

Abstract
Labeled dentures can be important in identifying the owners in case of an accident, loss of memory, states of unconsciousness, being inadvertently misplaced on admission to a hospital or, in identifying the bodies of those who have died in a calamity. Positive identification through labeled dentures plays a key role in forensic scenario. Marking dentures has been considered as an important part of forensic dentistry, although no standardized method is followed. A number of labeling systems are available and can be broadly separated into either surface marking methods or inclusion systems. Each of the commonly described techniques is assessed with respect to their strengths and weaknesses. The more contemporary methods, though hi-tech, are expensive and may not be suitable for all dental practitioners to use. This article reviews the strengths and weaknesses of various methods involved in labeling dentures concluding by recommending that this valuable topic be included in the dental curriculum in India.
Keywords: Dentures, inclusion methods, labeling, surface methods
Introduction
Labeling of all dentures is recommended by most international dental associations and forensic odontologists. In fact, in some countries and certain states of the USA, the labeling of dentures is regulated by legislation.[1] As part of the obligation of the profession, a dental practitioner needs to maintain meticulous dental records of his patients. This would include documenting the identity of dentures.
Identification of dentures provides vital clues in recognizing the denture-wearer and takes vital significance especially in a forensic scenario effectively bringing closure to the case. Alternately, should an edentulous individual be involved in a disfiguring catastrophe, it becomes easier to identify the person if his dentures were uniquely coded or marked. Positive identification of the denture is usually done with a tiny, discreet identification code which is embedded in the denture base.
The American Board of Forensic Odontology guidelines indicate that most dental identifications are based on restorations, caries, missing teeth and/or prosthetic devices.[2] The purpose of denture marking thereby not only assists in the return of a lost denture, but also it facilitates the identification of edentulous persons who are either living or deceased.
The standard requirements for denture markers are that they should be biologically inert when incorporated into the denture, inexpensive, easy and quick to apply, possible to retrieve after an accident, acid resistant and survive elevated temperatures.[3] The marking must also be esthetically acceptable, visible (readable) and durable without jeopardizing the strength of the prosthesis. In addition, the marking should be permanent and resistant to everyday cleansing and disinfecting agents. The recommended areas for marking therefore are the posterior regions of the lingual flange and the palate.[4]
In countries where unique identification numbers are given to each individual, dentures may be marked with that number to enable positive identification. Over the years, various methods of denture marking have been reported in the literature. However, there are two main methods in marking dentures, namely the surface method and the inclusion method.[5]
Surface methods
In the surface marking method, the marks are located on one of the denture's surface and can be done by “scribing or engraving” the denture itself.[5] In this technique, letters, or numbers are engraved with a small round dental bur on the fitting surface of the maxillary complete denture [Figure 1]. This engraving can cause detrimental effects such as food debris getting lodged leading to bacterial infection.[6]
Figure 1.
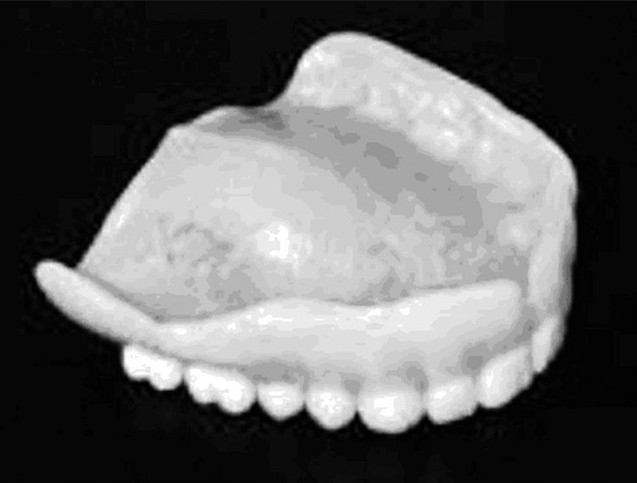
Initials of the patient engraved on the denture (tissue surface)
Another surface marking technique, “embossing”, comprises initials of the name and the surname of the patient that are scratched with a dental bur on the master cast.[5] This technique produces embossed lettering on the fitting surface of the denture [Figure 2a] and has been associated with malignancy, possibly due to continued tissue irritation, and may not be an ideal method for denture marking.[7] A better way is to cover the embossed marking on the denture framework with the denture base acrylic and process it to finished state so that it causes no irritation to the tissue [Figure 2b–d].
Figure 2.
