

Abstract
BACKGROUND AND OBJECTIVES:
Brucellosis is considered the leading zoonotic disease of the Middle East. The disease has a wide spectrum of clinical manifestations and can result in complications with severe morbidity. The aim of this study was to evaluate the frequency, distribution and characteristics of arthritis in Iranian children with brucellosis.
DESIGN AND SETTING:
A retrospective descriptive study conducted in a referral children center in Tehran from 1997 to 2005.
PATIENTS AND METHODS:
Arthritis in children with brucellosis who were admitted to a specialized hospital was detected by clinical signs of the involved joint(s) and characteristics of joint fluid aspiration. Socio-demographic information was recorded.
RESULTS:
Of 96 patients diagnosed with brucellosis, 24 (25%) had Brucella arthritis 14 (58.3%) males and 10 (41.7%) females. Most common manifestations were fever in 21 patients (87.5%) and fatigue in 18 patients (75%). Monoarthritis was recorded in 15 patients (62.5%) of the cases with involvement of the knee in 8 (45%) and hip in 5 (29%), the ankle in 2 (8%) patients while 9 (37.5%) patients suffered from polyarthritis. None of the patients had axial joints involvement. Seventy-five percent of the subjects (18 patients) were from urban areas and 66.7% (16 patients) had consumed un-pasteurized cheese. Recurrence was not seen in any of the 24 patients who received a combination of co-trimoxazole for 6 weeks and gentamicin for 5 days.
CONCLUSION:
Childhood brucellosis is a challenging disease in Iran that has serious complications like arthritis. Therefore all physicians who work in endemic areas should be familiar with this disease and consider the possibility of brucellosis in all children who present with arthritis and arthralgia.
Brucellosis is a serious public health problem that brings about socioeconomic consequences in many countries. The disease is a typical zoonotic infection of domesticated and wild animals caused by organisms of genus Brucella. The infection occurs in humans by ingestion of animal milk or its products such as cheese, ice cream, butter, by direct contact with infected animals or inhalation of infectious aerosols.1,2
Mediterranean and Middle East countries such as Saudia Arabia, Syria and Iran are considered to have a very high rate of incidence despite control interventions.3,4 Brucellosis is considered the leading zoonotic disease of the region.5,6 In Iran the prevalence of brucellosis in animals reached 44% in 1956, but the first major control program that had started in 1958 resulted in a decrease to 5%. A second control program started in 1983 decreased the prevalence to 1.3% in 1987.7
According to health ministry data, human brucellosis is endemic in all parts of Iran. The number of patients with brucellosis was 71 051 in 1988 (132.4 per 100 000).3,6 Herd vaccination and animal eradication programs lead to a significant decrease (24 cases per 100 000) in 1998. In 2008, 17 905 cases (25 cases per 100 000) of brucellosis were identified. Several studies have showed that consumption of un-pasteurized milk, cheese and other milk products is the most common risk factor for brucellosis, while animal husbandry and veterinary professions are the less common factors.8–10
The disease has a wide spectrum of clinical manifestations and can affect a variety of organs and systems. Localized and complicated forms of brucellosis can cause severe morbidity and require prolonged medical treatment. As many as 25% to 80% of patients develop rheumatic problems with subsequent functional impairment.4,11 The diagnosis of brucellosis arthritis can be established by signs and symptoms of arthritis (pain, tenderness, swelling of the joint) in the presence of an antibody titer greater than 1:160 in the tube agglutination test or by a positive culture.12
The aim of the present study was to evaluate the frequency, distribution and characteristics of arthritis in 24 children with documented brucellosis arthritis.
PATIENTS AND METHODS
This study was approved by the Institutional Review Board and informed consent was obtained from all children's parents after explaining the purpose of the study. We reviewed hospital records of children with a confirmed diagnosis of brucellosis who were admitted to the infectious disease ward and pediatrics department between 1997 and 2005. Patients were admitted based on documented brucellosis. The cases with arthritis were selected for additional studies. Children with a history of trauma to the affected joints or a history suggesting other musculoskeletal diseases were excluded from this study. The patients with a history of tuberculosis or abnormal chest x-ray were also excluded.
