

Abstract
Objective
To determine whether the installation of deep tube wells to reduce exposure to groundwater arsenic in rural Bangladesh had an effect on the incidence of childhood diarrhoeal disease.
Methods
Episodes of diarrhoeal disease in children aged under 5 years that occurred on one specified day each month between 2005 and 2006 were reported to community health workers for six rural villages. A geographical information system containing details of household water use and sanitation in the villages was built using data obtained by a global positioning system survey. The information system also included health, spatial and demographic data. A field survey was carried out to determine whether households obtained drinking water from deep tube wells installed in 2005. The effect of deep tube well use on the incidence of childhood diarrhoea was assessed using a random effects negative binomial regression model.
Findings
The risk of childhood diarrhoea was 46% lower in the 179 households that used a deep tube well than in the 364 that used a shallow tube well (P = 0.032). Neither socioeconomic status, latrine density, population density nor study year had a significant influence on disease risk. The incidence of childhood diarrhoea declined dramatically between 2005 and 2006, irrespective of water source.
Conclusion
The introduction of deep tube wells to reduce arsenic in drinking water in rural Bangladesh had the additional benefit of lowering the incidence of diarrhoea among young children.
ملخص
الغرض
تحديد ما إذا كان تركيب أنابيب آبار المياه العميقة لتقليل التعرّض للزرنيخ الموجود في المياه الجوفية في المناطق الريفية في بنغلاديش سيكون له تأثير على معدّل وقوع أمراض الإسهال بين الأطفال.
الطريقة
أبلغ عن وقوع الإسهال في الأطفال أقل من عمر 5 سنوات الذي حدث في يوم محدد في كل شهر بين عامي 2005 و 2006 إلى العاملين الصحيين في ست قرى ريفية. وأُعد نظام معلومات جغرافي يتضمن تفاصيل عن استخدام المياه والإصحاح المنزلي في تلك القرى باستخدام المعطيات المتحصل عليها من مسح نظام التحديد الجغرافي العالمي. كما تضمن نظام المعلومات أيضاً معطيات صحية، وديموغرافية، ومعطيات عن الموقع. وأُجري مسح ميداني لتحديد الأسر التي حصلت على مياه شرب من أنابيب آبار المياه العميقة التي تم تركيبها قبل عام 2005. وحُسِبَ تأثير استخدام أنابيب الآبار العميقة على وقوع الإسهال بين الأطفال باستخدام تأثيرات عشوائية لنموذج تحوّف ثنائي سلبي.
النتائج
كان اختطار الإصابة بالإسهال في الأطفال أقل بنسبة 46% في 179 أسرة استخدمت أنابيب الآبار العميقة مقارنة بـ 364 أسرة استخدمت أنابيب الآبار الضحلة (قوة الاحتمال P= 0.032). لم يكن هنا تأثير يعتد به للوضع الاجتماعي والاقتصادي، أو لوفرة المراحيض، أو كثافة السكان، أو للسنة التي أجريت فيها الدراسة على اختطار المرض. وقد تراجع معدل وقوع الإسهال بين الأطفال تراجعاً كبيراً بين عامي 2005 و 2006، بغض النظر عن مصدر المياه.
الاستنتاج
كان لإدخال أنابيب الآبار العميقة لغرض تقليل التعرّض للزرنيخ في مياه الشرب في المناطق الريفية في بنغلاديش تأثير إضافي في خفض وقوع الإسهال بين صغار الأطفال.
Resumen
Objetivo
Determinar si la instalación de pozos profundos entubados para reducir la exposición al arsénico subterráneo en zonas rurales de Bangladesh tiene un efecto en la incidencia de la enfermedad diarreica infantil.
Métodos
Entre 2005 y 2006, se notificaron los episodios de enfermedad diarreica en niños menores de 5 años que ocurrieron en un día específico de cada mes a los trabajadores sanitarios de la comunidad de seis pueblos rurales. Se utilizó un sistema de información geográfica que incluye los datos sobre el uso del agua de consumo humano y saneamiento de los pueblos en los que se construyó un pozo de este tipo. Para ello, también se utilizaron los datos obtenidos en un estudio de sistema de posicionamiento global. El sistema de información también incluye datos sanitarios, espaciales y demográficos. Asimismo, se llevó a cabo un estudio de campo para determinar si existían hogares que obtuvieron agua potable de pozos profundos instalados en 2005. El efecto del uso de pozos profundos entubados en la incidencia de la diarrea infantil se evaluó utilizando un modelo de regresión binomial negativa con efectos aleatorios.