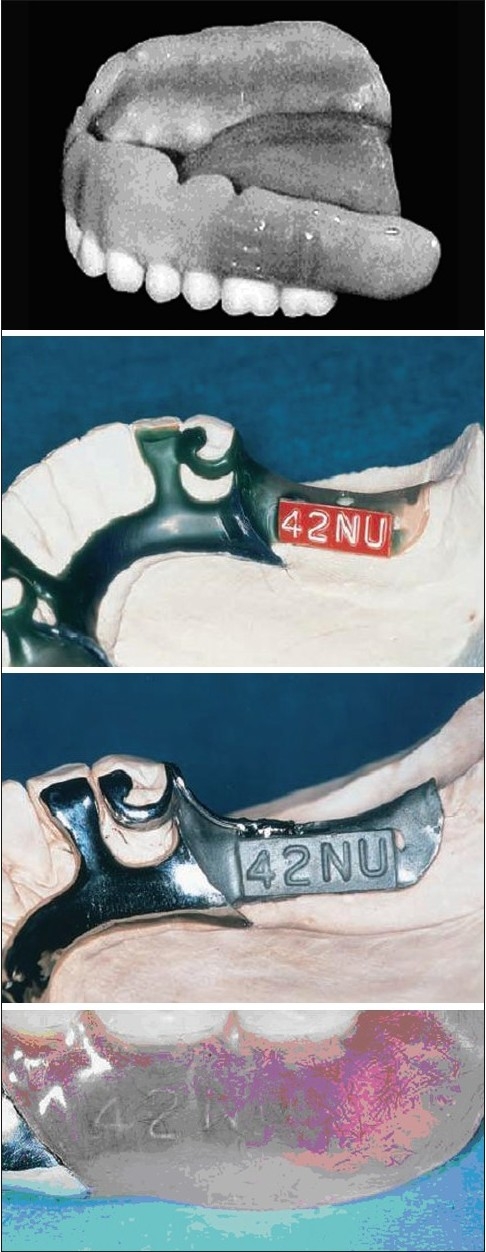
(a)Embossed initials of a patient on the buccal surface of the denture; (b) Embossed plastic tape applied to wax pattern; (c) Cast framework with marking; Marked framework visible through the processed denture
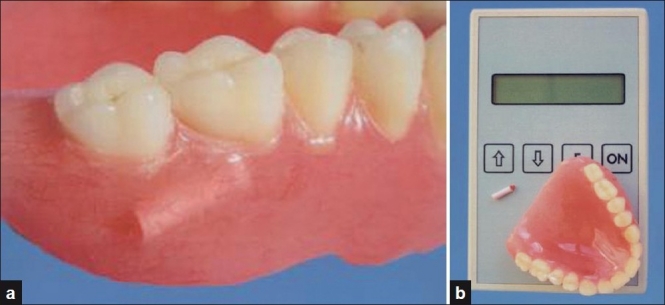
Writing on the tissue-fitting surface or the polished surface of the finished denture surface with a fibre-tip pen is another type of surface marking [Figure 3].[5] The patient's identification details are then covered by at least 2 thin coats of varnish which prolong the life of the marking. The varnish used is made by dissolving 5 g of acrylic resin polymer in 20 ml of chloroform and is inexpensive and unaffected by denture cleaners, antiseptics and mouthwashes.
Figure 3.

Identification marking on the tissue surface of a maxillary denture
Inclusion methods
The inclusion methods are more permanent as opposed to the relatively simple surface marking methods; however, these techniques require certain skills and are time consuming. The marks are made by using metallic or non-metallic materials, microchips and micro labels which are enclosed in the denture at the packing stage. Sometimes, a dislocation, wrinkling or tear can occur proving to be a disadvantage as an identification method.[5]
ID-Band
Dentures may be marked with a stainless steel metal band. The most commonly used fire- resistant materials are titanium foil and Ho Matrix Band containing an identifiable coding system representing patient details.[5] A shallow recess for the metal band is prepared in the denture base in the desired location, to a length 6 mm longer than the identification band. The preparation is 3 mm deeper than the thickness of the metal band. A small amount of clear acrylic resin is placed on the bottom of the prepared recess over which a metal band is placed and examined for proper fit. The band is covered with clear acrylic resin, trimmed and finished in the usual manner [Figure 4]. Stainless steel has a good biocompatibility and high corrosion resistance in oral environment and does not cause any allergies.[8]
Figure 4.
