issue of EMF exposure was not addressed in the original study nor included in the questions regarding environmental sensitivities. The limited possibility for such bias could be also supported by the non-significant association between actual and perceived proximity for both BS and powerlines, although this association could be influenced by the definition used to describe "vicinity", which leaves some room for subjective interpretation.
Besides the cross-sectional nature of the present study, further limitations should be acknowledged. One weakness is related to the utilization of actual distance to BS as a proxy for exposure. Geo-coded distance might be a useful component in an EMF exposure prediction model but it is moderately correlated with residential exposure from fixed transmitters [46]; it is considered as a too simplistic proxy of the actual exposure level [46,47] which is a function of the square root of the Equivalent Isotropic Radiated Power divided by the distance. In a better approximation the power level and the antenna characteristics, e.g. the direction of the main beam of the transmitter, as well as the reflections and absorptions along the path from antenna to the home of the participant, as the housing parameters should be taken into account. Also the contribution of other EMF sources is of prior importance [46,47].
Another limitation of the study is the relatively low response rate which could increase the risk for non-response bias. Possible reasons could be the length of the study questionnaire and the small reward for participation. Non-response analysis however did not reveal large differences. Finally, at the time of this study only data on BS location as far back as June 2008 were available. Therefore the sample addresses in 2006 could only be compared with the base stations of 2008. This implies that for some addresses the closest base station did not exist yet or was not yet operable in 2006. More specifically, in June 2006 the total number of base stations (GSM900, GSM1800 and UMTS) amounted to 20.821; for June 2008 this number was 24.240 indicating an increase of 16% (data derived from the website of the Dutch 'Antennebureau', (http://www.antennebureau.nl/antenneregister) consulted on March 15 2011). We judged this 16% mismatch in the number of base stations as acceptable and had no means to reduce it. Thus, we realize that this mismatch resulted in an underestimation of the distance of the sampled addresses to the base stations.
Bearing these limitations in mind, this analysis has laid the ground for future studies into the effects of actual and perceived exposure to EMF by pinpointing the influence of individual and environmental factors when examining the link between environmental risks and health. The findings suggest that the report of NSPS in EMF studies should be approached as the outcome of a complex interaction between aspects such as actual exposure to environmental factors, the perception of being exposed and psychological factors.
Definition and outcome measurement issues are still under debate, such as the consideration of IEI-EMF as syndrome, disorder or set of symptoms, and its differentiation from somatoform disorders and NSPS. Under a common conceptual ground in terms of diagnostic criteria, future studies have to target on the reduction of recall and selection bias in EMF studies by the combination of the electronic medical records of general practitioners and self-reported health data, and the separate examination of actual and perceived exposure. Appropriate methods for rating symptoms as EMF-related are required, taking into consideration measurement determinants that have been proposed by the broader research field of medically unexplained symptoms such as population type, use of validated symptom checklists and frequency, severity and duration of the symptoms [48]. This should be accompanied with testing the significance of psychological variables that have been proposed as relevant to the report of NSPS while adjusting for psychiatric comorbidity.
The possible role of external influential factors such as media in the perception of risk and the magnification of related worries can additionally be a dimension of research on EMF and NSPS. It is also necessary to conduct more longitudinal and prospective research to address which variables constitute stable determinants of NSPS.
Conclusions
The present cross-sectional epidemiological study in the Netherlands is an exploration of potential determinants of symptom report related to distance to mobile phone base stations and powelines. It shows no relation between actual distance to these EMF sources and NSPS. Perceived environmental sensitivity, perceived proximity, lower perceived control, increased avoidance behavior and particular demographic characteristics and home aspects were significantly associated with increased symptom report. Further analyses showed a trend towards a moderator effect of perceived environmental sensitivity on the relation between perceived proximity to BS and NSPS. These components should be introduced in future epidemiological studies as potential moderating factors in order to comprehend the causal pathways that lead to the activation of somatic responses and subsequent symptoms.