Resultados
El riesgo de diarrea infantil fue un 46% inferior en 179 hogares que utilizaron un pozo profundo entubado en comparación con los 364 hogares que utilizaron un pozo poco profundo entubado (P=0,032). Ni el estado socioeconómico, el número de letrinas, la densidad de población, ni el año del estudio influyeron significativamente en el riesgo de la enfermedad. La incidencia de la diarrea infantil descendió drásticamente entre el año 2005 y el año 2006, independientemente de la fuente de agua.
Conclusión
Con la introducción de los pozos profundos entubados para reducir el arsénico en el agua potable de las zonas rurales de Bangladesh se obtuvo el beneficio adicional de reducir la incidencia de la diarrea en niños de corta edad.
Résumé
Objectif
Déterminer si l'installation de puits tubulaires profonds pour réduire l'exposition à l'arsenic des eaux souterraines, dans le Bangladesh rural, a eu un effet sur l’incidence des maladies diarrhéiques chez les enfants.
Méthodes
Les cas de maladies diarrhéiques chez les enfants âgés de moins de 5 ans, qui se sont produits un jour spécifié de chaque mois entre 2005 et 2006, ont été signalés aux agents de santé communautaires de six villages ruraux. Un système d'information géographique contenant les détails de la consommation d'eau des ménages et des installations sanitaires dans les villages a été élaboré, en utilisant les données obtenues par une enquête réalisée au moyen d'un système de positionnement global. Le système d'information comprenait également des données sanitaires, géographiques et démographiques. Une enquête a été effectuée sur le terrain afin de déterminer si les ménages tiraient leur eau potable de puits tubulaires profonds installés en 2005. L'effet des puits tubulaires profonds sur l'incidence des diarrhées infantiles a été évalué à l’aide d’un modèle de régression binomiale négative à effets aléatoires.
Résultats
Le risque de diarrhée infantile était de 46% inférieur chez les 179 ménages utilisant un puits tubulaire profond par rapport aux 364 ménages utilisant un puits tubulaire peu profond (P = 0,032). Ni le statut socioéconomique, ni la densité des latrines, ni la densité de la population et ni l'année de l'étude n'ont eu d'influence significative sur le risque de maladie. L’incidence des diarrhées infantiles a diminué de façon spectaculaire entre 2005 et 2006, quelle que soit la source d'eau.
Conclusion
La mise en place de puits tubulaires profonds pour réduire la présence d'arsenic dans l'eau potable dans les régions rurales du Bangladesh présente l'avantage supplémentaire de réduire l’incidence des diarrhées chez les jeunes enfants.
Резюме
Цель
Определить, повлияло ли сооружение глубоких трубчатых колодцев в сельских районах Бангладеш, предпринятое с целью снижения экспозиции населения к мышьяку, содержащемуся в грунтовых водах, на заболеваемость детей диарейными болезнями.
Методы
В 2005–2006 годах жители шести деревень сообщали местным медработникам о том, что ежемесячно в определенный день у детей в возрасте до 5 лет возникает диарейное заболевание. С использованием данных, полученных путем обследования, основанного на системе глобального позиционирования, была создана система географической информации, которая содержала подробные сведения о водопользовании и канализации в этих деревнях. Система информации включала в себя также медицинские, пространственные и демографические данные. Было проведено полевое исследование с тем, чтобы определить, пользовались ли домохозяйства питьевой водой из глубоких трубчатых колодцев, сооруженных в 2005 году. Воздействие глубоких трубчатых колодцев на заболеваемость детей диареей оценивалось с использованием модели отрицательной биномиальной регрессии со случайными эффектами.
Результаты
В 179 домохозяйствах, пользовавшихся глубоким трубчатым колодцем, риск диареи у детей был на 46% ниже, чем в 364 домохозяйствах, бравших воду из мелкого трубчатого колодца (P = 0,032). Социально-экономический статус, частота размещения туалетов, плотность населения или год проведения исследования не оказывали существенного воздействия на риск заболевания. В 2005–2006 годах заболеваемость детей диареей, независимо от источника водопользования, резко снизилась.