Metallic band embedded in a lower denture
The Swedish ID-Band has now become the international standard among ID bands.[9] It is resistant to very high temperatures, up to 1100°C, is inexpensive, quick requiring no special equipment or training, legible, radiopaque and cosmetically appealing,[3] although, a metal insert will inevitably cause weakening of the denture at that point creating a plane of cleavage.[10]
Paper strips
This method is a less expensive alternative utilizing a piece of “onion skin” paper. The acrylic resin fitting surface situated adjacent palatally between the ridge and the center of the palate is moistened with monomer on a small brush. The strip of typed paper is laid on this surface and the paper is moistened with the monomer. Clear or pink polymethyl methacrylate (PMMA) is then placed over the paper before final closure of the denture flask.[14] The Vestermarks method uses pink paper and red inscription[12] and the paper strip may not survive a fire.[5]
T-Bar
A T-shaped clear PMMA resin bar is constructed by cutting baseplate wax and then is flasked, packed, processed, and finished in clear PMMA. An identification printed label (reduced in size, print-face inward) against the flat section of the bar is fixed. It is then surface polished to produce a clear window displaying the ID label.[13] This procedure is easy, inexpensive and time-effective.
Laser etching
Specially equipped laboratories can provide a copper vapor laser (CVL) that can etch a patient's identification into the metal surface of a partial denture.[13] A CVL can label the cobalt-chromium components of dentures easily, legibly and reduce the font size of the data. The CVL beam is focused and delivered to the material surface by the two-axis scanner mounted with mirrors. A personal computer controls the movement of the scanner and the firing of the CVL. However, this method is not only expensive but also requires specialized equipment and technicians to perform the procedure.
Electron microchips
With the value of denture markings gaining better understanding, high end technology was tried to label dentures. The patient's information was etched onto a chip measuring 5×5×0.6 mm. Tests conducted on chips embedded in acrylic resin performed well under high temperatures (600°C), had excellent acid resistance, was radio-opaque and bonded well with acrylic resin. However, the main disadvantage of the chip was that it could be inscribed only by the manufacturer and not by the dentist.[11] Further attempts included refining this method with additional equipment to transfer details to a computer.
RFID –tags
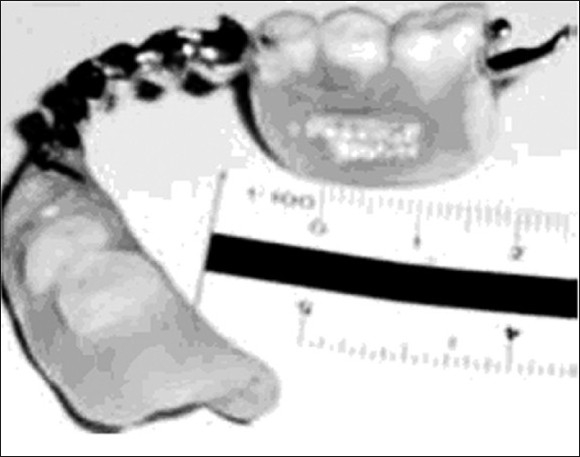
The inclusion of radio-frequency identification (RFID)-tags within dentures is a cosmetic, effective labeling method permitting rapid and reliable identification of the wearer.[11] They are preferred because of their small size (8.5×2.2 mm) and the large amount of denture user data that can be stored in them [Figure 5a]. Their RFID system consisted of a data carrier, or tag, and an electronic handheld reader that energizes the transponder by means of an electromagnetic field emitted via the reader's antenna [Figure 5b]. It then receives the coded signal returned by the transponder and converts it into readable data.[11] No special training is required to set the tag in the denture. The chip is resistant to disinfectants and solutions of 1% hypochlorite, 4% chlorhexidine, and 4% sodium perborate.
Figure 5.
(a) Polished denture with tag incorporated; (b) RFID-Tag, hand held reader and maxillary denture
Because of tag's size, there is no real weakening of the denture as would be expected with metallic markers. In case of laboratory reline or rebase of the denture, there is no need to remove the device before finishing the procedure. The chip remains intact and readable in sub-zero temperature[15] as well as after burning for 1 hr at 1500°C.[16] Unfortunately, RFIDs are not widely used due to the high cost of manufacture and data incorporation and may not be available in most dental set-ups.[17]
Lenticular system
Lenticular printing is a simple, cheap and quick method in which a lenticular lens is used to produce images with an illusion of depth, morph, or the ability to change or move as the image is viewed from different angles.[18] Lenticular technology allows images to be printed on the back of a synthetic paper and laminated on the lens. The lenticular card shows no signs of degradation when placed in water for up to a four-month period. It does not require special glass or device to read the data, like computer or hand-held reader and does not interfere with the oral function because of its small size. The possible disadvantages of this technique are that information can never be changed, and may not withstand a fire, unless the strip is placed in the most posterior part of the denture.