List of abbreviations used
EMF: Electromagnetic Fields; BS: mobile phone Base Stations; NSPS: Non-Specific Physical Symptoms; IEI: Idiopathic Environmental Intolerance; IEI-EMF: Idiopathic Environmental Intolerance attributed to Electromagnetic Fields; SES: Level of Socio-economic Status; GSM - Global System for Mobile communications; UMTS: Universal Mobile Telecommunications System; PC4: 4-digit postcode level; PC6: 6-digit postcode level
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
All the authors participate in the multidisciplinary project EMPHASIS of the National Institute for Public Health and the Environment (RIVM). CB drafted the manuscript, performed part of the analyses and incorporated input from all the rest authors in the manuscript. IVK conceived and coordinated the study, performed part of the analyses and provided critical comments on the manuscript. GK conducted the computation of the distance between household addresses and location of base stations and powerlines. MS performed the main statistical analyses. JB, JY and EL provided critical comments on the manuscript. All authors have read and approved the final version of the manuscript.
Pre-publication history
The pre-publication history for this paper can be accessed here:
Contributor Information
Christos Baliatsas, Email: Christos.Baliatsas@rivm.nl.
Irene van Kamp, Email: irene.van.kamp@rivm.nl.
Gert Kelfkens, Email: Gert.Kelfkens@rivm.nl.
Maarten Schipper, Email: maarten.schipper@rivm.nl.
John Bolte, Email: John.Bolte@rivm.nl.
Joris Yzermans, Email: J.Yzermans@nivel.nl.
Erik Lebret, Email: erik.lebret@rivm.nl.
Acknowledgements
Data used in this study were based on a survey funded by the Dutch Ministry of Housing Spatial Planning and the Environment. The current study is part of the Dutch project EMPHASIS "Non-specific physical symptoms in relation to actual and perceived exposure to EMF and the underlying mechanisms", funded by The Netherlands Organisation for Health Research and Development (ZonMw). The study sponsor had no involvement in study design, collection, analysis, writing and interpretation of the data and in the decision to submit the study for publication. In addition, we would like to thank Dr Rik Bogers for his helpful comments over the paper.
References
- Petrie KJ, Sivertsen B, Hysing M, Broadbent E, Moss-Morris R, Eriksen HR, Ursin H. Thoroughly modern worries. The relationship of worries about modernity to reported symptoms, health and medical care utilization. Journal of Psychosomatic Research. 2001;51:395–401. doi: 10.1016/S0022-3999(01)00219-7. [DOI] [PubMed] [Google Scholar]
- Hillert L, Berglind N, Arnetz BB, Bellander T. Prevalence of self-reported hypersensitivity to electric or magnetic fields in a population-based questionnaire survey. Scandinavian Journal of Work, Environment and Health. 2002;28:33–41. doi: 10.5271/sjweh.644. [DOI] [PubMed] [Google Scholar]
- Schreier N, Huss A, Roosli M. The prevalence of symptoms attributed to electromagnetic field exposure: a cross-sectional representative survey in Switzerland. Sozial- und Praventivmedizin. 2006;51:202–209. doi: 10.1007/s00038-006-5061-2. [DOI] [PubMed] [Google Scholar]
- Schrottner J, Leitgeb N. Sensitivity to electricity - Temporal changes in Austria. BMC Public Health. 2008;8:310. doi: 10.1186/1471-2458-8-310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blettner M, Schlehofer B, Breckenkamp J, Kowall B, Schmiedel S, Reis U, Potthoff P, Schuz J, Berg-Beckhoff G. Mobile phone base stations and adverse health effects: phase 1 of a population-based, cross-sectional study in Germany. Occupational and Environmental Medicine. 2009;66:118–123. doi: 10.1136/oem.2007.037721. [DOI] [PubMed] [Google Scholar]