Вывод
Дополнительной пользой от сооружения глубоких трубчатых колодцев с целью снижения потребления питьевой воды, содержащей мышьяк, в сельских районах Бангладеш стало снижение заболеваемости детей младшего возраста диареей.
摘要
目的
:确定孟加拉国农村地区用以降低地下水砷暴露的深管井的安装对儿童发生腹泻的影响。
方法
:将六个农村村庄5岁以下儿童于2005年到2006年期间每个月指定日期发生腹泻的情况汇报给社区卫生人员。采用全球定位系统调查获得的数据,建立一个地理信息系统,包含村庄中家庭用水和卫生用水的详细情况。该信息系统还包括健康、空间和人口数据。另外开展了一次实地调查,确定这些家庭是否从2005年前安装的深管井中获取饮用水。采用随机影响负二项回归模型,评估深管井的使用对儿童发生腹泻的影响。
结果
:179户使用深管井的家庭发生儿童腹泻的风险比364户使用浅管井的家庭低46%(P=0.032)。社会经济状况、公厕密度、人口密度以及研究年份都未对患病风险产生重大影响。2005年到2006年期间,不管水源如何,儿童患有腹泻的发生率都有大幅度的降低。
结论
:在孟加拉国农村地区采用深管井以降低饮用水砷含量的做法还具有额外作用,即可降低婴幼儿发生腹泻的患病率。
Introduction
Diarrhoeal diseases are the second leading cause of death in children aged under 5 years worldwide.1 An estimated 2.5 million cases of diarrhoea occur annually in these children, with Asia and southern Africa accounting for more than half.2 Those living in poor areas with inadequate nutrition are most susceptible to severe diarrhoea and dehydration. Moreover, diarrhoeal diseases are endemic in countries where the water and sanitation infrastructure is deficient, such as Bangladesh.
In Bangladesh, efforts by the United Nations Children’s Fund, the Bangladesh Department of Public Health Engineering and nongovernmental organizations have led to an almost universal shift from the consumption of surface water to groundwater.3 These efforts were in response to the severe burden of diarrhoeal disease in the country and the widespread contamination of surface water with human pathogens. Since the 1970s, the number of tube wells is thought to have doubled roughly every five years throughout rural Bangladesh.4 The majority are private shallow domestic wells, typically < 45 m deep, that were installed using a hand percussion drilling method that is affordable for individual households.5 Currently over 90% of households in Bangladesh obtain drinking water from a total of approximately 10 million, mostly shallow, tube wells.
While the proliferation of tube wells has provided access to drinking water that is much less contaminated with microbial pathogens than surface water, the high level of arsenic frequently found in groundwater has generated a new health problem. A survey carried out in the late 1990s showed that one third of the population of 130 million at the time was drinking water that did not meet the Bangladeshi standard for arsenic in drinking water of 50 µg/l and nearly half the population was exposed to levels that exceeded the guideline of the World Health Organization (WHO) of 10 µg/l.6 In addition to causing the early signs of arsenicosis, such as skin lesions,7 exposure to arsenic by drinking tube well water has increased all-cause mortality8 and cancers of the lung, liver and bladder in adults.9
Nearly 5 million wells were tested for arsenic throughout the affected regions of Bangladesh between 2000 and 2005 under the Bangladesh Arsenic Mitigation and Water Supply Programme. The result was that millions of households stopped drinking from their own shallow high-arsenic wells and switched to neighbouring wells that were low in arsenic, although often also shallow.4,10 It has recently been shown, however, that groundwater pumped from shallow low-arsenic wells is more likely to be contaminated with human waste than groundwater from shallow high-arsenic wells because of the nature of local hydrogeology combined with the high population density and poor sanitation.11,12 This raised the concern that the response of households to the testing of wells for arsenic could have increased exposure to microbial pathogens. More generally, faecal contamination of shallow groundwater may be one reason for the persistence of diarrhoeal disease in Bangladesh.13,14
After switching to a nearby low-arsenic household well, the next most effective means of reducing arsenic exposure from drinking water is to use one of the approximately 165 000 deep wells installed throughout the country by the Bangladesh Department of Public Health Engineering and nongovernmental organizations over the past decade.10,15 These deep wells tap older geological strata that either retain arsenic within aquifer sands or have been flushed of their initial arsenic content.16,17 Most of the deep wells installed by the Department of Public Health Engineering and nongovernmental organizations are over 150 m deep. Typically, deep public tube wells are installed near a road in a central location of a village to maximize access. It has been shown that some villagers are willing to walk up to 150 m several times a day to obtain drinking water from these deep tube wells.18,19 Although the wells were installed to reduce exposure to arsenic, the health effects of switching to these, often more distant, wells has to our knowledge not been systematically investigated. One source of concern is that water obtained from a distant well may be stored for longer in the home, thereby increasing the risk of microbial contamination even though the depth of the public wells might have been expected to offer some additional protection against contamination.13,20,21 The effect of access to deep tube wells on hygiene is likely to be less important because villagers have been encouraged to continue to rely on their household wells for uses other than drinking and cooking.
