

Abstract
Background & objectives
The congregation of a large number of people during Hajj seasons from different parts of the world in overcrowded conditions within a confined area for a long period of time presents many public health challenges and health risks. One of the main health problems of the crowding is ease transmission of pneumonia by air droplets. This study was aimed to determine the most common causes of bacterial pneumonia during the 2005 Hajj season and to relate the findings with clinical conditions.
Methods
A total of 141 patients with suspected pneumonia from the three main tertiary care hospitals in Makkah, Saudi Arabia, were investigated during Hajj season, 2005. Sputum and serum samples were collected and investigated for the possible presence of typical or atypical causative agents.
Results
Of the 141 clinically suspected pneumonia cases, 76 (53.9%) were confirmed positive by microbiological tests. More than 94 per cent of the confirmed cases were in the age group >50 yr, and 56.6 per cent of the cases were men. The most frequent isolates were Candida albicans (28.7%) and Pseudomonas aeruginosa (21.8%), followed by Legionella pneumophila (14.9%) and Klabsiella pneumoniae (9.2%). More than one causative pathogens were isolated in 15 patients (16.3%), and 55 per cent of patients were diabetic.
Interpretation & conclusions
Clinicians should be aware that typical pneumonia treatment regimens may not work well during the Hajj season due to the wide variety of isolated organisms. This necessitates taking a sputum sample before starting treatment for identification and sensitivity testing. Special precautions need to be taken for >50 yr old patients.
Keywords: Hajj, pneumonia, Candida, Pseudomonas
Hajj (the Muslim pilgrimage to Makkah) is one of the largest annual gatherings in the world and attracts more than 2 million pilgrims from almost every country. The Hajj takes place between the 8th and 13th day of the last month of the Islamic lunar calendar (355 days), and therefore, falls at different dates each year.
The gathering of so many people from different parts of the world in unavoidably overcrowded and confined areas for a short period of time presents many public health challenges. The combination of physical efforts, overcrowding and any pre-existing health conditions enhances the possibility of acquiring infectious diseases during the Hajj journey1.
Due to the heavy crowd, the distance between individuals remains less than one meter most of the time, and therefore, infectious diseases transmitted by droplet are very common during Hajj2. All of these diseases have domestic and international ramifications as Muslim pilgrims return home. In a prospective study in two tertiary hospitals during the Hajj season, Al-Ghamdi et al3 identified respiratory disease as the most common cause (57%) of admission to hospital with pneumonia being the leading reason for admission, affecting 39 per cent of all patients. A similar finding was obtained by Madani et al4 who found that infection with pneumonia was the most common cause of hospitalization (19.7%) during Hajj.
This cross-sectional study was performed to determine the most common causes of bacterial pneumonia during the 2005 Hajj season and to associate the findings with clinical conditions.
Material & Methods
This study protocol was approved by the Ethical Committee, Custodian of The two Holly Mosques Institute of Hajj Research, Umm Al-Qura University, Makkah- Saudi Arabia.
This was a cross-sectional study of pilgrim patients with suspected pneumonia who were admitted to Makkah hospitals at Makkah, Soudi Arabia, from the 1st to the 20th day of the Hajj month of the Islamic year 1426 (Jan 2005).
Three tertiary care hospitals [Hera General Hospital (284 beds), Al-Noor specialist Hospital (560 beds) and King Faisal Hospital (275 beds)] were included in this study. All those patients admitted with the clinical symptoms of pneumonia, including coughing with sputum, chills with shaking, fever, chest pain, shortness of breath and rapid breathing, were included. For those clinically suspected to have pneumonia, chest X-rays were performed and sputum specimens were collected and sent for laboratory examination. A history of diabetes was also reported during the study.
Microbiological analysis of sputum samples was performed in accordance to the standard microbiological methods5 to detect typical and atypical pneumonia causative agents. The tests include routine culture, acid fast bacilli examination, culture for Mycobacterium tuberculosis, and testing for IgM and/or IgG antibodies against Chlamydia pneumoniae, Mycoplasma pneumoniae and Legionella pneumophila (Vircell, S.L., Santa Fe, Granada, Spain).
Data entry and statistical analysis were performed using the Statistical Package for Social Science (SPSS) program (Release 15.0 Spss Inc., Chicago, II). Descriptive statistics, cross tabulations, χ2 tests, and t-tests were performed where appropriate. Statistical significance was set at P<0.05.
