

Abstract
Bioterrorism, the deliberate, private use of biological agents to harm and frighten the people of a state or society, is related to the military use of biological, chemical, and nuclear weapons. Attacks with biological agents are among the most insidious and breed the greatest fear. Attacks could go undetected for a long time, potentially exposing a vast number of people, who are unaware of the threat. Dentist's responses to catastrophes have been redefined by bioterrorism. Accurate and substantial information given to the public by credible public health and medical experts can do much to allay their fears and encourage their cooperation and participation in constructive, organized community response efforts. The dental profession could potentially play a significant role in the emergency response to a major bioterrorism attack.
Keywords: Biological agents, biological weapons, bioterrorism
Introduction
Bioterrorism covers a very broad spectrum of concerns, from catastrophic terrorism with mass casualties, to microevents using low technology but producing civil unrest, disruption, disease, disabilities, and death.[1] The threat of bioterrorism, long ignored and denied, has heightened over the past few years. We are ill prepared to deal with a terrorist attack that employs biological weapons. As was done in response to the nuclear threat, the medical community should educate the public and policy makers about the threat. In the longer term, we need to be prepared to detect, diagnose, characterize epidemiologically, and respond appropriately to biological weapons use and the threat of new and re-emerging infections. On the immediate horizon, we cannot delay the development and implementation of strategic plans for coping with civilian bioterrorism.[2]
History
The use of biological weapons for terror is ancient.
Assyrian politicians dumped fungus from rye into their opponents′ wells, giving them fatal ergot poisoning in 650 BC.[3]
Armies besieging a town relied on increased disease among the defending population and threw dead animals into water supplies, to spread it.[3]
Tatars of the 14th century spread bubonic plague by catapulting diseased corpses into towns.[3]
In World War I, United States and Germany developed biological weapons to contaminate animal fodder.[3]
In Cold War, United States and Soviet Union created arsenals of biological agents for use in battle and against civilian populations.[3]
Dr. Anton Dilger worked with cultures of anthrax and glanders, between 1915 and 1916, with the intention of biological sabotage on behalf of the German Government.[4]
Modern bioterrorist incidents
In 1984, pseudo-Buddhist Rajneeshee cult distributed Salmonella in restaurants and grocery stores in Oregon to poison civic leaders and gain control of the local Government.[3]
In 1992, Russia had the ability to launch missiles containing weapons-grade small pox. A number of terrorist organizations, including Al-Qaeda, have explored the use of biological agents.[3]
In 1995, Sarin gas was released in a Tokyo subway, by the religious sect Aum Shinrikyo, which immediately killed 12 and hospitalized 5000 people.[3]
In 2001, letters containing anthrax spores were mailed to a television news anchor, US senator, and others, leading to the death of a few people and hospitalization of a few others.[3]
Biological Agents
The Center for Disease Control and Prevention ranks the biological agents and diseases that have the potential to be used as weapons into 3 categories.[5,6]
Category A: These agents are characterized by ease of dissemination and transmission of disease with high mortality rate, likelihood of causing public panic and social disruption [Table 1].
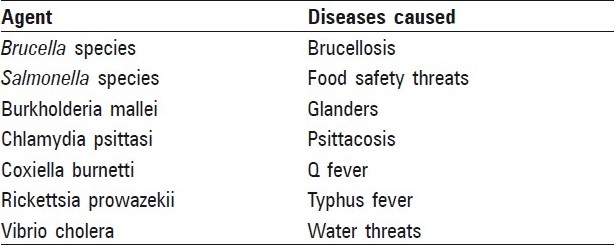
Category B: These agents disseminate less easily, have lower morbidity and mortality rate [Table 2].
Category C: Tan viruses comprise this category. These could be used for mass dissemination in the future because of their availability, ease of production, dissemination, and high morbidity and mortality rates.
Table 1.
Category A biological agents (CDC)
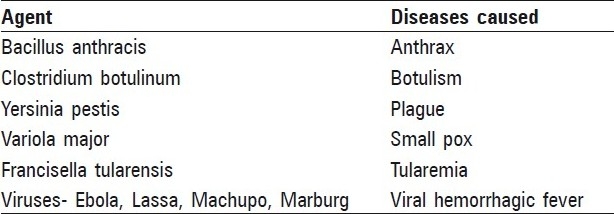
Table 2.