The International Centre for Diarrhoeal Disease Research in Bangladesh collected an extensive set of data on diarrhoeal disease in the Matlab region of the country in 2005 and 2006. The availability of these data provided a unique opportunity to investigate the relationship between diarrhoeal disease and the use of drinking water from deep tube wells in a population that drinks primarily untreated groundwater.
Methods
Study setting and design
The study was carried out in six villages in the rural region of Matlab, Bangladesh, which is located 50 kilometres (km) south-east of Dhaka. The International Centre for Diarrhoeal Disease Research in Bangladesh has a field site in this area which includes a hospital that provides inpatient treatment of severe diarrhoea free of charge to all residents. The Health and Demographic Surveillance System for the study area is a longitudinal surveillance system that has maintained health and demographic records for all Matlab residents since 1966. Individuals are assigned a unique identification number on entry into the area, following birth or migration. These identification numbers are used to link demographic, health and other data. In addition to data on the population at the household level collected each month under the Health and Demographic Surveillance System, data on socioeconomic status and maternal education were available from a detailed household census conducted in 2005.
Data on the incidence of diarrhoea in children aged under 5 years were collected by female community health workers who asked mothers once a month whether their children had had diarrhoea during the previous 24 hours. A case of diarrhoea was defined as the occurrence of three loose stools in a 24-hour period and episodes reported to have lasted several days were recorded as a single case.22
Geographical database and study variables
The village of Bara Haldia and five neighbouring villages were selected for monitoring the faecal contamination of tube well water because the area contained a high proportion of shallow wells with a low arsenic concentration.12 As part of this study, information on drinking water resources was obtained for 543 households with a total population of 2700 for the years 2008 and 2009. A field survey was conducted to map the water and sanitation infrastructure of the six villages using global positioning system receivers with an accuracy greater than 1 m. Spatial data were differentially corrected by postprocessing to ensure high accuracy and data were incorporated into the geographical information system for the study area. All tube wells, latrines and household locations were mapped and, during the survey, residents provided information on which tube wells they used for drinking water. Households generally obtained drinking water from the nearest tube well within their cluster of patrilineally-related households called baris. Baris that did not own a tube well used drinking wells owned by a neighbouring bari or mosque or a public well. Some households owned a tube well but reported that they used a deep public tube well as the source of their drinking water. It was possible to determine which households obtained drinking water from deep tube wells installed in 2005 and which obtained water from private shallow wells by using knowledge of the ages of the tube wells and information provided by residents.
The study used four time-invariant control variables: the number of latrines within 30 m of a household, the population density in the vicinity of the household, household socioeconomic status and the educational level of the mother in the household. The geographical information system was used to determine the number of latrines around each household and the number of people living within a 30 m radius. The variable for the number of adjacent latrines controls for the effect of sanitation at the local level and the variable for population density controls for the local use of water resources and for the transmission and source strength of contaminants above ground. A categorical socioeconomic status score was developed using principal components analysis. The score was derived from a composite of five dichotomous variables representing the ownership of various household assets (i.e. a bed, bicycle, blanket, lamp and watch) and one ordinal variable that represented the material used to construct the household’s walls. The composite score was divided into quintiles that corresponded to a range of economic levels; higher quintiles reflected higher socioeconomic status.23 The maternal education variable was the number of years of education the mother had received; the average over all households was 3.4 years.