Results
Among the three hospitals included in this study, results showed that a total of 141 cases were identified as clinically suspected pneumonia. Of these, 76 cases were confirmed positive by microbiological tests, representing a frequency of 53.9 per cent. The distribution of positive cases was 28 (out of 46), 22 (out of 52) and 26 (out of 43) in Hera General Hospital, King Faisal Hospital and Al-Noor Specialist Hospital, respectively. The presence of classical symptoms of pneumonia such as cough and fever were present in 110 (78%) of the confirmed pneumonia cases. The data showed no significant association between the number of clinically suspected pneumonia cases among different hospitals and positive diagnosis. In terms of using a chest X-ray as a confirmatory method for the diagnosis of pneumonia cases, the study showed that an X-ray was positive in 122 (86.5%) of the total suspected cases. The association between X-ray results and positive microbiological tests was statistically significant (P<0.01).
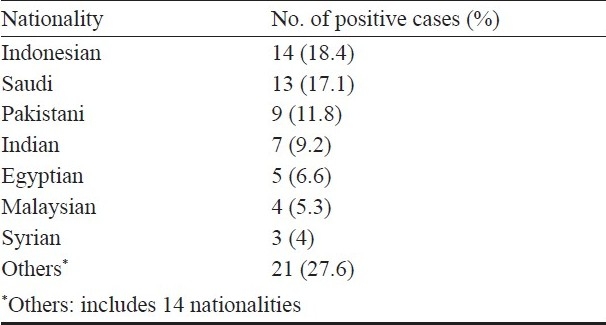
The demographic characteristics of pa-tients showed that the number of pneumonia cases in males (43, 56.6%) was slightly higher compared to female cases (33, 43.4%). In terms of age, the data showed that more than 94 per cent of the cases were in the >50 yr age group (Fig.). Most cases were reported in Indonesian nationals (18.4%) followed by Saudi (17.1%) and Pakistani (11.8%) nationals (Table I).
Fig.
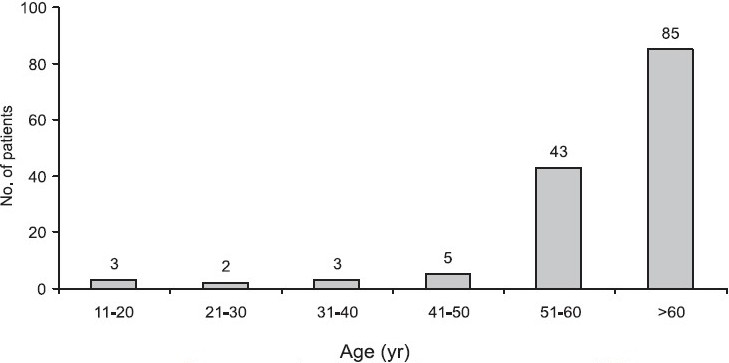
Frequency of suspected pneumonia cases among different age groups.
Table I.
Distribution of pneumonia cases among different nationalities
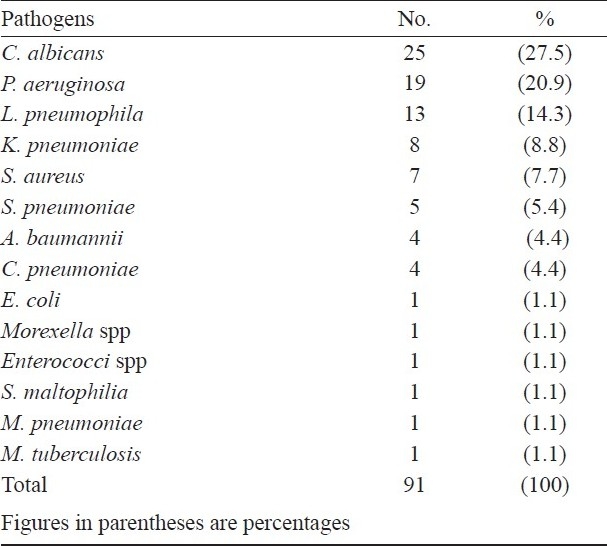
The study showed that the majority of pneumonia cases were caused by C. albicans (27.5%) and P. aeruginosa (20.9%), followed by L. pneumophila (14.3%) and K. pneumoniae (8.8%) (Table II). Interestingly, more than one causative pathogen was isolated in 15 patients (16.3%), and 55 per cent of cases were diabetic.
