

Abstract
Aims and Objectives:
To identify existence of elder abuse among the patients seeking prosthetic rehabilitation of missing teeth.
Materials and Methods:
This study was conducted on 300 patients aged 65 years and above. It included 238 males and 62 females. A questionnaire prepared by a psychologist was used to evaluate the patient in various aspects of neglect.
Results:
The results revealed that 40% of the total subjects that were studied were suffering from neglect in one way or the other.
Conclusion:
The results conclude that elder negligence was highly prevalent in elder patients who report to the dental office seeking oral prosthetic rehabilitation.
Keywords: Elder abuse, elder maltreatment, elder neglect, forensic, geriatric, homicide, suicide
Introduction
Each year millions of elderly persons suffer as a result of maltreatment.[1] As the number of elders age 65 and older increases, the number of maltreatment cases is expected to rise.[2,3] Elder maltreatment can be divided into six categories:- physical abuse, sexual abuse, neglect, psychological abuse, financial exploitation and violation of rights.[4–6] Elder neglect is complex and sometimes fatal. India has about 7.7% of elderly population[7] which means that there are 77 million older persons at present and the number is going to grow to 177 million in another 25 years. On one side of the globe, elderly people of developed countries contemplate plastic surgical procedures like facelifts, liposuction or laser skin resurfacing so that they are able to smile confidently and improve their self-esteem; on the other hand we are still in a mode of denial that our elderly population is not secure and living among us without suffering.
According to a study done in United States by Elderly Abuse Intervention Team (EAIT), the most common abuse identified was emotional (59%), followed by financial (54%) and physical (33%). The abuser most often were son (38%), spouse (16%), daughter (13%) and others (16%). Although the incidence was high but reporting of abuse by the elderly was very low. The victim conceals the situation for reasons like fear of retaliation by the abuser, fear of being institutionalized, dependence on the abuser and fear of losing respect of the family in the society.[8] India also has seen a growth of life expectancy among its population along with growth in number of elderly people. India faces a tough task to secure its elder population in every sector – financial, health, shelter and culture. The living places are getting smaller and congested, causing stress in families. Even though the elderly are co residing with their families, marginalization, isolation and insecurity is felt among them, due to the generation gap and rapidly changing lifestyles. Indian culture gives lot of respect and support to elders, which is why elder neglect has always been considered as problem of western countries. However, the coping capacities and tolerance of younger and older family members are now being challenged and more often than not, their difference in behavior and attitude toward older people, cannot be labeled as such. There are many incidents that have been reported in Indian media especially in metropolitan cities where criminals are targeting elderly people and/or where a servant is exploiting an elder, who has been abandoned. These incidents are directly a consequence of neglect by the families.
Although elder neglect occurs across all socioeconomic, racial and religious lines, yet it is typically under-reported in most cultures. Prevalence rates/estimates exist only in selected developed countries.[9] Although estimates vary, it is generally believed that 4-6% of the elderly are abused. Two-thirds (2/3) of victims of elder abuse are women. There are only few small-scale studies in India regarding elder abuse especially in the form of neglect.[10,11] Many factors lead to the mistreatment of the elderly including: elderly persons need for care giving, dependency of people on the elderly, mental impairments, isolation, inadequate living arrangements, inability to perform daily functions, frailty, family conflict, poverty, alcohol or drug abuse of the caregiver or other socioeconomic issues.
Lack of understanding regarding the forensic aspects of elder mistreatment could be misleading and would allow the perpetrator to go free. Signs of abuse (in the form of neglect) in the elderly are usually missed and are rarely determined to be cause of death. The World Health Organization (WHO) has recognized the need to develop a global strategy for the prevention of the abuse of older people. WHO recommends making primary health care workers aware of the problem, a crucial step in preventing and/or managing elder abuse.[12] Even the American Medical Association recommends that physicians routinely enquire about possible mistreatment of elderly patients. The American Medical Association recommendations include incorporating routine questioning related to elder abuse and neglect into daily clinical practice.[13]
Aims and objective
To prepare a standard questionnaire which would allow health care professionals like nurses, orthopedicians, general surgeons and physicians, ophthalmologists, physiotherapists, prosthodontists, endodontist, community dentist, dietician, neurosurgeons, psychologists to identify elder neglect.
To estimate the prevalence of elderly neglected patients in a dental out-patient department who seek artificial dentures.
To promote awareness of the subject among all health care professionals.
To collect data for future forensic considerations in the area of the survey.