Iran is an endemic area for brucellosis, therefore diagnosis of brucellosis was based on a standard tube agglutination titer (SAT)>1/160 and detection of 2-mercaptoethanol (2ME) brucella agglutination test in a titer of ≥1/40. Of the patients with confirmed diagnosis of brucellosis, the ones who had pain, swelling and loss of range of motion in their joints were selected for joint aspiration to confirm the diagnosis of brucellosis arthritis. The characteristics of the aspirated joint fluid for diagnosis of brucellosis arthritis was considered as positive Gram stain, markedly elevated leukocyte count and low glucose level. Bacterial cultures were performed in all patients. Patients were admitted 1-7 days after showing the signs of arthritis. All patients received oral co-trimoxazole 10 mg/kg (as trimethoprim) for 6 weeks and intramuscular gentamicin 5-7 mg/kg during first 5 days. Social and demographic information were recorded. The statistical analysis was performed with SPSS version 10. All cases were followed up to one year.
RESULTS
The 96 children in the study ranged in age from 2-12 years and 24 (14 boys and 10 girls) had arthritis. Mean (SD) age of patients was 7.4 years (3.71) (range, 25-144 months) (Table 1). There was a history of un-pasteurized cheese and milk consumption in 16 (66.7%) and 4 (16.7%) patients respectively. In 2 (8.4%) subjects there was a history of animal contact. In 7 cases there was another family member identified with brucellosis and in 2 cases two other family members had brucellosis.
Table 1.
Demographic data of the 96 children
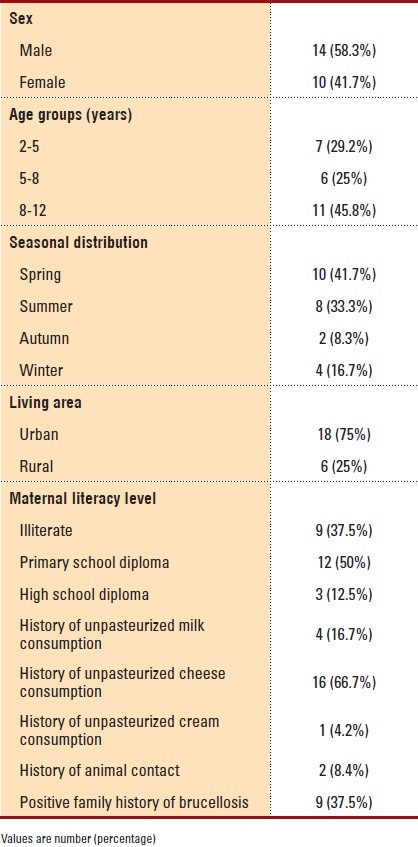
The most common presenting symptoms were fever in 21(87.5%), fatigue in 18 (75%), headache in 14 (58.3%), chills in 11 (45.8%), nocturnal diaphoresis in 10 (41.7%) and weight loss in 5 (20.8%) patients. Clinically-evident splenomegaly and hepatomegaly were found in 6 (25%) and 4 (16.7%) patients respectively. Fifteen cases (62.5%) demonstrated monoarthritis while 9 patients (37.5%) had polyarthritis. Knee, hip and ankle were the most common joints involved (Table 2). There was no record of axial joint involvement. Anemia in 4 (16.7%) and leukopenia in 3 (12.5%) patients were the most common laboratory findings. Thrombocytopenia was found in 2 (8.4%) patients. The erythrocyte sedimentation rate (ESR) value was elevated (≥20 mm/h) in 16 (66.7%) of cases and the C-reactive protein (CRP) value was elevated in 15 (62.5%). After treatment only 6 (25%) subjects had elevated ESR. The antibody titer to brucellosis determined by SAT and 2 ME are shown in (Table 3). All patients had normal blood and urine cultures. Brucella organisms were isolated in four patients from joint fluid; all positive cultures belonged to B melitensis. All patients showed a good response to the combination treatment and no recurrence was detected in any patient after one-year follow up.
Table 2.
Frequency of joint involvement in children with brucellosis
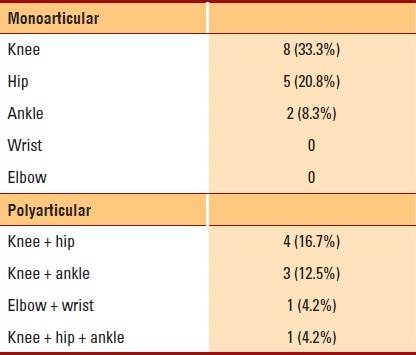
Table 3.