Statistical analysis
The study had a repeated measures design that used data from the six villages which reported childhood diarrhoea in each household during 2005 and 2006. To study the effect of obtaining drinking water from a deep tube well on childhood diarrhoea we considered the number of cases reported in children aged under 5 years on 12 occasions per year during the study period. The numbers were aggregated for 2005 and 2006. Although data on diarrhoeal disease were available from as early as 2000, we used only data from 2005 onwards because the majority of deep tube wells in our study area were installed in that year and it would have been difficult to separate the effect of time on diarrhoea from the effect of deep tube well use. The analysis did not extend beyond 2006 because the collection of comprehensive data on diarrhoeal disease in Matlab ended that year.
Because the study outcome was a count variable with a skewed distribution, we first determined whether our data were drawn from a negative binomial or Poisson distribution by analysing the mean and variance of the outcome. The overdispersion of the data (i.e. the mean was 0.13 cases of diarrhoea per household per year and the variance was 0.17 cases per household per year) indicated that a negative binomial regression model was preferable. This model allowed for overdispersion by using an additional parameter and assuming a gamma distribution. We used a random effects specification to account for the clustered nature of the repeated measures.
Data were arranged using unique identifiers representing n cases over t time periods for a total of n × t observations. The negative binomial regression model below gives the probability that yit = r:
 |
(1) |
where r represents success (e.g. a case of diarrhoea) and so r = 0, 1, 2, … and yit represents the number of cases of diarrhoea in household i at time period t. In this equation, λit is the expected value of yit, θ is the overdispersion parameter and Γ(…) is the gamma function. Next, we assumed that the expected value λit was described by a log-linear regression model, which is given in the following equation in which logλit is expressed as a function of the predictor variables:
| (2) |
where β and γ represent the vectors of coefficients. The outcome is a function of the following: the time-specific intercept μt, time-variant factors xit, time-invariant factors zi and an individual specific error term, αi, that represents unobserved variables that are assumed not to be correlated with the observed variables.
Coefficients for both time-variant and time-invariant predictors can be derived using the random effects negative binomial model and incidence rate ratios for the various predictors can be obtained by exponentiating these coefficients. An incidence rate ratio of one indicates that the independent variable has no effect on the risk of diarrhoea, while a ratio greater than one indicates an increased risk and a ratio below one, a decreased risk.
In this study, use of a deep tube well as the primary source of household drinking water was the time-invariant predictor of interest. Additional time-invariant predictors included in the model were maternal educational level, socioeconomic status and latrine and population density. The model also included a time-variant predictor for the number of children aged under 5 years in the household and a dummy variable for the year to capture the effect of time on the decreasing incidence of diarrhoea. All statistical analyses were carried out using Stata version 11.0 (StataCorp LP, College Station, United States of America).
Results
Of the 543 households within the study area, 179 obtained drinking water from a deep tube well located at a median distance of 41 m from the household (Fig. 1). For the remaining 364 households, the median distance to the nearest deep tube well was 153 m, which probably influenced the residents’ decision to use private shallow tube wells. The incidence of diarrhoea was lower in households that used drinking water from a deep well than in those that used water from a shallow well in both 2005 and 2006 (Fig. 2). The key observation for this analysis is that the proportional decrease in the incidence of diarrhoea between 2005 and 2006 was nearly twice as large in households using a deep tube well than in those using a shallow tube well.
Fig. 1.
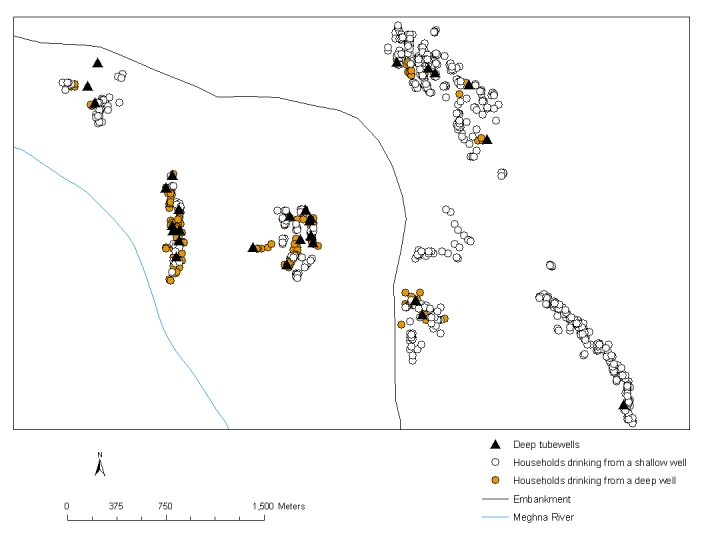
Households and deep tube wells in six villages, Matlab, Bangladesh, 2008–2009
Fig. 2.