- Mild KH, Repacholi M, van Deventer E, Ravazzani P. Proceedings of the International Workshop on Electromagnetic Field Hypersensitivity. Prague, Czech Republic: World Health Organization; 2006. Electromagnetic Hypersensitivity. 25 - 27 October 2004. [Google Scholar]
- WHO. Fact Sheet No. 296: Electromagnetic fields and public health. World Health Organization; 2005. http://www.emfandhealth.com/WHO_EMSensitivity.pdf [Google Scholar]
- Levallois P, Neutra R, Lee G, Hristova L. Study of self-reported hypersensitivity to electromagnetic fields in California. Environmental Health Perspectives. 2002;110:619–623. doi: 10.1289/ehp.021100619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roosli M, Moser M, Baldinini Y, Meier M, Braun-Fahrlander C. Symptoms of ill health ascribed to electromagnetic field exposure - A questionnaire survey. International Journal of Hygiene and Environmental Health. 2004;207:141–150. doi: 10.1078/1438-4639-00269. [DOI] [PubMed] [Google Scholar]
- Carlsson F, Karlson B, Orbaek P, Osterberg K, Ostergren PO. Prevalence of annoyance attributed to electrical equipment and smells in a Swedish population, and relationship with subjective health and daily functioning. Public Health. 2005;119:568–577. doi: 10.1016/j.puhe.2004.07.011. [DOI] [PubMed] [Google Scholar]
- Schuz J, Petters C, Egle UT, Jansen B, Kimbel R, Letzel S, Nix W, Schmidt LG, Vollrath L. The "Mainzer EMF-Wachhund": results from a watchdog project on self-reported health complaints attributed to exposure to electromagnetic fields. Bioelectromagnetics. 2006;27:280–287. doi: 10.1002/bem.20212. [DOI] [PubMed] [Google Scholar]
- Hutter HP, Moshammer H, Wallner P, Kundi M. Subjective symptoms, sleeping problems, and cognitive performance in subjects living near mobile phone base stations. Occup Environ Med. 2006;63:307–13. doi: 10.1136/oem.2005.020784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thomas S, Kühnlein A, Heinrich S, Praml G, Nowak D, von Kries R, Radon K. Personal exposure to mobile phone frequencies and well-being in adults - across- sectional study based on dosimetry. Bioelectromagnetics. 2008;29:463–470. doi: 10.1002/bem.20414. [DOI] [PubMed] [Google Scholar]
- Berg-Beckhoff G, Blettner M, Kowall B, Breckenkamp J, Schlehofer B, Schmiedel S, Bornkessel C, Reis U, Potthoff P, Schüz J. Mobile phone base stations and adverse health effects: phase 2 of a cross-sectional study with measured radio frequency electromagnetic fields. Occup Environ Med. 2009;66:124–30. doi: 10.1136/oem.2008.039834. [DOI] [PubMed] [Google Scholar]
- Heinrich S, Kühnlein A, Thomas S, Praml G, von Kries R, Radon K. Association between exposure to radiofrequency electromagnetic field exposure and acute well-being in children and adolescents. Environmental Health. 2010;9:75. doi: 10.1186/1476-069X-9-75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heinrich S, Thomas S, Praml G, von Kries R, Radon K. The impact of exposure to radio frequency electromagnetic fields on chronic well-being in young people - a cross sectional study based on personal dosimetry. Environment International. 2011;37:26–30. doi: 10.1016/j.envint.2010.06.008. [DOI] [PubMed] [Google Scholar]
- Seitz H, Stinner D, Eikmann T, Herr C, Roosli M. Electromagnetic hypersensitivity (EHS) and subjective health complaints associated with electromagnetic fields of mobile phone communication--a literature review published between 2000 and 2004. Science of the Total Environment. 2005;34:45–55. doi: 10.1016/j.scitotenv.2005.05.009. [DOI] [PubMed] [Google Scholar]