Denture barcoding
A bar code applicable to dentures consists of a machine-readable code of a series of bars and spaces printed in defined ratios.[19] A tedious technique described denture bar coding to printing a number code on paper, photographing the paper, making and transferring the negative to a piece of silk. An image of the bar code appeared on a prepared faience, by a machine that forced the paint through the silk, when heated to 860°C for 30 min in an industrial porcelain oven. The barcode was then read with a reader, and incorporated on to the denture, sealed with acrylic resin [Figure 6] and could be used for crowns also.[20] Denture barcoding provides exact information, and is resistant to high temperatures and commonly used oral solutions. However, it requires expensive special equipments.
Figure 6.

Barcode strip placed with in the processed maxillary denture
Photograph
A new denture marker has been suggested which makes use of the patient's photograph embedded in clear acrylic denture base.[21] The marker is particularly useful in the countries with low literacy rate where a photograph is the easiest method of identification. However, thermal tests revealed that the photographic marker and bar code were only resistant to around 200–300°C.
Discussion
Among the techniques surveyed, the surface method seemed easy to apply and relatively inexpensive, but they worn off very easily and needed to be reapplied. The inclusion methods were definitely more permanent and provided a positive result, but it tended to weaken the denture structure and create porosity. It was also found to be more expensive and trained personnel in well-equipped dental laboratories were needed, if any of the inclusion methods were to be chosen.
Several situations demand that the individual be identified. It is obvious that only marked dentures can reveal the positive identity of a person when all other methods fail to do so. This itself is the reason enough to justify the implementation of ID-marking of dentures.[22] The dentist should always inform the patient clearly the benefits of denture labeling and motivate the patient for the same. However, the patient has a right to refuse. Some of the procedures for dental labeling may be too expensive for the patient.[23] In the United Kingdom, the National Health Service provides a fee to the dentist to label patients who are in “care” homes.[24] In the USA, denture marking is mandatory in 21 states only, and the social security number of the individual is marked. In Australia, the tax file numbers are used, whereas in Sweden, the unique personal identity of the person is labeled.[25] In India, denture marking is neither taught nor is it practiced in any dental college on routine basis.
Recommendations
Considering the social and practical value of denture marking, there is an urgent need for marking dentures by members of the dental team involved in the provision of dentures to the public. The following recommendations to achieve this are offered:
Education at undergraduate level is urgently needed regarding the social and forensic value of marking dentures.
The practice of denture marking in all teaching institutions should be initiated immediately.
Further research should be carried out into improving and simplifying methods of labeling dentures.
Dental associations should find more effective ways of promoting the practice of denture labeling within the dental profession and the community.
Conclusions
The major reasons for not marking dentures are cost, lack of awareness of the various methods and a belief that it is of little importance. Needless to say, that the value of labeling dentures is immense when a positive identity of an individual is required. This has been stressed by forensic odontologists worldwide. Hence, an appropriate framework within dental education is required to ensure that both student dentists and student dental technologists are exposed to denture marking methodologies. There is a need to offer patients an esthetically suitable denture marking system that is also inexpensive and permanent.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Alexander PM, Taylor JA, Szuster FS, Brown KA. An assessment of attitudes to, and extent of, the practice of denture marking in South Australia. Aust Dent J. 1998;43:337–41. doi: 10.1111/j.1834-7819.1998.tb00185.x. [DOI] [PubMed] [Google Scholar]
- 2.The ABFO Identification Guidelines. Home page 2006. [last accessed on 2010 Sep 14]. Available from: http://www.forensicdentistryonline.org/Forensic_pages_1/ident_guidelines.htm .
- 3.Borrman HI, DiZinno JA, Wasén J, René N. On denture marking. J Forensic Odontostomatol. 1999;17:20–6. [PubMed] [Google Scholar]
- 4.Wilson HJ, Mansfield MA, Heath JR, Spence D. 8th ed. London: Blackwell Scientific Publications; 1987. Dental technology and materials for students; pp. 397–401. [Google Scholar]
- 5.Stavrianos CH, Petalotis N, Metska M, Stavrianou I, Papadopoulos CH. The value of identification marking on dentures. Balk J Stom. 2007;11:212–6. [Google Scholar]
- 6.Seals RR, Jr, Dianna JS. Hospital dentistry: The importance of denture identification. Spec Care Dentist. 1985;5:164–8. doi: 10.1111/j.1754-4505.1985.tb00558.x. [DOI] [PubMed] [Google Scholar]
- 7.Germishuys JJ. Air crash investigation. [last accessed on 2010 Sep 9]. Available from: http://www.desastres.unanleon.edu.ni/pdf/2003/enero/pdf/eng/doc1953/doc1953-7c.pdf .