Mean annual incidence of diarrhoeal disease in children aged under 5 years in six study villages, by tube well use, Matlab, Bangladesh, 2005–2006
The random effects negative binomial model used data only from households in which children aged under 5 years were present during the study period. Because children “aged” in and out of the community diarrhoea survey between 2005 and 2006, data for each household were used either once or twice during the 2-year study period. As a result, the total number of observations for the 543 households included in the model was 927. The average number of children aged under 5 years in each household was 1.3. In total, 122 cases of diarrhoea were reported in 2005 and 2006.
The incidence rate ratios derived using the random effects negative binomial model for the different predictors are shown in Table 1. The incidence rate ratio for using a deep tube well was 0.541, which implies that the risk of diarrhoea in a child aged under 5 years in a household that used a deep tube well was 46% lower than in a household that used a shallow tube well, after controlling for the number of children aged under 5 years in the household and keeping all other variables constant. This difference was significant (P = 0.032). In addition, a higher level of maternal education tended to reduce the risk of diarrhoea (P = 0.094). Neither socioeconomic status, latrine density, population density nor study year had a significant influence on the risk.
Table 1. Incidence rate ratios (IRR)a for predictors of diarrhoea in children aged under 5 years derived using a random effects negative binomial model,b Matlab, Bangladesh, 2005–2006.
| Predictor | IRR | 95% CI | P |
|---|---|---|---|
| Deep tube well use | 0.541 | 0.308–0.949 | 0.032 |
| No. of children aged < 5 years in the household | 1.988 | 1.434–2.755 | 0.0001 |
| Maternal educational level | 0.932 | 0.858–1.012 | 0.094 |
| Household socioeconomic status | 0.983 | 0.840–1.151 | 0.835 |
| Latrine densityc | 0.977 | 0.882–1.082 | 0.650 |
| Population density in the vicinity of the householdd | 0.999 | 0.987–1.012 | 0.911 |
| Study yeare | 1.371 | 0.914–2.058 | 0.128 |
CI, confidence interval.
a An IRR of 1 indicates that the independent variable has no effect on the risk of diarrhoea, while an IRR greater than 1 indicates an increased risk and an IRR below 1, a decreased risk.
b The model considered 927 observations from a total of 543 households.
c Number of latrines within 30 metres of a household.
d Number of people living within 30 metres of a household.
e The study years were 2005 and 2006.
Discussion
The main result of the study is that obtaining drinking water from a deep public tube well was associated with a significantly lower incidence of diarrhoeal disease in children aged under 5 years. It appears that factors associated with using a deep well, such as less convenient access to the main source of drinking water and the possibility that drinking water was stored for longer in the home, did not have a major impact on the incidence of diarrhoeal disease.20 One possible explanation is that household wells, regardless of their arsenic content, continued to be used for personal hygiene.24 However, it appears that the microbial quality of low-arsenic water pumped from deep public wells might be higher than that from shallower household wells, though this should be determined more rigorously. It is possible that the greater physical separation between deep wells and major surface sources of microbial contamination, such as latrines and ponds, may have provided a protective effect.6,11 The incidence of childhood diarrhoea declined dramatically between 2005 and 2006, irrespective of water source (Fig. 2), but discussion of the reasons for this decline lie beyond the scope of this analysis.
Our study findings suggest that the approximately 165 000 deep tube wells that were installed throughout Bangladesh between 2000 and 2005 to reduce arsenic exposure had the added benefit of decreasing exposure to microbial pathogens. Given the high cost of deep wells, it is unlikely that many will be installed privately in the future. The question raised, therefore, is whether even households with shallow wells that are low in arsenic should also use deeper public wells instead as their main source of drinking water. Before making such a recommendation, however, it is important that the periodic testing of deep public wells for arsenic is considered. The limited time series data available indicate that arsenic concentrations in groundwater pumped from deep public wells have remained low in most cases. However, a small but significant proportion of these wells is likely to fail over time because the plastic pipes used may become broken or disconnected.25 Even a modest failure rate of 5% translates into a total of more than 8000 deep public wells throughout Bangladesh that could potentially provide water unsuitable for drinking to an estimated population of 2 000 000, assuming conservatively that 250 villagers on average obtain drinking water from each deep public well.18
The main limitation of this study is the relatively small number of households and deep public wells that were considered. The analysis of available data on diarrhoeal disease could be expanded to cover all 142 villages in Matlab if households were asked whether they use a deep tube well as their primary source of drinking water.