- Roosli M. Radiofrequency electromagnetic field exposure and non-specific symptoms of ill health: a systematic review. Environmental Research. 2008;107:277–87. doi: 10.1016/j.envres.2008.02.003. [DOI] [PubMed] [Google Scholar]
- Rubin GJ, Nieto-Hernandez R, Wessely S. Idiopathic environmental intolerance attributed to electromagnetic fields (formerly 'electromagnetic hypersensitivity'): An updated systematic review of provocation studies. Bioelectromagnetics. 2009;31:1–11. doi: 10.1002/bem.20536. [DOI] [PubMed] [Google Scholar]
- Van Den Berg B, Grievink L, Yzermans J, Lebret E. Medically unexplained physical symptoms in the aftermath of disasters. Epidemiologic Reviews. 2005;27:92–106. doi: 10.1093/epirev/mxi001. [DOI] [PubMed] [Google Scholar]
- Van der Windt DAW M, Dunn ZM, Spies-Dorgelo MN, Mallen CD, Blankestein AH, Stalman WAB. Impact of physical symptoms on perceived health in the community. Journal of Psychosomatic Research. 2008;64:265–274. doi: 10.1016/j.jpsychores.2007.10.003. [DOI] [PubMed] [Google Scholar]
- Augner C, Hacker GW. Are people living next to mobile phone base stations more strained relationship of health concerns, self-estimated distance to base station, and psychological parameters. Indian Journal of Occupational and Environmental Medicine. 2009;13:141–145. doi: 10.4103/0019-5278.58918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Landgrebe M, Frick U, Hauser S, Langguth B, Rosner R, Hajak G, Eichhammer P. Cognitive and neurobiological alterations in electromagnetic hypersensitive patients: results of a case-control study. Psychological Medicine. 2008;38:1781–1791. doi: 10.1017/S0033291708003097. [DOI] [PubMed] [Google Scholar]
- Persson R, Carlsson EF, Osterberg K, Orbaek P, Karlson B. A two-week monitoring of self-reported arousal, worry and attribution among persons with annoyance attributed to electrical equipment and smells. Scandinavian Journal of Psychology. 2008;49:345–356. doi: 10.1111/j.1467-9450.2008.00660.x. [DOI] [PubMed] [Google Scholar]
- Rubin GJ, Cleare AJ, Wessely S. Psychological factors associated with self-reported sensitivity to mobile phones. Journal of Psychosomatic Research. 2008;64:1–9. doi: 10.1016/j.jpsychores.2007.05.006. [DOI] [PubMed] [Google Scholar]
- Osterberg K, Persson R, Karlson B, Carlsson EF, Orbaek P. Personality, mental distress, and subjective health complaints among persons with environmental annoyance. Human & Experimental Toxicology. 2007;26:231–241. doi: 10.1177/0960327107070575. [DOI] [PubMed] [Google Scholar]
- Johansson A, Nordin S, Heiden M, Sandstrom M. Symptoms, personality traits, and stress in people with mobile phone-related symptoms and electromagnetic hypersensitivity. Journal of Psychosomatic Research. 2010;68:37–45. doi: 10.1016/j.jpsychores.2009.06.009. [DOI] [PubMed] [Google Scholar]
- Rubin GJ, Das MJ, Wessely S. A systematic review of treatments for electromagnetic hypersensitivity. Psychotherapy & Psychosomatics. 2006;75:12–18. doi: 10.1159/000089222. [DOI] [PubMed] [Google Scholar]
- Henningsen P, Priebe S. New environmental illnesses: what are their characteristics? Psychotherapy & Psychosomatics. 2003;72:231–4. doi: 10.1159/000071893. [DOI] [PubMed] [Google Scholar]
- Taylor SE, Repetti RL, Seeman T. Health psychology: what is an unhealthy environment and how does it get under the skin? Annual Review of Psychology. 1997;48:411–47. doi: 10.1146/annurev.psych.48.1.411. [DOI] [PubMed] [Google Scholar]