Wright and 2-ME titration before treatment

DISCUSSION
Despite all measures, brucellosis remains a challenging health problem in Iran. The disease could potentially harm children's health. The present study describes the clinical features of brucellosis arthritis, as a common manifestation of the disease in children. The most common age group with arthritis was 8 to 12 years old, which is similar to that reported by previous studies.2,13,14 About 16% of patients mentioned unpasteurized milk consumption, though a higher percentage (66.7%) of patients mentioned consumption of unpasteurized cheese. There was a history of animal contact in 2 cases. Other studies reported consumption of unpasteurized milk and contact with infected animals as the main routes of infection.4,13,15
In a study of 745 patients with brucellosis, Salari et al reported consumption of unpasteurized milk, cheese and other milk products as the main underlying factor.9 In a similar epidemiological study in the north of Iran, Roushan et al found that the consumption of fresh cheese, animal husbandry, working in a laboratory, and the veterinary profession, respectively, were the main risk factors for brucellosis infection.8 In the present study a majority of children were from urban areas and so animal contact was less common compared to similar studies. Milk products, especially cheese, are widely consumed in both rural and urban areas of the country as a traditional breakfast food. The high use of unpasteurized products by consumers proves that there is still not enough knowledge about the disease even in urban areas of the country. Spring and summer are the reproductive seasons of goats and sheep; therefore unpasteurized milk products are more available during these times as 41.7% and 33.3% of admissions occurred in spring and summer, respectively.
The most common manifestations were fever, fatigue, loss of appetite and arthralgia. The most common affected joints were the knee, hip and ankle, respectively. Arthritis of the upper extremities (wrist and elbow) was rare. These findings confirm results of other studies.13,14,16
Sacroiliitis and involvement of the spine were not observed in this study although these symptoms are reported as common in adults.16 The organism was isolated from the joint fluid in four patients. The type of Brucella in patients with positive bacterial culture was Brucella melitensis. No other species or organism was isolated. Brucella melitensis is reported to be the most common type of organism encountered in the region. It seems that Brucella melitensis is the most common type in Iran, but this needs to be clarified in a large national study.
ESR and CRP were positive in 66.7% and 62.5% of the cases, respectively. ESR values declined to normal ranges in 10 patients after treatment. In 6 patients the ESR value declined after treatment, but it did not return to a normal range. In most of the patients the sesrum agglutination test (SAT) was ≥1/320. SAT and 2ME titers decreased in all patients three weeks after completion of treatment. The combination of oral co-trimoxazole for 6 weeks and intravenous gentamicin for 5 days was used for all patients. Different types of treatment were used in other studies,2,4,17 but most used three drugs at least. For example combination of rifampin, doxycycline and co-trimoxazole2 or co-trimoxazole, streptomycin and rifampin was used for at least for 6 weeks.4 Although the population size was small, the combination of mentioned drugs is an effective treatment for childhood brucellosis. Following this treatment, the SAT titer decreased and clinical manifestations improved. No sign of recurrence was seen in any of the patients. A low recurrence rate (of about 3.5%) has been reported when the combination of rifampicin and doxycycline or cotrimoxazole were administered to children with brucellosis.17 Am high recurrence rate has been reported with short-term (3 weeks) two-drug regimens in children even when an aminoglycoside was included.18
In conclusion, all physicians who work in endemic areas should be familiar with this disease and should rule out brucellosis in all children presented with arthritis and arthralgia to prevent further complications. Treatment with co-trimoxazole for 6 weeks and gentamicin for 5 days seems to be effective for childhood brucellosis.