- 8.Chaturvedi TP, Upadhayay SN. An overview of orthodontic material degradation in oral cavity. Indian J Dent Res. 2010;21:275–84. doi: 10.4103/0970-9290.66648. [DOI] [PubMed] [Google Scholar]
- 9.Stavrianos C, Stavrianou I, Kafas P. Denture identification system based on Swedish guidelines: A forensic aspect. Internet J Forensic Sci. 2008;3 [Google Scholar]
- 10.Thomas CJ. The role of the denture in identification: A review. J Forensic Odontostomatol. 1984;2:13–6. [PubMed] [Google Scholar]
- 11.Richmond R, Pretty IA. Contemporary methods of labeling dental prostheses—A review of the literature. J Forensic Sci. 2006;51:1120–6. doi: 10.1111/j.1556-4029.2006.00238.x. [DOI] [PubMed] [Google Scholar]
- 12.Thomas CJ. The role of the denture in identification. [last accessed on 2010 Sep 15]. pp. 353–8. Available from: http://www.desastres.unanleon.edu.ni/pdf/2003/enero/pdf/eng/doc1953/doc1953-7c.pdf .
- 13.Ryan LD, Keller JB, Rogers DE, Schaeffer L. Clear acrylic resin T-bar used in denture identification. J Prosthet Dent. 1993;70:189–90. doi: 10.1016/0022-3913(93)90017-i. [DOI] [PubMed] [Google Scholar]
- 14.Ling BC, Nambiar P, Low KS, Lee CK. Copper vapour laser ID labelling on metal dentures and restorations. J Forensic Odontostomatol. 2003;21:17–22. [PubMed] [Google Scholar]
- 15.Richmond R, Pretty IA. A range of postmortem assault experiments conducted on a variety of denture labels used for the purpose of identification of edentulous individuals. J Forensic Sci. 2009;54:411–4. doi: 10.1111/j.1556-4029.2009.00987.x. [DOI] [PubMed] [Google Scholar]
- 16.Wilson DF, Kolbinson D. The heat resistance of a data encoded ceramic microchip identification system. Am J Forensic Med Pathol. 1983;4:209–15. doi: 10.1097/00000433-198309000-00006. [DOI] [PubMed] [Google Scholar]
- 17.Raymond R, Pretty IA. The use of radio-frequency identification tags for labeling dentures—scanning properties. J Forensic Sci. 2009;54:664–8. doi: 10.1111/j.1556-4029.2009.01010.x. [DOI] [PubMed] [Google Scholar]
- 18.Colvenkar SS. Lenticular card: A new method for denture identification. Indian J Dent Res. 2010;21:112–4. doi: 10.4103/0970-9290.62813. [DOI] [PubMed] [Google Scholar]
- 19.Jagdev PS, Mehrotra P, Rastogi N. Forensic orthodontics – An Innovation. Indian J Forensic Odontol. 2009;2:9–12. [Google Scholar]
- 20.Agülolu S, Zortuk M, Beydemi K. Denture barcoding: A new horizon. Br Dent J. 2009;206:589–90. doi: 10.1038/sj.bdj.2009.477. [DOI] [PubMed] [Google Scholar]
- 21.Anehosur GV, Acharya AB, Nadiger RK. Usefulness of patient photograph as a marker for identifying denture-wearers in India. Gerodontology. 2010;27:272–7. doi: 10.1111/j.1741-2358.2009.00316.x. [DOI] [PubMed] [Google Scholar]
- 22.Bushick RD. Forensic dentistry: An overview for the general dentist. Gen Dent. 2006;54:48–52. [PubMed] [Google Scholar]
- 23.Stenberg I, Borrman HI. Dental condition and identification marking of dentures in homes for the elderly in Goteborg, Sweden. J Forensic Odontostomatol. 1998;16:35–7. [PubMed] [Google Scholar]
- 24.Pretty IA, Sweet D. A look at forensic dentistry—Part 1: The role of teeth in the determination of human identity. Br Dent J. 2001;190:359–66. doi: 10.1038/sj.bdj.4800972. [DOI] [PubMed] [Google Scholar]
- 25.Matsumura H, Shimoe S, Nagano K, Tanoue N. International telephone code used for citizenship identification in a denture. J Oral Sci. 2007;49:337–40. doi: 10.2334/josnusd.49.337. [DOI] [PubMed] [Google Scholar]