Table II.
Frequency of isolated pathogens among pneumonia cases
Discussion
Acute respiratory tract infection, particularly pneumonia, is the leading infectious disease acquired during Hajj representing 39 per cent among various diseases acquired during Hajj4. This study was carried out to determine the extent of pneumonia admitted in the three main hospitals in Makkah during Hajj season, 2005.
The study showed the total percentage of positive cases as 53.9 per cent. The large gap between the number of suspected cases and positives could be due to several factors, including the clinical misdiagnosis of cases, pre antibiotic usage, and inadequate sputum collection technique.
A previous study in 200 suspected pneumonia cases concluded that direct laboratory examination of sputum and leukocyte count should be performed routinely in patients with suspected pneumonia since leukocyte (>25) and epithelial (<10) counts in sputum samples per low-power field appear to be the most important criterion for predicting a positive culture6.
The study showed that a significant association existed between chest X-ray results and positive microbiological tests. This technique could be used as a quick diagnostic method to detect pneumonia cases during Hajj, as has been suggested previously, especially if combined with other clinical symptoms such as cough and fever7.
In terms of gender, the study revealed that there is no sex predominance among pneumonia cases; this is in contrast to many studies that showed the pneumonia infection are more frequent in males8. A similar finding to our results was found by Madani et al4during the Hajj season, 2003. This could be due to the fact that both genders are subjected to the same environment and physical activities during the Hajj journey. Regarding age, the data showed that more than 94 per cent of the cases were in the >50 yr old age group. In general, elderly pilgrims are susceptible to infections due to exertion, lack of sleep, disturbance in dietary schedule, etc., and developing serious medical complications due to decreased immune function2,4,8,9.
Our results showed that pneumonia cases were more predominant among Indonesian pilgrims. This finding could be explained by taking into account the higher number of Indonesian pilgrims performing Hajj compared to other nationalities.
The study showed that the majority of pneumonia cases were caused by C. albicans and P. aeruginosa followed by L. pneumophila and K. pneumoniae. The etiological agents of pneumonia in Hajj have not been extensively studied before. Alzeer et al9 studied 64 selected patients with pneumonia during the 1994 Hajj season who failed the first line of therapy and required hospital admission. The diagnosis of pneumonia was confirmed in 46 (72%) patients; M. tuberculosis (13/46, 28%) and Gram-negative organisms (12/46, 26%) were the most common causative organisms, accounting for over half of the culture-confirmed cases. S. pneumoniae was identified in 6 (10%) patients, and atypical organisms were identified in only 4 (6%) patients. They concluded that the aetiological agents of pneumonia in Hajj are different from those of community-acquired pneumonia9. In another study, El-Sheikh et al10, obtained 395 sputum samples during the 1998 Hajj season from patients presenting with symptoms of pneumonia. They recorded H. influenzae, K. pneumoniae, and Streptococcus pneumoniae as the most common pathogens. A few local studies conducted during the pilgrimage period highlighted that pneumonia was one of the most frequent morbidities among hajjees11,12.
The finding that more than half of the confirmed pneumonia cases were diabetic should be carefully considered in treatment planning, since it has been confirmed that diabetes mellitus is associated with a poor prognosis, by increasing the rate of pleural effusion and mortality13–16.
In conclusion, this study provided information on the most common causes for pneumonia, and the demographic distribution of the disease. These data will be of help to health care planners, administrators, and officials in order to provide optimal health care services to pilgrims in Hajj. Clinicians should be aware that typical pneumonia treatment regimens may not work well during the Hajj season due to the wide variety of isolated organisms. This necessitates taking a sputum sample before starting treatment for identification and sensitivity testing, since a single dose of antibiotic treatment prior to pneumonia diagnosis may hinder the detection of the causative agent13. As most of the patients were above 50 yr old, special precautions could be taken with this age group, including immunization, avoiding crowds and using facial masks to reduce the chance of infection.
Acknowledgments
The authors acknowledge The Custodian of the Two Holy Mosques Institute of Hajj Research for financial support, and thank the hospitals participated in this study for their co-operation and support.