Category B biological agents (CDC)
Role of a dentist in response to a bioterrorism attack
Dentistry can contribute valuable assets, both in personnel and in facilities, to the preparation for and in the immediate response to a bioterrorist attack and its aftermath. These assets can make a significant difference in the outcome. In a major bioterrorist attack, the local needs could be massive and immediate. As hospitals become filled, alternate sites for the provision of health care may be required, and dental offices could fill that need.[7]
Preparation before an attack
Education of the dental profession regarding the medical and oral manifestations of diseases that may result from a bioterrorist attack will be important. Formal plans for an organized response by dental personnel in case of an attack must be developed, integrated into each community's response plan, and practiced periodically. Dental offices are equipped with potentially useful equipment and supplies and should be prepared to serve as decentralized auxiliary hospitals in case the need arises. Educational programs that provide information about potential biological weapons should be developed and made available to dentists through continuing education courses and to dental students as a part of the dental school curriculum.[7]
Up-to-date sources of information should be developed that can be accessed quickly during an attack and reference materials that can be distributed for use as needed. These quick references should be able to provide dentists with a sufficient level of information concerning the particular agent used in an attack to enable them to respond effectively. Dentists have contact with the general public on a regular basis. Armed with knowledge and connected to scientifically based information sources about agents that may be used in bioterrorism, dentists can educate their patients and correct misinformation that may be circulating throughout the general public. Special training may be needed for risk communication. Dental offices are located throughout any given community and have many of the resources that hospital facilities have: sterilization equipment, air and gas lines, suction equipment, radiology capabilities, instruments, and needles. They may be called on to serve as local “minihospitals” when local hospital facilities become overwhelmed or when the concentration of patients is to be avoided, as in attacks involving contagious agents. Predesignated dental offices may act as stockpiling sites for materials and supplies to be distributed in the event of an attack.[7]
The key to successful preparation for an effective response to a major bioterrorism attack is the development of a response plan that is integrated into each community's disaster response plan and testing it by conducting mock attacks.[7]
Assistance during an attack
The assistance that dentists and other dental personnel can provide during the first few days of a significant bioterrorist attack will vary according to the needs of the community and the resources available. These may run the gamut from the packaging of medications in individual doses to providing a major portion of primary medical care in a quarantined area if physicians are unavailable because they have become disabled or have died.[7]
In 1999, the University of Pittsburgh's Center for Biomedicalnone Informatics deployed the first automated bioterrorism detection system, called Real-Time Outbreak Disease Surveillance (RODS). RODS is designed to collect data from many data sources and use them to perform signal detection, that is, to detect a possible bioterrorism event at the earliest possible moment. RODS, and other systems similar to it, collect data from sources, including clinic data, laboratory data, and data from over-the-counter drug sales.[8]
Surveillance and Notification
Disease surveillance systems are critical not only for the initial detection of an outbreak but also for monitoring the extent and spread of the outbreak and for determining when it is over. Managing a large outbreak would require gathering information from contact tracing and source-of-exposure investigations, as well as information about the availability of critical medicine, medical equipment, and the handling of corpses.[9]
Since there is incubation period before the clinical manifestations of diseases that have been used as weapons in bioterrorist attacks become apparent, the initial recognition that an attack has been perpetrated may be difficult. Dentists can serve as an excellent surveillance resource, as they can detect characteristic intraoral or cutaneous lesions, if they are present and report them to public health authorities. They also may be able to detect unusual patterns of employee absences or patients′ cancelling or missing appointments that are not explainable by recognizable local circumstances. These occurrences may well be a harbinger of serious events about to happen.[7]
Diagnosis and Monitoring
Besides assisting in the early identification of the disease or diseases introduced in a bioterrorist attack, dentists can provide individual patient diagnosis by observing the physical and behavioral signs people manifest when the nature of the attack has been determined. Salivary swabs may yield important diagnostic or treatment information and can be collected by dentists for laboratory testing to determine diagnosis when necessary or to monitor treatment progress.[7]
Referral
Dentists can refer suspicious cases to the appropriate specialists for confirmation, treatment, or both.[7]
Immunizations