Materials and Methods
This study was done on 300 patients (238 males and 62 females) and was carried out in the Department of Prosthodontics. Patients, above 65 years, who came for complete denture fabrication, were randomly selected for this study. A questionnaire was prepared with the help of a clinical and experienced psychologist to evaluate the patient in various aspects of neglect [Table 1]. To standardize the language of the questionnaire, it was translated to Hindi language and back translated to English language by independent translators. Both, the original English version and back-translated English version, were compared and accepted when they revealed the same meaning. Hindi version was used to take the interview. Based upon this questionnaire, patients were interviewed. Interview was not taken at the first appointment. Good rapport with the patient was necessary to elicit the truth. Patients were assured regarding the confidentiality of information given by them. To verify the reliability of the answers same questions were asked to patients at different appointments also. Data obtained through the interview was analyzed, discussed and categorized with the help of psychologist.
Table 1.
Questionnaire
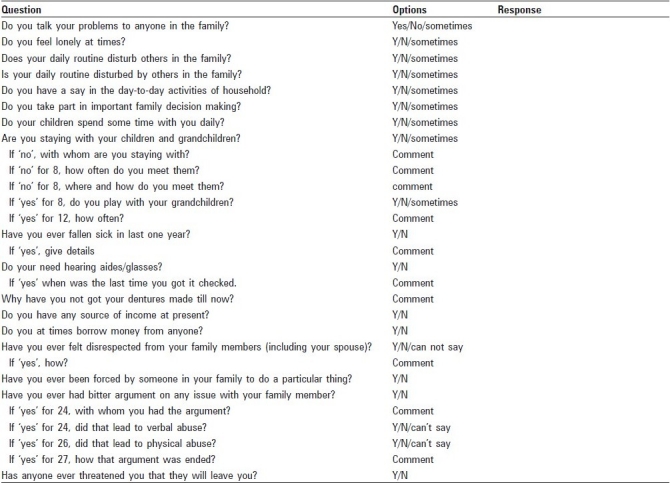
The questionnaire formulated [Table 1] identified elder neglect. Others like exploitation, abandonment and conflict may also coexist and can be identified.
Results
Out of 300 patients interviewed, 60% belonged to rural population. Facts obtained from the analysis of the data were astonishing. Forty-three percent of the total elders, one or the other way, were found to be abused. Majority of them (40%) were neglected. Three percent was physically and socially abused. Elders were so neglected that 27% even do not talk their problems to others and have no say in the family. Thirty-three percent elder were not considered while making the important family decisions. For 33% elders, their children do not spend time daily with them. Even 13% elder did not get suggestions from the family members when needed. Thirteen percent of elders were not getting proper respect from the family members. Thirty percent elders were disrespected by the family members. Thirty-three percent elders faced verbal abuse and 3% encountered with physical abuse.
Discussion
There is little doubt that our lifestyle has changed much during the last few decades. In most of the metropolitan cities all over the world people have to work, in fact slog throughout the day, week or a month to make a good living. Many of us have little time for even ourselves. Even developed countries like United States in year 1992, have enacted the Family Violence Prevention and Services Act,[14] which directs that a study of the national incidence of abuse, neglect and exploitation of elderly persons be conducted.[14] This lead to national elder abuse incidence study. Elder neglect is defined as the refusal or failure to fulfill any part of a person's obligation or duties to an elder.[14] Neglect typically means the refusal or failure to provide an elderly person with such life necessities as food, water, clothing, shelter, personal hygiene, medicine, comfort, personal safety and other essentials as a responsibility of agreement.[14,15]
Risk factors for neglect by family members includes psychopathology, transgenerational violence, economic dependency upon victim, isolation, family member unengaged outside of the household, caregivers stress and living arrangement (perpetrator living with victim, overcrowding). Inherent factors in the elder that appear to put him/her at risk include dementia, physical impairment, provocative actions of the elder, guilt and a fear of retaliation.[15–21]
Elder neglect is a growing concern globally. Tackling such a sensitive issue requires involvement of health care workers at all levels. It is an acceptable fact that a vast majority of elders come in contact with specialists like prosthodontists. Mental attitude of a patient who is suffering from abuse in any form will definitely affect the outcome of any treatment.
The present study was aimed to identify the existence and prevalence of elder abuse especially neglect among the patients that a prosthodontist sees in his everyday OPD. Prosthodontist is one such specialist who encounters geriatric patients daily and majority of his patients are elderly. The subjects of the present study were chosen randomly from the dental out patient and out of 300 patients, 62 were females and 238 were males. Less number of female patients coming to seek complete denture treatment could be either due to self-neglect, neglect by those on whom they are dependant, financial dependence or ignorance. In the present study it was noted that 85% of the females were dependant out of which 53% were dependant on their spouse, 40% on their son and the rest on others.