REFERENCES
- 1.Young E. Mandell, Douglas and Bennett's principles and practice of Infectious disease. Philadelphia: Churchill Livingston; 2000. Brucella species; pp. 2386–93. [Google Scholar]
- 2.Tsolia M, Drakonaki S, Messaritaki A, Farmakakis T, Kostaki M, Tsapra H, et al. Clinical features, complications and treatment outcome of childhood brucellosis in central Greece. J Infect. 2002;44:257–62. doi: 10.1053/jinf.2002.1000. [DOI] [PubMed] [Google Scholar]
- 3.Meslin FX. Zoonoses in the world: current and future trends. Schweiz Med Wochenschr. 1995;125:875–8. [PubMed] [Google Scholar]
- 4.Geyik MF, Gür A, Nas K, Cevik R, Sarac J, Dikici B, et al. Musculoskeletal involvement of brucellosis in different age groups: a study of 195 cases. Swiss Med Wkly. 2002;132:98–105. doi: 10.57187/smw.2002.09900. [DOI] [PubMed] [Google Scholar]
- 5.Abdou AE. Overview on the major bacterial zoonoses situation in the Mediterranean region. Inf. Cir. WHO MZCC. 1996:41. [Google Scholar]
- 6.Refai M. Incidence and control of brucellosis in the Near East region. Vet Microbiol. 2002;90:81–110. doi: 10.1016/s0378-1135(02)00248-1. [DOI] [PubMed] [Google Scholar]
- 7.Zowghi E, Ebadi A, Mohseni B. Isolation of Brucella organisms from the milk of seronegative cows. Rev Sci Tech. 1990;9:1175–8. doi: 10.20506/rst.9.4.525. [DOI] [PubMed] [Google Scholar]
- 8.Hasanjani Roushan MR, Mohrez M, Smailnejad Gangi SM, Soleimani Amiri MJ, Hajiahmadi M. Epidemiological features and clinical manifestations in 469 adult patients with brucellosis in Babol, Northern Iran. Epidemiol Infect. 2004;132:1109–14. doi: 10.1017/s0950268804002833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Salari MH, Khalili MB, Hassanpour GR. Selected epidemiological features of human brucellosis in Yazd, Islamic Republic of Iran: 1993-1998. East Mediterr Health J. 2003;9:1054–60. [PubMed] [Google Scholar]
- 10.Roushan MR, Ahmadi SA, Gangi SM, Janmohammadi N, Amiri MJ. Childhood brucellosis in Babol, Iran. Trop Doct. 2005;35:229–31. doi: 10.1258/004947505774938693. [DOI] [PubMed] [Google Scholar]
- 11.Colmenero JD, Reguera JM, Fernández-Nebro A, Cabrera-Franquelo F. Osteoarticular complications of brucellosis. Ann Rheum Dis. 1991;50:23–6. doi: 10.1136/ard.50.1.23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gotuzzo E, Alarcón GS, Bocanegra TS, Carrillo C, Guerra JC, Rolando I, et al. Articular involvement in human brucellosis: a retrospective analysis of 304 cases. Semin Arthritis Rheum. 1982;12:245–55. doi: 10.1016/0049-0172(82)90064-6. [DOI] [PubMed] [Google Scholar]
- 13.Lubani M, Sharda D, Helin I. Brucella arthritis in children. Infection. 1986;14:233–6. doi: 10.1007/BF01644269. [DOI] [PubMed] [Google Scholar]
- 14.Adam A, Macdonald A, MacKenzie IG. Monarticular brucellar arthritis in children. J Bone Joint Surg Br. 1967;49:652–7. [PubMed] [Google Scholar]
- 15.Shaalan MA, Memish ZA, Mahmoud SA, Alomari A, Khan MY, Almuneef M, et al. Brucellosis in children: clinical observations in 115 cases. Int J Infect Dis. 2002;6:182–6. doi: 10.1016/s1201-9712(02)90108-6. [DOI] [PubMed] [Google Scholar]
- 16.Benjamin B, Annobil SH. Childhood brucellosis in southwestern Saudi Arabia: a 5-year experience. J Trop Pediatr. 1992;38:167–72. doi: 10.1093/tropej/38.4.167. [DOI] [PubMed] [Google Scholar]
- 17.Khuri-Bulos NA, Daoud AH, Azab SM. Treatment of childhood brucellosis: results of a prospective trial on 113 children. Pediatr Infect Dis J. 1993;12:377–81. doi: 10.1097/00006454-199305000-00005. [DOI] [PubMed] [Google Scholar]
- 18.Abramson O, Abu-Rashid M, Gorodischer R, Yagupsky P. Failure of short antimicrobial treatments for human brucellosis. Antimicrob Agents Chemother. 1997;41:1621–2. doi: 10.1128/aac.41.7.1621. [DOI] [PMC free article] [PubMed] [Google Scholar]