Acknowledgements
Data on cases of diarrhoea were collected by the International Centre for Diarrhoeal Disease Research in Bangladesh with unrestricted support from the following donors: the Australian Agency for International Development, the Government of the People’s Republic of Bangladesh, the Canadian International Development Agency, the Swedish International Development Cooperative Agency and the United Kingdom Department for International Development. Support from these donors is gratefully acknowledged. Veronica Escamilla, Brandon Wagner and Michael Emch are affiliated with the Carolina Population Center, University of North Carolina-Chapel Hill, Chapel Hill, USA.
Funding:
This study was supported by a grant from the National Institute of Environmental Health Sciences and the Fogarty International Center, number 5 R01 TW008066.
Competing interests:
None declared.
References
- 1.You D, Wardlaw T, Salama P, Jones G. Levels and trends in under-5 mortality, 1990–2008. Lancet. 2010;375:100–3. doi: 10.1016/S0140-6736(09)61601-9. [DOI] [PubMed] [Google Scholar]
- 2.Boschi-Pinto C, Lanata CF, Black RE. Maternal and child health: global challenges, programs, and policies. In: Ehiri J, editor. The global burden of childhood diarrhea. New York: Springer; 2010. pp. 225-243. [Google Scholar]
- 3.Ebi LK, Mills D, Smith JB. A case study of unintended consequences: arsenic in drinking water in Bangladesh. In: Ebi KL, Smith J, Burton I, editors. Integration of public health with adaptation to climate change: lessons learned and new directions. London: Taylor & Francis; 2005. pp. 72-90. [Google Scholar]
- 4.Van Geen A, Ahsan H, Horneman AH, Dhar RK, Zheng Y, Hussain I, et al. Promotion of well-switching to mitigate the current arsenic crisis in Bangladesh. Bull World Health Organ. 2002;80:732–7. [PMC free article] [PubMed] [Google Scholar]
- 5.Horneman A, van Geen A, Kent DV, Mathe PE, Zheng Y, Dhar RK, et al. Decoupling of As and Fe release to Bangladesh groundwater under reducing conditions. Part I: evidence from sediment profiles. Geochim Cosmochim Acta. 2004;68:3459–73. doi: 10.1016/j.gca.2004.01.026. [DOI] [Google Scholar]
- 6.Arsenic contamination of groundwater in Bangladesh (Final Technical Report WC/00/19). Keyworth: British Geological Survey; 2001.
- 7.Ahsan H, Chen Y, Parvez F, Zablotska L, Argos M, Hussain I, et al. Arsenic exposure from drinking water and risk of premalignant skin lesions in Bangladesh: baseline results from the Health Effects of Arsenic Longitudinal Study. Am J Epidemiol. 2006;163:1138–48. doi: 10.1093/aje/kwj154. [DOI] [PubMed] [Google Scholar]
- 8.Argos M, Kalra T, Rathouz PJ, Chen Y, Pierce B, Parvez F, et al. Arsenic exposure from drinking water, and all-cause and chronic-disease mortalities in Bangladesh (HEALS): a prospective cohort study. Lancet. 2010;376:252–8. doi: 10.1016/S0140-6736(10)60481-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Smith AH, Lingas EO, Rahman M. Contamination of drinking-water by arsenic in Bangladesh: a public health emergency. Bull World Health Organ. 2000;78:1093–103. [PMC free article] [PubMed] [Google Scholar]
- 10.Ahmed MF, Ahuja S, Alauddin M, Hug SJ, Lloyd JR, Pfaff A, et al. Epidemiology. Ensuring safe drinking water in Bangladesh. Science. 2006;314:1687–8. doi: 10.1126/science.1133146. [DOI] [PubMed] [Google Scholar]
- 11.Leber J, Rahman MM, Ahmed KM, Mailloux B, van Geen A. Contrasting influence of geology on E. coli and arsenic in aquifers of Bangladesh. Ground Water. 2011;49:111–23. doi: 10.1111/j.1745-6584.2010.00689.x. [DOI] [PubMed] [Google Scholar]
- 12.van Geen A, Ahmed KM, Akita Y, Alam MJ, Culligan PJ, Emch M, et al. Fecal contamination of shallow tubewells in Bangladesh inversely related to arsenic. Environ Sci Technol. 2011;45:1199–205. doi: 10.1021/es103192b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Howard G, Ahmed MF, Shamsuddin AJ, Mahmud SG, Deere D. Risk assessment of arsenic mitigation options in Bangladesh. J Health Popul Nutr. 2006;24:346–55. [PMC free article] [PubMed] [Google Scholar]
- 14.Luby SP, Gupta SK, Sheikh MA, Johnston RB, Ram PK, Islam MS. Tubewell water quality and predictors of contamination in three flood-prone areas in Bangladesh. J Appl Microbiol. 2008;105:1002–8. doi: 10.1111/j.1365-2672.2008.03826.x. [DOI] [PubMed] [Google Scholar]
- 15.Report on situation analysis of arsenic mitigation, 2009 Dhaka: Department of Public Health engineering & Japan International Cooperation Agency; 2010.