About 44% of the total patients were abused in one form or the other, majority of them were neglected. Psychological abuse of females was more common and was attributed to their neglect by their son and the influence that their daughter-in-law had over their son after marriage. Their inability to take self-related decisions was a major factor which they revealed possible for their psychological depression. Indifference, unhappiness, sorrow and negative attitude was evident during the course of rapport build-up with such patients.
All the female patients that were interviewed were housewives and were dependant either on their husband or their children for finance. Financial dependence seemed to make a person more prone to be exploited, as is evident by the fact that 60% of males who had retired from government service and were receiving pension were less abused in any form. Patients who were still in business also were found to be less prone to be abused. Patients irrespective of their past status were seen to be more abused as they were dependant financially on their children for everything. Dependence on son was common followed by spouse. Neglect by the son had made 22 patients to seek financial help from their other relatives. There was no correlation found between the financial status of the son with neglect. Patients whose children especially son were financially sound, were facing the same problem.
Physical abuse was uncommon except in cases where influence of alcohol often led to verbal abuse followed by a brawl and beating of the elderly. There was no physical abuse of females reported which could be associated with respect for tradition and culture or may be did not want to reveal. Physical abuse of the elderly can be a determinant of death and the forensic investigator needs to be familiar with the signs of neglect which are evident from the living conditions of the sufferer.
Negligence on part of the children and or spouse often led to bitter arguments with family members in patients being abused. The argument with daughter-in-laws was more common in females. Irrespective of that one-third of the arguments would lead to verbal abuse being rendered to the elderly by the children.
Loneliness was common among patients suffering from neglect. The elders who were not being consulted or informed about family decisions felt that their day-to-day activity was considered as disturbance to their family members and more commonly children who were not spending time with their parents made the elderly feel more lonely and isolated. They feel so lonely that they would not talk their problems to anyone in the family. Those elders who were staying with their children but were not able to play with their grandchildren were more expressive in their feelings. The busy schedule of the young children (schools) was also an important factor that grandchildren would neglect their grandparents.
Neglect and loneliness of an elder especially those without a spouse can lead to suicide. The problem of an elder is his age and this very age becomes an escape route for the perpetrator. If an elder person commits suicide, the perpetrator would easily get away, by blaming the age and health of the deceased and most of us would believe it. It is only untimely death of a young one, when the community gets suspicious and police is called to investigate. Recognizing fatal neglect is challenging especially with concurrent organic disease.
Disrespect from family members was found in the form of verbal abuse, ignoring what elders had to say, not paying attention to what opinion they hold, not allowing elders to decide their own things, making faces and not attending them even when they were sick.
Common physical findings in cases of elder neglect consisted of dehydration, malnutrition/starvation, poor hygiene, untreated medical conditions and neglect of existing medical conditions. About 75% of the patients interviewed documented poor overall hygiene including untidy clothing. This could be associated with the poor status of the family. Thirty-five cases were found to be dressed in torn clothes.
Five percent of the patients showed hearing impairment and 23% showed signs of impaired vision. Out of which only five were wearing glasses which were regularly updated. The rest of them could not afford on their own and were hesitant to ask their children.