In the event that rapid inoculation or vaccination of the public is required to prevent the spread of infection by a biological agent, dentists may be recruited to assist in a mass inoculation program.[7]
Triage
Whenever there are a greater number of casualties that the medical care system cannot accommodate or whenever medical care resources are overwhelmed, some system for establishing priorities for treatment must be established. Appropriately trained dentists can fulfill this function, thus freeing up medical professionals to provide definitive care for the large number of patients. This system should be established now, in preparation for potential future attacks.[7]
Medical care augmentation
Because of their training and experience, many dentists may be able to augment and assist medical and surgical personnel in providing definitive treatment for victims of bioterrorist attacks. Some of the services dentists may provide include the following:
treatment of cranial and facial injuries;
providing or assisting in administration of anesthesia;
starting intravenous lines;
performing appropriate surgery and suturing;
assisting in shock management;
assisting in stabilizing patients;
collecting preantibiotic blood samples;
taking medical histories; and
providing cardiopulmonary resuscitation.[7]
Decontamination and Infection Control
Dentists and dental auxiliaries are well versed in infection control procedures and can apply their knowledge in reducing the spread of infections—between patients and between patients and caregivers—in mass disasters. The decontamination of casualties, when appropriate, can be accomplished effectively by dental personnel. Dentists who have experience in practicing in a hospital setting may be especially valuable and may be particularly equipped to provide services that require a close working relationship with physicians.[7]
After the initial attack
Dentists trained in forensic odontology will work closely with local Disaster Mortuary Operational Response Teams, (DMORTs). Dentists also may provide local surveillance to detect any spreading of disease beyond the original area of attack or re-emergence of infections in the original attack area.[7]
Conclusion
Terrorism with biological weapons is likely to remain rare. Because the magnitude of the threat is so difficult to calculate, however, it is sensible to focus on dual-use remedies: pursuing medical countermeasures that will improve public health in general, regardless of whether major biological attacks ever occur. This would include strengthening the international system of monitoring disease outbreaks in humans, animals, and plants and developing better pharmaceutical drugs.[10] The current public discussion of the threat of biologic terrorism is an opportunity to evaluate our collective capabilities and to assess weaknesses and vulnerabilities. Raising the level of national preparedness will require leadership and action by responsible federal agencies. A thoughtful analysis of the consequences of unpreparedness provides a mandate for action.[11] For longer-term solutions, the medical community must educate both the public and policy makers about bioterrorism and build a global consensus condemning its use.[2] Dentists can provide a valuable service to their patients and communities by providing quality information about the potential for attacks, what to watch for, and how to respond appropriately should an attack occur.[12]
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Hamburg MA. Addressing Bioterrorist Threats: Where Do We Go from Here? Emerg Infect Dis. 1999;5:564–5. doi: 10.3201/eid0504.990421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Henderson DA. Bioterrorism as a public health threat. Emerg Infect Dis. 1998;4:488–92. doi: 10.3201/eid0403.980340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. [last accessed on 2009 Nov 05]. Available from: http://www.answers.com/bioterrorism .
- 4. [last accessed on 2009 Nov 05]. Available from: http://www.wikipedia.com/bioterrorism .
- 5.Centers for Disease Control and Prevention CDC. Recognition of illness associated with the intentional release of biological agent. MMWR Morb Mortal Wkly Rep. 2001;50:893–7. [PubMed] [Google Scholar]
- 6.Rotz LD, Khan AS, Lillibridge SR, Ostroff SM, Hughes JM. Public health assessment of potential biological terrorism agents. Emerg Infect Dis. 2002;8:225–30. doi: 10.3201/eid0802.010164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Guay AH. Dentistry's response to bioterrorism: A report of a consensus workshop. J Am Dent Assoc. 2002;133:1181–7. doi: 10.14219/jada.archive.2002.0359. [DOI] [PubMed] [Google Scholar]
- 8.Chmar JE, Ranney RR, Guay AH, Haden NK, Valachovic RW. Incorporating bioterrorism training into dental education: Report of ADA-ADEA terrorism and mass casualty curriculum development workshop. J Dent Educ. 2004;68:1196–9. [PubMed] [Google Scholar]
- 9.Hoffman RE. Preparing for a bioterrorist attack: legal and administrative strategies. Emerg Infect Dis. 2003;9:241–5. doi: 10.3201/eid0902.020538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Stern J. The Prospect of domestic bioterrorism. Emerg Infect Dis. 1999;5:517–22. doi: 10.3201/eid0504.990410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Russell PK. Biologic terrorism - responding to the threat. Emerg Infect Dis. 1997;3:203–4. doi: 10.3201/eid0302.970217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Han SZ, Alfano MC, Psoter WJ, Rekow ED. Bioterrorism and catastrophe response: A quick-reference guide to resources. J Am Dent Assoc. 2003;134:745–52. doi: 10.14219/jada.archive.2003.0261. [DOI] [PubMed] [Google Scholar]