References
- 1.Alzeer AH. Respiratory tract infection during Hajj. Ann Thorac Med. 2009;4:50–3. doi: 10.4103/1817-1737.49412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ahmed QA, Arabi YM, Memish ZA. Health risks at the Hajj. Lancet. 2006;25; 367:1008–15. doi: 10.1016/S0140-6736(06)68429-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Al-Ghamdi SM, Akbar HO, Qari YA, Fathaldin OA, Al-Rashed RS. Pattern of admission to hospitals during muslim pilgrimage (Hajj) Saudi Med J. 2003;24:1073–6. [PubMed] [Google Scholar]
- 4.Madani TA, Ghabrah TM, Al-Hedaithy MA, Alhazmi MA, Alazraqi TA, Albarrak AM, et al. Causes of hospitalization of pilgrims in the Hajj season of the Islamic year 1423 (2003) Ann Saudi Med. 2006;26:346–51. doi: 10.5144/0256-4947.2006.346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Murray PR, Baron EJ, Jorgensen JH, Landry ML, Pfaller MA, editors. Manual of clinical microbiology. 9th ed. Washington DC: American Society for Microbiology Press; 2007. [Google Scholar]
- 6.Roche N, Kouassi B, Rabbat A, Mounedji A, Lorut C, Huchon G. Yield of sputum microbiological examination in patients hospitalized for exacerbations of chronic obstructive pulmonary disease with purulent sputum. Respiration. 2007;74:19–25. doi: 10.1159/000093158. [DOI] [PubMed] [Google Scholar]
- 7.Fein A, Grossman R, Ost D, Talwar A, Merwin S. Diagnosis and management of pneumonia and other respiratory infections. 2nd ed. Washington DC: Professional Communications; 2006. [Google Scholar]
- 8.Combes A, Luyt CE, Trouillet JL, Nieszkowska A, Chastre J. Gender impact on the outcomes of critically ill patients with nosocomial infections. Crit Care Med. 2009;37:2506–11. doi: 10.1097/CCM.0b013e3181a569df. [DOI] [PubMed] [Google Scholar]
- 9.Alzeer A, Mashlah A, Fakim N, Al-Sugair N, Al-Hedaithy M, Al-Majed S, et al. Tuberculosis is the commonest cause of pneumonia requiring hospitalization during Hajj (pilgrimage to Makkah) J Infect. 1998;36:303–6. doi: 10.1016/s0163-4453(98)94315-8. [DOI] [PubMed] [Google Scholar]
- 10.El-Sheikh SM, El-Assouli SM, Mohammed KA, Albar M. Bacteria and viruses that cause respiratory tract infections during the pilgrimage (Haj) season in Makkah, Saudi Arabia. Trop Med Int Health. 1998;3:205–9. [PubMed] [Google Scholar]
- 11.Asghar AH. Frequency and antimicrobial susceptibility patterns of bacterial pathogens isolated from septicemic patients in Makkah hospitals. Saudi Med J. 2006;27:361–7. [PubMed] [Google Scholar]
- 12.Baharoon S, Al-Jahdali H, Al Hashmi J, Memish ZA, Ahmed QA. Severe sepsis and septic shock at the Hajj: etiologies and outcomes. Travel Med Infect Dis. 2009;7:247–52. doi: 10.1016/j.tmaid.2008.09.002. [DOI] [PubMed] [Google Scholar]
- 13.Falguera M, Pifarre R, Martin A, Sheikh A, Moreno A. Etiology and outcome of community-acquired pneumonia in patients with diabetes mellitus. Chest. 2005;128:3233–9. doi: 10.1378/chest.128.5.3233. [DOI] [PubMed] [Google Scholar]
- 14.Valdez R, Narayan K, Geiss L, Engelgau M. Impact of diabetes mellitus on mortality associated with pneumonia and influenza among non-Hispanic black and white US adults. Am J Public Health. 1999;89:1715–21. doi: 10.2105/ajph.89.11.1715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ruiz-Gonzalez A, Falguera M, Nogues A, Rubio-Caballero M. Is Streptococcus pneumoniae the leading cause of pneumonia of unknown etiology? A microbiologic study of lung aspirates in consecutive patients with community-acquired pneumonia. Am J Med. 1999;106:385–90. doi: 10.1016/s0002-9343(99)00050-9. [DOI] [PubMed] [Google Scholar]
- 16.Baomer AA, el bushra HE. Profile of diabetic Omani pilgrims to Mecca. East Afr Med J. 1998;75:211–4. [PubMed] [Google Scholar]