Summary and Conclusion
The biggest users of health care system are the elderly people who occupy around two-thirds of hospital beds. A report to the United Kingdom parliament estimated that around 500,000 elderly people may be abused with up to two-thirds of cases occurring in their own homes. More alarming was that abuse of the elderly was not only restricted to their homes, but it took place in nursing homes, residential care, hospitals and sheltered housings. Among various professionals, doctors have the moral and ethical responsibility to understand undermining problems of their patients. In dentistry, prosthodontics is one field where a large majority of patients fall in geriatric category. A prosthodontist, among other professionals, has a key role to play to identify the existence and the impact that abuse can have on his patient. Dental education needs to cover this aspect of forensic science and train every dental student how to identify abuse of his patient in any form. Currently, more than 15,000 dental graduates are added every year to the total trained dental manpower. More than 60 institutions offer postgraduate training in various specialties in dentistry to produce postgraduates within the nine recognized specialties. Approximately about 450 prosthodontists are joining the brigade each year. This makes dentist a potent source to identify elder abuse and neglect. Elder abuse could be a determinant of a suicide or a homicide. Forensic dentistry needs to evolve and studies need to be directed to identify elder abuse rather than merely depend on non-government organizations.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Dong XQ. Medical implications of elder abuse and neglect. Clin Geriatr Med. 2005;21:293–313. doi: 10.1016/j.cger.2004.10.006. [DOI] [PubMed] [Google Scholar]
- 2.Cowen HJ, Cowen PS. Elder mistreatment: Implications for public health dentistry. J Public Health Dent. 2001;61:131–7. doi: 10.1111/j.1752-7325.2001.tb03379.x. [DOI] [PubMed] [Google Scholar]
- 3.Grossman MD, Miller D, Scaff DW, Arcona S. When is an elder old? Effect of preexisting conditions on mortality in geriatric trauma. J Trauma. 2002;52:242–6. doi: 10.1097/00005373-200202000-00007. [DOI] [PubMed] [Google Scholar]
- 4.A Profile of Older Americans. Washington, DC: American Association of Retired Persons; 1993. Program Resources Department, American Association of Retired persons, Administration on Aging, US Department of Health and Human Services. [Google Scholar]
- 5.Collins KA, Bennett AT, Hanzlick R. Elder abuse and neglect. Arch Intern Med. 2000;160:1567–8. doi: 10.1001/archinte.160.11.1567. [DOI] [PubMed] [Google Scholar]
- 6.Silverman TN. Abuse of the elderly through fraud and deception. Psychiatr Hosp. 1983;14:104–7. [PubMed] [Google Scholar]
- 7.Soneja S. Elder abuse in India.Country report for world health organization. Help age India [Google Scholar]
- 8.Elder abuse – Questions and Answers. Developed by Elder Abuse Intervention Team (EAIT) 2007 Jun 11; [Google Scholar]
- 9.Comijs HC, Pot AM, Smit JH, Bouter LM, Jonker C. Elder abuse in the community: Prevalence and consequences. J Am Geriatr Soc. 1998;46:885–8. doi: 10.1111/j.1532-5415.1998.tb02724.x. [DOI] [PubMed] [Google Scholar]
- 10.Shah G, Veedon R, Vasi S. Elder abuse in India. J Elder Abuse Negl. 1995;6:101–18. [Google Scholar]
- 11.Chokkanathan S, Lee AE. Elder Mistreatment in Urban India.A Community Based Study. J Elder Abuse Negl. 2005;17:45–61. doi: 10.1300/j084v17n02_03. [DOI] [PubMed] [Google Scholar]
- 12.Mattoo KA, Shalabh K, Khan A. Prevalence of elder abuse among completely edentulous patients seeking complete denture prosthesis: A survey. J Indian Acad Geriatr. 2009;5:177–80. [Google Scholar]
- 13.Chicago, IL: American Medical Association; 1992. American medical association Diagnostic and treatment guidelines on elder abuse and neglect. [Google Scholar]
- 14.Dolan V. Risk factors for elder abuse. J Insur Med. 1999;31:13–20. [PubMed] [Google Scholar]
- 15.Abyad A. Elder abuse: Diagnosis, management and prevention. Med Interface. 1996;9:97–101. [PubMed] [Google Scholar]
- 16.Paris BE. Violence against elderly people. Mt Sinia J Med. 1996;63:97–100. [PubMed] [Google Scholar]
- 17.Breckman RS, Adelman RD. Newbury Park: Sage Publications; 1989. Strategies for helping victims of elder mistreatment; pp. 35–6. [Google Scholar]
- 18.Hansberry MR, Chen E, Gorbein MJ. Dementia and elder abuse. Clin Geriatr Med. 2005;21:315–32. doi: 10.1016/j.cger.2004.11.002. [DOI] [PubMed] [Google Scholar]
- 19.Lachs MS, Pillemer K. Elder abuse. Lancet North Am Ed. 2004;364:1263–72. doi: 10.1016/S0140-6736(04)17144-4. [DOI] [PubMed] [Google Scholar]
- 20.Akaza K, Bunai Y, Tsujinaka M, Nakamura I, Nagai A, Tsukata Y, et al. Elder abuse and neglect: Social problems revealed from 15 autopsy cases. Leg Med (Tokyo) 2003;5:7–14. doi: 10.1016/s1344-6223(02)00057-3. [DOI] [PubMed] [Google Scholar]
- 21.Joshi S, Flaherty J. Elder abuse and neglect in long term care. Clin Geriatr Med. 2005;21:333–54. doi: 10.1016/j.cger.2004.10.009. [DOI] [PubMed] [Google Scholar]