- 16.Zheng Y, van Geen A, Stute M, Dhar R, Mo Z, Cheng Z, et al. Geochemical and hydrogeological contrasts between shallow and deeper aquifers in two villages of Araihazar, Bangladesh: implications for deeper aquifers as drinking water sources. Geochim Cosmochim Acta. 2005;69:5203–18. doi: 10.1016/j.gca.2005.06.001. [DOI] [Google Scholar]
- 17.von Brömssen M, Jakariya M, Bhattacharya P, Ahmed KM, Hasan MA, Sracek O, et al. Targeting low-arsenic aquifers in Matlab Upazila, southeastern Bangladesh. Sci Total Environ. 2007;379:121–32. doi: 10.1016/j.scitotenv.2006.06.028. [DOI] [PubMed] [Google Scholar]
- 18.van Geen A, Ahmed KM, Seddique AA, Shamsudduha M. Community wells to mitigate the arsenic crisis in Bangladesh. Bull World Health Organ. 2003;81:632–8. [PMC free article] [PubMed] [Google Scholar]
- 19.Opar A, Pfaff A, Seddique AA, Ahmed KM, Graziano JH, van Geen A. Responses of 6500 households to arsenic mitigation in Araihazar, Bangladesh. Health Place. 2007;13:164–72. doi: 10.1016/j.healthplace.2005.11.004. [DOI] [PubMed] [Google Scholar]
- 20.Hoque BA, Hallman K, Levy J, Bouis H, Ali N, Khan F, et al. Rural drinking water at supply and household levels: quality and management. Int J Hyg Environ Health. 2006;209:451–60. doi: 10.1016/j.ijheh.2006.04.008. [DOI] [PubMed] [Google Scholar]
- 21.Mondal D, Polya DA, Giri AK, Banerjee M, Hegan A, Rodriguez-Lado L, et al. Mitigation of geogenic arsenic bearing groundwaters: assessing the importance of risk substitution arising from waterborne pathogens. Proceedings of the 19th Goldscmidt Conference, 21–26 June 2009, Davos, Switzerland Goldschmidt Conference Abstracts 2009:A893. [Google Scholar]
- 22.Black RE, Brown KH, Becker S, Yunus M. Longitudinal studies of infectious diseases and physical growth of children in rural Bangladesh. I. Patterns of morbidity. Am J Epidemiol. 1982;115:305–14. doi: 10.1093/oxfordjournals.aje.a113307. [DOI] [PubMed] [Google Scholar]
- 23.Emch M, Yunus M, Escamilla V, Feldacker C, Ali M. Local population and regional environmental drivers of cholera in Bangladesh. Environ Health. 2010;9:2. doi: 10.1186/1476-069X-9-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Esrey SA, Potash JB, Roberts L, Shiff C. Effects of improved water supply and sanitation on ascariasis, diarrhoea, dracunculiasis, hookworm infection, schistosomiasis, and trachoma. Bull World Health Organ. 1991;69:609–21. [PMC free article] [PubMed] [Google Scholar]
- 25.van Geen A, Trevisani M, Immel J, Jakariya M, Osman N, Cheng Z, et al. Targeting low-arsenic groundwater with mobile-phone technology in Araihazar, Bangladesh. J Health Popul Nutr. 2006;24:282–97. [PMC free article] [PubMed] [Google Scholar]