- Spurgeon A. Models of unexplained symptoms associated with occupational and environmental exposures. Environmental Health Perspectives. 2002;110:601–5. doi: 10.1289/ehp.02110601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kelfkens G, Pennders RMJ, Pruppers MJM. Woningen bij bovengrondse hoogspanningslijnen in Nederland. Report commissioned by the Laboratory of Radiation Research. National Institute for Health and the Environment (RIVM), Bilthoven; 2002. [Google Scholar]
- Terluin B. De Vierdimensionale Klachtenlijst (4DKL). Een vragenlijst voor het meten van distress, depressie, angst en somatisatie. Huisarts Wet. 1996;39:538–47. [Google Scholar]
- Job RFS. Noise sensitivity as a factor influencing human reaction to noise. Noise and Health. 1999;1:57–68. [PubMed] [Google Scholar]
- Schreurs PJG, Van de Willige G, Brosschot JF, Tellegen B, Graus GMH. De Utrechtse Coping Lijst: UCL. Omgaan met problemen en gebeurtenissen [The Utrecht coping list, coping with problems and events] Lisse: Swets & Zeitlinger; 1993. [Google Scholar]
- Vinck J. Optimisme gemeten: validatie van de Nederlandstalige levensoriëntatietest bij jongeren. Gedrag en gezondheid. 1998;26:82–93. [Google Scholar]
- Chaix B, Leal C, Evans D. Neighborhood-level confounding in pidemiologic studies: unavoidable challenges, uncertain solutions. Epidemiology. 2010;21:124–7. doi: 10.1097/EDE.0b013e3181c04e70. [DOI] [PubMed] [Google Scholar]
- Cohen J, Cohen P. Applied multiple regression/correlation for the behavioural sciences. 2. Hillsdale, NJ: Erlbaum; 1983. [Google Scholar]
- Terluin B Van Rhenen W Schaufeli WB De Haan M The four-dimensional symptom questionnaire (4DSQ): measuring distress and other mental health problems in a working population Work & Stress 200418187–207. 10.1080/026783704200029753521638515 [DOI] [Google Scholar]
- Terluin B, Duijsens IJ. Handleiding van de Vierdimensionale Klachtenlijst. Leiderdorp: Datec; 2002. 4DKL-handleiding. [Google Scholar]
- McMahan S, Meyer J. Symptom prevalence and worry about high voltage transmission lines. Environmental Research. 1995;70:114–8. doi: 10.1006/enrs.1995.1055. [DOI] [PubMed] [Google Scholar]
- Santini R, Santini P, Danze JM, Le Ruz P, Seigne M. Symptoms experienced by people in vicinity of base stations: [Incidences of age, duration of exposure, location of subjects in relation to the antennas and other electromagnetic factors] Pathologie Biologie. 2003;51:412–415. doi: 10.1016/S0369-8114(03)00020-8. [DOI] [PubMed] [Google Scholar]
- Litt MD. Self-efficacy and perceived control: Cognitive mediators of pain tolerance. Journal of Personality and Social Psychology. 2010;54:149–160. doi: 10.1037//0022-3514.54.1.149. [DOI] [PubMed] [Google Scholar]
- Wilkinson P, Mynors-Wallis L. Problem-solving therapy in the treatment of unexplained physical symptoms in primary care: A preliminary study. Journal of Psychosomatic Research. 1994;38:591–598. doi: 10.1016/0022-3999(94)90056-6. [DOI] [PubMed] [Google Scholar]
- Campbell JM. Ambient Stressors. Environment and Behavior. 1984;15:355–380. [Google Scholar]
- Breckenkamp J, Neitzke HP, Bornkessel C, Berg-Beckhoff G. Applicability of an exposure model for the determination of emissions from mobile phone base stations. Radiation Protection Dosimetry. 2008;131:474–481. doi: 10.1093/rpd/ncn201. [DOI] [PubMed] [Google Scholar]
- Frei P, Mohler E, Bürgi A, Fröhlich J, Neubauer G, Braun-Fahrländer C, Röösli M. Classification of personal exposure to radio frequency electromagnetic fields (RF-EMF) for epidemiological research: Evaluation of different exposure assessment methods. Environment International. 2010;36:714–720. doi: 10.1016/j.envint.2010.05.005. [DOI] [PubMed] [Google Scholar]
- Kroenke K. Studying symptoms: Sampling and measurement issues. Ann Intern Med. 2001;134:844–853. doi: 10.7326/0003-4819-134-9_part_2-200105011-00008. [DOI] [PubMed] [Google Scholar]